Abstract
Globally, 19 million women are estimated to undergo unsafe abortions each year. Age patterns of unsafe abortion are critical for tailoring effective interventions to prevent unsafe abortion and for providing post-abortion care. This paper estimates the incidence and the rate of unsafe abortion among women aged 15—44 in the Africa, Asia (excluding Eastern Asia), and Latin America/Caribbean regions, where a woman is likely to have close to one unsafe abortion by age 44. For developing regions as a whole, two-thirds of unsafe abortions occur among women aged 15—30 and 14% among women under age 20. The age pattern of unsafe abortions differs markedly between regions, however. Almost 60% of unsafe abortions in Africa are among women under age 25 and almost 80% are among women under 30. In Asia 30% of unsafe abortions are in women under 25 and 60% in women under 30. In Latin America and the Caribbean, women aged 20—29 account for more than half of unsafe abortions with almost 70% in women under 30. Over 40% of unsafe abortions among adolescents in the developing world occur in Africa, where one in four unsafe abortions takes place during adolescence. Young (under age 25) women in Africa, those over age 25 in Asia and women aged 20—35 years in Latin America and the Caribbean are in the greatest need of interventions to prevent unsafe abortion and good quality post-abortion care.
Résumé
On estime que, chaque année, 19 millions de femmes subissent un avortementàrisque dans le monde. Pour intervenir efficacement, il faut connaître la ventilation des avortements par groupes d’âge. L’article évalue l’incidence et le taux d’avortementàrisque chez les femmes de 15à44 ans en Afrique, en Asie (sauf l’Asie de l’Est), en Amérique latine et aux Caraébes, régions où une femme aura subi près d’un avortementàrisque avant 44 ans. Les deux tiers des avortementsàrisque concernent des femmes de 15à30 ans et de 14% des moins de 20 ans. Néanmoins, les âges diffèrent selon les régions. En Afrique, près de 60% des avortementsàrisque se produisent chez des femmes de moins de 25 ans et près de 80% chez les moins de 30 ans. En Amérique latine et aux Caraébes, les femmes âgées de 20à29 ans représentent plus de la moitié des avortementsàrisque, avec près de 70% chez les moins de 30 ans. Plus de 40% des avortementsàrisque chez les adolescentes de pays en développement se produisent en Afrique, où un avortementàrisque sur quatre est pratiqué sur une adolescente. En Afrique, les interventions doivent se centrer sur les femmes de moins de 25 ans, en Asie sur les plus de 25 ans, et en Amérique latine et aux Caraébes, sur les femmes de 20à35 ans.
Resumen
Se estima que, a nivel mundial,cada año aproximadamente 19 millones de mujeres se someten a abortos. Los patrones de edad del aborto inseguro son fundamentales para adaptar las intervenciones de manera eficaz. En este artáculo se calcula la incidencia y tasa de abortos inseguros en las mujeres de 15 a 44 años de edad en África, Asia (excluida Asia Oriental), Latinoamérica y el Caribe, donde es probable que cada mujer experimente un aborto inseguro antes de cumplir 44 años. Dos terceras partes de los abortos inseguros ocurren entre las mujeres de 15 a 30 años, y el 14% entre las menores de 20 años. No obstante, el patrón de edades de los abortos inseguros difiere marcadamente entre regiones. Casi el 60% de los abortos inseguros en África ocurre entre las mujeres menores de 25 años, y casi el 80% entre aquéllas menores de 30. En Asia, el 30% de abortos inseguros ocurre entre las mujeres menores de 25 y el 60% entre aquéllas menores de 30. En Latinoamérica y el Caribe, casi la mitad de los abortos inseguros se presentan en mujeres de 20 a 29 años; casi el 70% son menores de 30. Más del 40% de los abortos inseguros entre las adolescentes en los paáses en desarrollo ocurren en África donee uno de cuatro abortos inseguros ocurre entre las adolescentes. Para las poláticas y los programas, las intervenciones en África deben centrarse en aquéllas menores de 25; en Asia, en las mayores de 25; y en Latinoamérica y el Caribe, en las de 20 a 35 años.
Unsafe abortion is one of the most neglected problems of health care in developing countries and a serious concern for many women during their reproductive lives. When faced with an unintended pregnancy, women of all reproductive ages resort to abortion, and contrary to common belief, over 50% of women seeking abortion are married or live in stable unions and already have several children.Citation1 Citation2 Citation3 Citation4 Citation5 Citation6 Citation7 Many women use abortion to limit family size or space births, sometimes in the event of contraceptive failure or because of the lack of access to modern contraceptives.Citation8 Citation9 In all countries, access to induced abortion services is governed by the legal condition(s) under which abortion is allowed.Citation10 Citation11 Citation12 In some countries access is highly restricted while in others pregnancy termination is available on broad medical and social grounds or on request.Citation13
In countries where access to safe abortion is restricted, the situation is especially precarious for unmarried women, particularly adolescents, who have, in general, little or no access to reproductive information and counselling, and are frequently excluded from contraceptive services. The need for readily available information and services for family planning or abortion care is, however, not confined to young people. Women may be unaware that safe abortion services are legally available,Citation14 even under limited circumstances; they may lack the resources, time or decision-making power to avail themselves of such services; or the services may be inadequate to meet demand. Other inhibiting factors are negative attitudes of health care providers.Citation15 Citation16 Citation17 In some countries, the liberalisation of abortion laws has not been systematically followed by the availability of safe abortion services or the elimination of unsafe abortion.Citation18 Citation19 Citation20
The World Health Organization (WHO) defines unsafe abortion as a procedure for terminating an unintended pregnancy either by persons lacking the necessary skills or in an environment lacking the minimal medical standards, or both.Citation21 Unsafe abortions may also be self-induced using hazardous techniques or using pharmaceuticals without the involvement of a skilled provider or the necessary support. Unsafe abortion puts women’s health and lives at risk. Although the legality or illegality of the services may not be the defining factor of their safety, for the purposes of this paper abortions in countries where most abortions are illegal are defined as unsafe, except for those known to be legal.
WHO maintains a database and periodically issues estimated figures on regional and global incidence of unsafe abortion and related mortality. Recent estimates show that 19 million unsafe abortions (out of an estimated total of 46 million induced abortions) occur each year, 97% of them in the developing world, but important differentials exist between and within these regions.Citation22 Citation23 These estimates are presented in , with and without Eastern Asia. Unsafe abortion is negligible in Eastern Asia (China, Democratic People’s Republic of Korea, Mongolia, Republic of Korea) where abortion is legal and relatively accessible. Ratios and rates therefore better describe the situation of unsafe abortion in the developing world by excluding this demographically large region from calculations.Footnote*

While it is important to recognise the magnitude of the problem, these estimates do not indicate the ages of women having unsafe abortions, information that is critical to guide interventions for those most in need of services. Some past studies suggest that abortions among young women under age 20 in developing countries may have been as high as 4.4 million per year;Citation24 Citation25 incidence for other age groups has not been estimated. The main objective of this paper is therefore to analyse the extent of unsafe abortion by age and region in developing countries.
Estimating unsafe abortion by age and region: data and methods
This paper is based on information from some 300 studies published from 1985 to 2002 that look at unsafe abortion by age, identified through literature searches for the Department of Reproductive Health and Research database on unsafe abortion.Citation23 A review of these studies identified 69 that gave age distributions of women who had had an unsafe induced abortion and included information both from hospital and community surveys. The remaining studies, though they may have discussed abortion and age, did not give any breakdown of abortion by age.
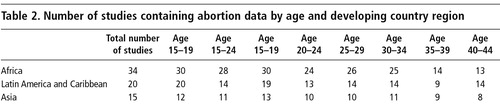
Among the 69 studies, 34 were from countries in Africa, 15 from Asia and 20 from Latin America and the Caribbean. In general, the reproductive age of 15—49 was covered, though not always by sequential five-year age groups (e.g. 15—19, 20—24, 25—29 and so on). In some studies the upper or youngest age groups were open-ended. Therefore, to make the groupings comparable between studies, data for ages below 15 were included in the 15—19 age group and those for over 44 in the 40—44 age group. This was the case for only a few studies and did not have a significant effect on figures by age.
The 69 studies cover a wide range of settings within each region, but no claim is made that they are fully representative of the regions. Age distributions were used for calculations as reported in the studies without modifications. A variety of age groupings were described in the studies included in the review; however, the age groups 15—19, 15—24 and 15—29 were particularly well represented, either as one age group or subdivided. The unsafe abortion incidence in age groups 20—24 and 25—29 can be calculated by subtraction, but the confidence intervals of the estimates for these important ages would be unknown in such application. However, the analysis of data by five-year age groups showed almost identical results, even though fewer data were available. It was therefore decided to carry out the estimates by five-year age groups, covering the full range of reproductive age cohorts, with confidence intervals that show the precision of the estimates. This is in line with the general demographic tradition of providing information on fertility and other indicators by five-year age groups. shows the availability of data by age group and region.
The method of estimation was as follows. Based on the data available by five-year age groups, and giving equal weight to each study, the average percentage of all unsafe abortions for each age group was calculated by region ( , column 2) together with the confidence interval of the mean. These were then applied to the estimated total number of unsafe abortions for women aged 15—44 () to arrive at the estimated number of unsafe abortions by age and region for the year 2000, together with the approximate range of the estimate (, column 3). Assuming that the incidence in Oceania was similar to that in Asia, we then aggregated the incidence for all developing country regions.
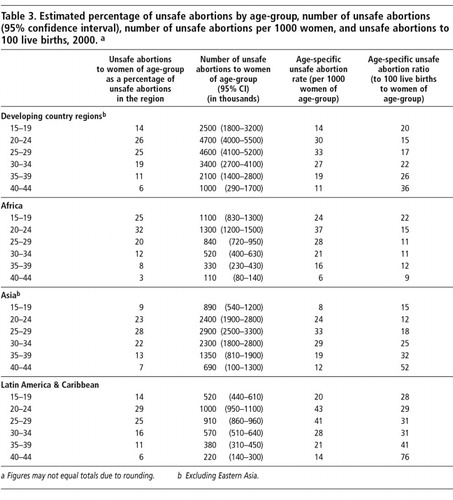
Finally, the estimated age-specific number of unsafe abortions by region was compared to the number of women and to live births in the corresponding age cohorts for the year 2000. The mid-year numbers of women by age were available directly from the UN Population Division,Citation26 while the age-specific number of live births for the year 2000 was calculated as the average of 1995—2000 and 2000—2005 from the same source. The number of unsafe abortions to 1000 women (age-specific unsafe abortion rate), and the number of unsafe abortions to 100 live births (age-specific unsafe abortion ratio) were calculated for each age cohort and by region. The results are shown in , columns 4 and 5. It should be borne in mind that the actual incidence of unsafe abortions remains unknown and difficult to measure.
The 15—29 age group contains the bulk of pregnancies and abortions in developing countries. The largest amount of information is also available for this age group and therefore allows for quite narrow confidence intervals. The estimates for the older age-groups show a wider range of estimates because there are fewer studies, implying less precision in the estimates. The estimated number of unsafe abortions and their distribution by age are important to highlight the magnitude of the unsafe abortion problem, while percentages, ratios and rates allow meaningful comparison between regions and age groups.
Estimated incidence of unsafe abortion by age and region
shows that of the 18.5 million unsafe abortions that take place each year in the developing world, approximately two-thirds are in women aged 15—29 and one-third in women over age 30. Importantly, 14% of all unsafe abortions in developing country regions are in women under the age of 20.
Figure 1 shows that for developing regions as a whole, unsafe abortions tend to peak in the age group 20—24 and then decline with age both as a percentage of all abortions (bars in Figure) and per 1000 women in each age group, as illustrated by the line with “•”. Typically 20—30 women per 1000 women of a given age group in the developing world turn to unsafe abortion each year. The rate increases up to age 30, whereupon it decreases for each subsequent age group. On the other hand, the ratio of unsafe abortions to live births (the line with “□) increases due to there being fewer births at older ages and thus a smaller and shrinking denominator.
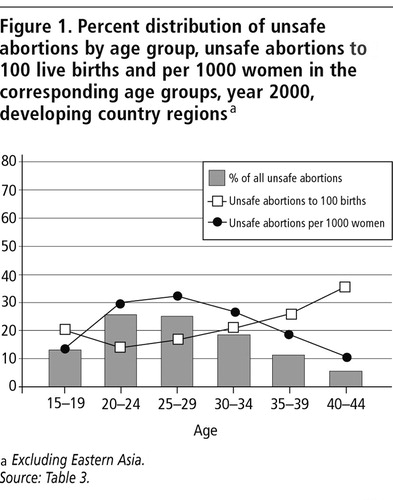
Overall, 19 unsafe abortions to 100 live births are estimated to occur in the developing world (), excluding Eastern Asia, or one unsafe abortion to every five live births. Most births occur at ages 20—24 and the line with “□in Figure 1 illustrates that despite the simultaneous peak in unsafe abortions, the ratio therefore is globally at a low in this age group, i.e. 15 to 100 live births or one to seven live births. The ratio thereafter increases with each consecutive age group: important proportions of ever fewer pregnancies are aborted. Except in the Africa region, the desire to limit or terminate childbearing with increasing age (and parity) results in high proportions of the relatively few pregnancies being aborted.
Specific features of the three regions
Figure 2 shows that in Africa almost 60% of unsafe abortions take place among 15—24 year-olds. In particular, the percentage in the group aged 15—19 is notably higher than in the other two regions, as shown by the bar for that age group. The trend in age-specific unsafe abortions to 100 live births (line with “□) is distinct for Africa: while initially high, the ratio decreases with increasing age. The unsafe abortion ratio in Africa remains constant at around 10 to 100 live births, starting with the 25—29 year-old age group.
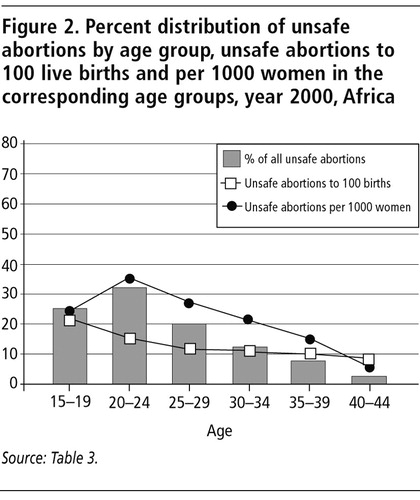
On the other hand, the unsafe abortion rate per 1000 women in Africa peaks among 20—24 year olds as illustrated by the line with “•”, whereupon it decreases for each subsequent age group, similar to other developing regions. The unsafe abortion rate in adolescents is, however, higher than for the other regions ().
The situation is distinctly different in Asia, as compared to Africa, where a relatively smaller percentage of unsafe abortions take place at young ages. Bars in Figure 3 show that unsafe abortions reach the highest point at age 25—29, later than in the other regions. At the youngest ages the ratio of unsafe abortions to live births (line with “□) is relatively modest, less than for Africa and Latin America. As in the other regions, it is lowest at ages 20—24, when the majority of births occur. It increases rapidly thereafter, which shows that reliance on unsafe abortion to limit childbearing supplements the natural effect of fewer pregnancies at older ages.
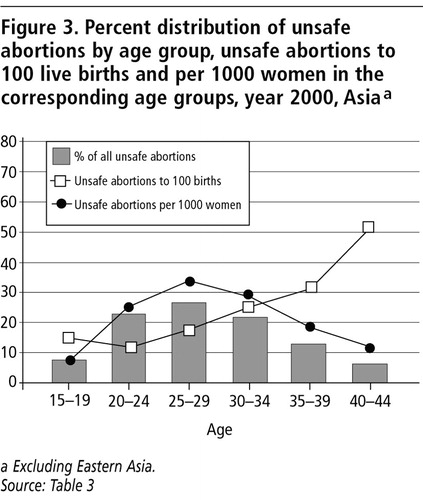
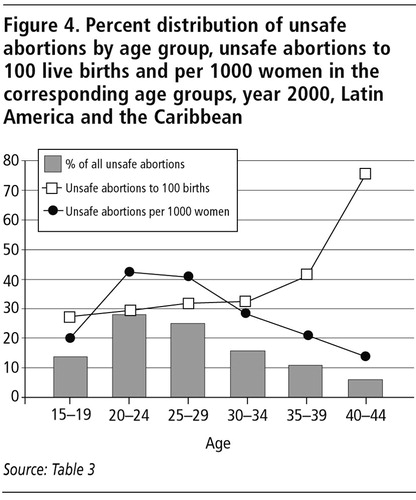
Figure 4 reflects a relatively high reliance on unsafe abortion in Latin America and the Caribbean. While contraceptive use is high in the region, unsafe abortions also contribute to the lowest level of fertility among the three developing regions.Citation22 Citation27 The proportion of unsafe abortions is highest at age 20—24, decreasing thereafter. The age-specific unsafe abortion ratio to 100 live births (line with “□ is higher for Latin America at all ages compared to the other regions (). The ratio remains at a relatively high and constant level, around 30 to 100 live births, increasing at older ages, reaching almost 80 to 100 live births at age 40—44. The ratios increase by age because of fewer births in the older age groups, a result of decreasing fertility and greater reliance on sterilisation at older ages in the region. This seems to indicate that to regulate fertility, unsafe abortion is initially used to space births and later to limit childbearing. The line with “x” shows that the unsafe abortion rate per 1000 women of any age group reaches a high of over 40 in women in their 20s in Latin America and the Caribbean, which supports the notion that unsafe abortion is used particularly for spacing purposes in those age groups.
The total unsafe abortion rate
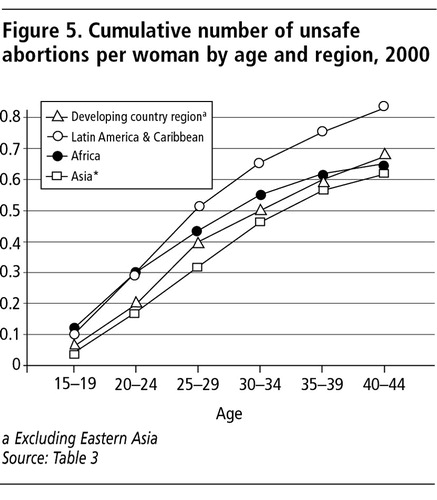
Another summary measure of the unsafe abortion situation is by calculating the total unsafe abortion rate. This measure is the equivalent for unsafe abortions to the total fertility rate, and refers to the cumulative number of unsafe abortions per woman by the age of 44. The age-specific abortion rates derived from were converted, by summing and multiplying by five (for the width of the age-group) to arrive at the total unsafe abortion rate. These calculations show that by age 44, on average a woman in Latin America and the Caribbean is expected to have 0.8 unsafe abortions, compared to 0.7 in Africa and 0.6 in Asia (Figure 5 ).
Discussion
Each year approximately 210 million women become pregnant worldwide, of whom 132 million go on to have a live birth. Millions of pregnancies are, however, unplanned. Some are carried to term; others end in spontaneous or induced abortion. It is estimated that 46 million pregnancies are terminated each year, 27 millionCitation28 safely and 19 millionCitation23 unsafely.
Most efforts thus far have focused on estimating the total incidence of unsafe abortion by region or sub-region. Studying the age pattern of unsafe abortion can indicate which age-groups are most in need of attention with regard to information, access to contraceptives and safe abortion services as well as services for complications of unsafe abortion.
The relatively high level of unintended pregnancies and unsafe abortions among young women under the age of 25 in Africa, compared to other regions, requires urgent action. Over 40% of unsafe abortions among adolescents in the developing world occur in Africa, and 25% of all estimated unsafe abortions in Africa are among adolescents. These data reflect both a general lack of information and access to contraceptive services. The risk of maternal mortality for young women, not yet ready for motherhood, is estimated to be several times higher than for adult women.Citation29 Because of fewer resources and the lack of support, this may be further augmented in the case of unsafe abortion.
The age pattern of unsafe abortions differs markedly between regions. Almost 60% of unsafe abortions in Africa are among women under age 25 and almost 80% are among women under age 30. This contrasts with Asia where 30% of unsafe abortions are in women under age 25 and 60% are in women under age 30. In Latin America and the Caribbean women aged 20—29 account for more than half of all unsafe abortions with almost 70% in women under age 30.
The elevated incidence of unsafe abortion in Africa in the youngest age group is not surprising; surveys have shown that sexual initiation is earlier in African women than elsewhere: 61% are sexually active by age 18 and 79% by age 20 compared to 38% and 58% in Latin America and the Caribbean.Citation30 Much of the sexual activity among adolescents and young adults is unprotected, and initiation of sexual activity more often takes place before marriage.Citation30 Surveys also show that among those with primary level or no education the percentage of adolescent girls who are sexually active before age 18 is higher than among those with secondary education or higher.
On average, women in developing countries are likely to have close to one unsafe abortion before reaching the end of their reproductive years. Thus, efforts must be made to prevent unintended pregnancy and to provide contraceptive information and services for women of all ages. However, our analysis suggests that interventions should be tailored for the different age groups in the different world regions. In Africa, the focus should be on women below age 25, whereas in Asia the focus should be on women over age 25. In Latin America and the Caribbean, the focus of interventions should be on women aged 20—35. In all regions and for all ages, unsafe abortions need to be prevented for they exert a heavy toll on the lives of women.
Notes
* Hence, for the remainder of this paper “developing regions”, “developing country regions” “Asia” do not include Eastern Asia.
Related Research Data
References
- LC Remez. Confronting the reality of abortion in Latin America International Family Planning Perspectives. 21: 1995; 32–36.
- F Pardo, G Uriza. Estudio de morbilidad y mortalidad por aborto en 36 instituciones de Bolivia, Colombia, Perú y Venezuela Revista Colombiana de Obstetricia y Ginecologáa. 42(4): 1991; 287–289.
- Encuentro de Investigadores sobre Aborto Inducido en América Latina y el Caribe. Representaciones Sociales y Movimientos Sociales. 1994; Universidad Externado de Colombia: Santafé de Bogotá, D.C. Colombia.
- M Barrère. Avortement Demographic and Health Surveys, Direction Générale de la Statistique et des Etudes Economiques (Gabon). Enquete Démographique et de Santé Gabon 2000. 2001; Direction Générale de la Statistique et des Etudes Economiques (Gabon), UNDP, Macro International Inc: Calverton MD.
- National Statistical Office of Mongolia, United Nations Population Fund. National Report: Mongolia, Reproductive Health Survey 1998. 1999; Ulaanbaatar, Mongolia National Statistical Office.
- National Center for Disease Control (NCDC, Georgia), US Centers for Disease Control and Prevention (DRH/CDC), UNFPA, USAID, UNICEF, UNHCR, AIHA. Women’s Reproductive Health Survey, Georgia, 1999—2000. Final Report. 2001; NCDC, CDC: Tbilisi, Republic of Georgia and Atlanta GA, USA, 53–78.
- A Bankole. Characteristics of women who obtained induced abortion: a worldwide review International Family Planning Perspectives. 25(2): 1999; 68–77.
- CF Westoff, LH Ochoa. Unmet Need and the Demand for Family Planning. (Comparative Studies No.5). 1991; Macro International Inc: Columbia MD.
- CF Westoff, A Bankole. Unmet Need: 1990—1994. (Comparative Studies No.16). 1995; Macro International Inc: Calverton MD.
- United Nations Department of Economic and Social Affairs Population Division. Abortion Policies: A Global Review. Vol. I. Afghanistan to France. 2001; United Nations: New York.
- United Nations Department of Economic and Social Affairs Population Division. Abortion Policies: A Global Review. Vol. II. Gabon to Norway. 2001; United Nations: New York.
- United Nations Department of Economic and Social Affairs Population Division. Abortion Policies: A Global Review. Vol. III. Oman to Zimbabwe. 2001; United Nations: New York.
- World Health Organization. Safe Abortion: Technical and Policy Guidance for Health Systems. 2003; WHO: Geneva.
- K Iyengar, SD Iyengar. Elective abortion as a primary health service in rural India: experience with manual vacuum aspiration Reproductive Health Matters. 10(19): 2002; 54–63.
- A Langer. Emergency contraception in Mexico City: what do health care providers and potential users know and think about it? Contraception. 60(4): 1999; 233–241.
- J Kasule. Abortion: attitudes and perceptions of health professionals in Zimbabwe Central African Journal of Medicine. 45(9): 1999; 239–244.
- E Djohan. The attitudes of health care providers towards abortion in Indonesia. AI Mundigo, C Indriso. Abortion in the Developing World. 1999; WHO: Geneva.
- C Ahiadeke. Incidence of induced abortion in Southern Ghana International Family Planning Perspectives. 27(2): 2001; 96–101.
- AR Nanda. Abortion services and health care ISSRF Newsletter. 3: 2000; 1–4.
- A Harrison. Barriers to implementing South Africa’s Termination of Pregnancy Act in rural KwaZulu/Natal Health Policy and Planning. 15(4): 2000; 424–431.
- World Health Organization. The Prevention and Management of Unsafe Abortion. Report of a Technical Working Group. Geneva, April 1992. WHO/MSM/92.5. 1992; WHO: Geneva.
- E Áhman, I Shah. Unsafe abortion: worldwide estimates for 2000 Reproductive Health Matters. 10(19): 2002; 13–17.
- E Áhman, I Shah. Unsafe Abortion. Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2000. 4th ed, 2004; WHO: Geneva.
- AP McCauley. Meeting the needs of young adults Population Reports. 23(3): 1995; 1–42.
- AA Olukoya. Unsafe abortion in adolescents International Journal of Gynecology & Obstetrics. 75(2): 2001; 137–147.
- Department for Economic and Social Information and Policy Analysis. World Population Prospects: The 2000 Revision. 2001; United Nations: New York.
- Áhman E, Shah I. Contraceptive use, fertility and unsafe abortion in developing countries. (Submitted for publication, 2004)
- S Singh, SK Henshaw, K Berentsen. Abortion: a worldwide overview. AM Basu. The Sociocultural and Political Aspects of Abortion: Global Perspectives. 2003; Praeger Publishers: Westport CT, 15–48.
- World Health Organization. Issues in Adolescent Health and Development: Adolescent Pregnancy. Geneva: WHO. (Forthcoming 2004).
- United Nations Commission on Population and Development. World Population Monitoring 2002. Reproductive Rights and Reproductive Health: Selected Aspects. 2003; United Nations: New York.