Abstract
Second trimester abortion has been legal in the Netherlands since 1984. Factors influencing second trimester abortion in the Netherlands may be different from those that play a role in first trimester abortions. This is important for professionals in counselling and education. In this paper national registration data are used to complement data from a small, qualitative, exploratory file study conducted in three clinics, on the factors associated with second trimester abortions. In 2006, 6.6% of all abortions registered in the National Abortion Registry took place after 12 weeks of gestation. In the qualitative data, relationship problems with the partner were mentioned more frequently as the main reason for second trimester abortions than for first trimester abortions. Factors associated with delay in obtaining an abortion were young age, inability to recognise pregnancy, ambivalence towards the pregnancy, having to travel to the Netherlands for abortion and to a lesser extent being an immigrant from specific countries. Information should be provided for young women and women from specific immigrant groups on early awareness of pregnancy, contraception and reduction of fear about seeking abortion and sexuality education should be provided.
Résumé
Aux Pays-Bas, l'avortement du deuxième trimestre est légal depuis 1984. Les facteurs qui l'influencent dans ce pays peuvent différer de ceux qui jouent un rôle dans l'avortement du premier trimestre. Cette distinction est importante pour les conseillers et les éducateurs. Dans cet article, les données de l'enregistrement national complètent les résultats d'une petite étude qualitative et exploratoire menée dans trois dispensaires sur les facteurs associés aux avortements du deuxième trimestre. En 2006, 6,6% des avortements recensés dans le registre national des avortements avaient eu lieu après 12 semaines de gestation. Dans les données qualitatives, les problèmes de relation avec le partenaire étaient mentionnés plus fréquemment comme principale raison de l'avortement du deuxième trimestre que du premier trimestre. Les facteurs associés au retard pour obtenir un avortement étaient le jeune âge, l'incapacité à déceler la grossesse, l'ambivalence à l'égard de la grossesse, l'obligation de se rendre aux Pays-Bas pour y avorter et, dans une moindre mesure, la qualité d'immigrante originaire de certains pays. Les jeunes femmes et les femmes issues de certains groupes d'immigrants doivent être informées des signes précoces de la grossesse et de la contraception ; il faut réduire leurs craintes de demander un avortement et dispenser une éducation sexuelle.
Resumen
Desde 1984, el aborto en el segundo trimestre es legal en los Países Bajos, donde los factores que influyen en éste pueden ser diferentes a aquellos relacionados con el aborto en el primer trimestre. Esto es importante para los profesionales en consejería y enseñanza. En este artículo se utilizan datos del registro nacional para complementar los datos de un pequeño estudio exploratorio cualitativo, realizado en tres clínicas, sobre los factores asociados con el aborto en el segundo trimestre. En 2006, el 6.6% de todos los abortos registrados en el Registro Nacional de Abortos ocurrieron después de 12 semanas de gestación. En los datos cualitativos, los problemas en la relación de pareja fueron mencionados como el motivo principal para tener un aborto en el segundo trimestre, con más frecuencia que para el aborto en el primer trimestre. Los factores asociados con la demora en obtener un aborto fueron: temprana edad, incapacidad de reconocer el embarazo, ambivalencia hacia el embarazo, tener que viajar a los Países Bajos para tener un aborto y, en menor medida, ser inmigrante de determinado país. Las mujeres jóvenes y mujeres de determinados grupos de inmigrantes deben recibir información sobre el reconocimiento temprano del embarazo, la anticoncepción y la reducción del temor de buscar servicios de aborto y educación sexual.
In the Netherlands, abortion has been permitted on request since 1984 up to 22 weeks of pregnancy, if performed by a physician in a hospital or a clinic licensed to perform abortions.Citation1 A five-day waiting period is required between the woman's first contact with a doctor and the abortion. Even before the law was passed, in fact since 1971, safe first trimester abortion was already practised and second trimester abortions have been possible since the late 1970s. Although not yet legal in the strict sense, abortion was condoned by public opinion and the government. Of the 16 clinics that currently offer abortions, eight have a special permit to perform second trimester abortions.
There are no financial barriers to obtaining an abortion for residents of the Netherlands. All residents have government-sponsored national health insurance, which covers the cost of abortions performed in clinics. Payment for abortions under this system has not resulted in a rise in abortions, but has caused a shift in the balance of providers from hospitals to clinics.Citation1 By 1992, 91% of all abortions were being carried out in clinics.Citation2 Women living abroad who come to the Netherlands to have an abortion must cover the financial costs themselves.
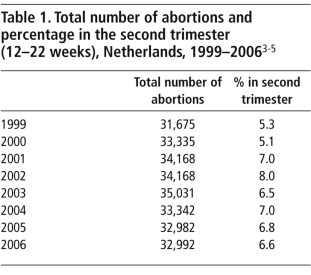
For decades, the Netherlands has been known for its low abortion rate. Over the last five years, the overall abortion rate stabilised at around 8.6 abortions per 1,000 women of reproductive age.Citation3–5 Table 1 shows the annual number of abortions together with the proportion of second trimester abortions. It includes both women living in the Netherlands and women living abroad who had abortions in the Netherlands (n=4,508 in 2006). In the period 1999–2006 the proportion of second trimester abortions has fluctuated between 5–8%.
As in other countries where abortion is legal, late abortions have always been a topic of heated discussion in the Netherlands. From both the medical and the religious side, there is debate over the question of why there is a need for second trimester abortions and what can be done to lower the number. Little is known about the factors influencing second trimester abortion in the Netherlands, however, but it is possible that they are different from the factors that play a role in first trimester abortions.
A study of the factors influencing the percentage of second trimester abortions has not been done since the early 1980s.Citation6 Since that time, a lot has changed. The abortion rate is higher, the abortion services have changed and the composition of the female population is very different. It is therefore valuable to get renewed insight into the factors associated with second trimester abortion.
This paper seeks to answer the following questions: What are the most important motivations and reasons for delay of women who have had a second trimester abortion? Are there specific sub-groups of women who are more likely to have later abortions? Are there aspects of abortion service delivery that cause delays in obtaining an abortion until the second trimester?
Methods
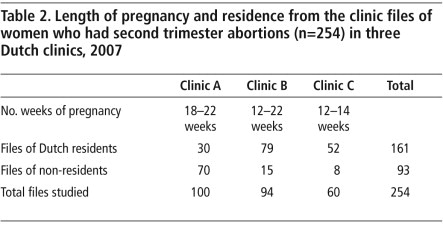
To answer these questions, we used two data sources. The motivations and reasons for delay were explored by means of a small-scale, exploratory study of clinic files. Consecutive files of women at three different clinics in 2007 were studied to see what factors emerged from the personal histories. The length of pregnancy of the women whose pregnancies were terminated in the three clinics and the number of files analysed in each clinic are found in Table 2. In clinic A, about half the women come to the Netherlands from abroad especially to have a second trimester abortion. From the clinic files, information on 100 women with a pregnancy of 18+ weeks was collected in the last three months of 2007, of whom 70 came from abroad. Clinic B serves mostly Dutch residents. Here data were collected on 94 women with an abortion between 12–22 weeks of pregnancy in the last three months of 2007, 15 of whom came from abroad. Clinic C only terminates early second trimester abortions, up to 14 weeks of pregnancy. This clinic provided data on 60 women in the second half of 2007, eight of whom came from abroad. The three clinics were selected to participate in the study on grounds of willingness to make the files and their time available.
Information was collected about age, duration of pregnancy, reason for wanting to terminate the pregnancy, referral time and the reason why the abortion was delayed. All the women whose files were studied were aged 14–43 years. Almost one third (28%) of them were under 20 years of age. In the national statistics for all abortions, about 14% are under the age of 20. In contrast, the older age group is under-represented: 4% of the women in the group studied were more than 40 years old, while for all abortions in the Netherlands this figure was 8% in 2006.
The other source of data used was the Landelijke Abortus RegistratieCitation4 (LAR, National Abortion Registry). Data on abortions are submitted on a quarterly basis to the Ministry of Health by all abortion providers, both specialised abortion clinics and general hospitals. In 2006, 94.3% of all abortions were performed in clinics and 5.7% in hospitals. In addition to this registry data, 14 of the 16 clinics provide additional data which are collected by the Rutgers Nisso Groep and reported annually. The latter dataset covers 86% of all abortions of Dutch residents and 91% of the abortions of women from abroad that are carried out in the Netherlands. Data from two clinics and the hospitals are not included in the LAR. The latter data cannot be analysed because they are reported in aggregate tables only.
Reasons for abortion and why in the second trimester
The most frequent reason given for having a second trimester abortion by Dutch residents (n=161) was the relationship with the partner (40%). Either the women had no stable partner, or their partner had left them or was aggressive (some of them had been raped). This was closely followed by “too early to have children” (35%). Either the woman considered herself too young or it was too early in the relationship to have children together. The third most frequent reason was that her family was complete (11%). Other reasons were much less frequent, including spacing of children, study/work, no wish for children, older age, health or financial problems. Often several reasons were mentioned, for example, too early, no finances, still a student and no stable relationship were often combined.
In the group of women who travelled to the Netherlands for an abortion (n=93), the most frequent reason for the abortion was that the pregnancy was too early (42%). Almost a quarter (23%) said that there were relationship problems, 10% said their family was complete, and three women had had an abnormal antenatal screening result.
By comparison, the main or most influential reason for abortion in the Netherlands, reported by a national sample of Dutch abortion patients in 2005, was financial difficulties. It was most often mentioned as one of the reasons, by 46.7% of the women, and mentioned as the most important factor by 11.6% of the women. The family already being complete was the second most influential reason (mentioned respectively by 23.9% and 11.6%) A broken-off relationship with the partner was mentioned by 5.1% of this group of women.Citation7
A second trimester abortion may be caused either by not being aware of the pregnancy or not being able to reach a decision to terminate the pregnancy or other reasons for delay. Since there are no official data about the reasons why women present in the second trimester for abortion, we searched the files for indications why.
Of the 177 women who mentioned a reason, 99 said they were late in finding out they were pregnant. The most frequently mentioned reasons were that they were still having periods because they had used the pill inconsistently, with blood loss as a result, or they had used the injectable and were used to have no periods. Others had hoped that their menstruation would still come.
Forty-eight of the 177 women had postponed making a decision because they were ambivalent about what to do. These women often had problems in their relationship with their partner. Similar reasons for delay were found in a 2005 study in England and Wales by Ingham et al.Citation8 The main difference is that in the Netherlands, the proportion of second trimester abortions has been consistently lower and, unlike in England and Wales, service-related delays play a minor role.
A few women (mostly from abroad) did not know where to go for an abortion or had a long delay in their country of origin, and for ten women there were reasons such as needing time to collect money for the abortion, fetal anomalies diagnosed only late in the pregnancy, and fear of a partner, who was against the abortion. In this group the maximum period a woman waited before coming to a decision to have an abortion was 90 days.
Risk factors for second trimester abortions
Data from the National Abortion Registry in 2006 (Table 3) show that age, country of residence and country of origin are individual characteristics associated with a higher risk for second trimester abortion.
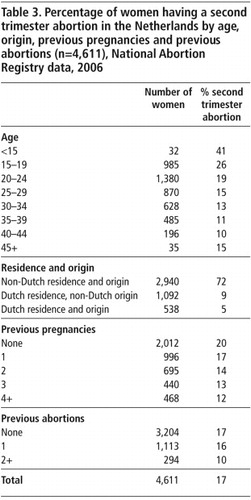
Over the years there has been a change in the behaviour of teenagers in the Netherlands. Sexual initiation starts a little earlier than before.Citation9 At the same time the average age at which Dutch women have their first child is higher than ever, currently just under age 30. So, the period in which most girls are sexually active but do not want to become pregnant has become substantially longer. DataCitation1 show that teenagers had an abortion rate of 5.0 per 1,000 women in 2006 (which is much lower than the abortion rate for all age groups. which is 8.6). The proportion of abortions in teenagers that are second trimester abortions is much higher than for women that are older (Table 3). The proportion decreases with age but rises slightly for women aged 45 or more, who might think they are menopausal and therefore do not recognise they are pregnant.
In Table 3, the women who had an abortion in 2006 are divided into three groups: those from other countries, those resident in the Netherlands but not of Dutch origin, and those of Dutch origin resident in the Netherlands. There is a very high proportion of women from other countries who had second trimester abortions, which they could not access in their own countries. Since the late 1970s, women from countries with more restrictive abortion laws have been travelling to the Netherlands for second trimester abortions. The proportion of foreign women needing to do this was declining, but the number has stabilised over the past five years. In 2006, 13.6% of all abortion patients were residents of another country.
The women of non-Dutch origin living in the Netherlands had a slightly higher proportion of second trimester abortions than the women of Dutch origin, especially those from other European countries (16%). Women from Asia, Turkey and Morocco were comparable to the Dutch (5–6%).
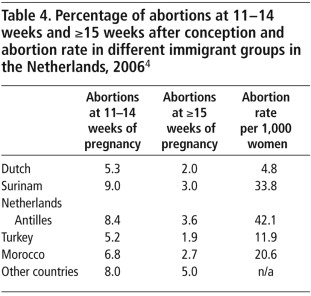
The influx of immigrant women from the Netherlands Antilles and Surinam, as well as from Mediterranean countries and Africa has changed the composition of the population. In the 1990s a large number of single teenage asylum seekers came to the Netherlands. This influx has now dwindled due to new, restrictive regulations. Together with immigrants from non-western countries they now represent around 12.7% of women of reproductive age.Citation10 These women, especially those from the Netherlands Antilles, Surinam, Africa and Turkey have a slightly higher to a much higher overall abortion rate than the native Dutch population (Table 4). Most but not all of these groups also have a somewhat higher percentage of second trimester abortions.
Risk of second trimester abortion decreased with a higher number of previous pregnancies and/or previous abortions. Of course, this is strongly related to age. When a woman is older she has an higher chance of having experienced pregnancy or abortion. This effect could therefore be due to age. A logistic regression analysis using all four variables, in order to control for the relations between them, with the dependent variable being a second trimester abortion found that all four variables: age, country of origin, previous pregnancies and previous abortions influenced the chances of a second trimester abortion (data not shown). Thus, previous experience of pregnancy and/or abortion lowers the risk for a second trimester abortion.
Service delivery as a possible cause of delay
Generally, access to the Dutch facilities is very good. This is demonstrated by the fact that in 2006, one third of all abortions took place at under four weeks gestation. Not only are most women quickly aware they may be pregnant, the majority decide rather promptly whether the pregnancy is unwanted and find their way to a clinic. However, with the data available to us, we have no way of checking whether or not this is also the case for women going to a clinic for a second trimester abortion. Not all clinics offer second trimester abortions. Our experience is that referral to another clinic may cause a delay of about a week. This situation is different from the USA where lack of access is one of the main reasons for delay.Citation11
It has been repeatedly suggested in the international debate that the availability of early medical abortion will lower the percentage of women with a second trimester abortion. Medical abortion is offered in the Netherlands to women in the first 49 days of pregnancy, or 35 days after conception. This method is slowly becoming more popular in the Netherlands and there is a shift towards very early abortions (about half of all abortions take place before 35 days of conception), but only 11% of all abortions are early medical abortions. A relationship between the introduction of early medical abortion and a decreasing demand for second trimester abortion is not seen in the Dutch registry data.
Late second trimester abortions in hospitals in the Netherlands are often performed because of fetal anomalies found in antenatal screening post-20 weeks gestation. Reporting of these abortions is obligatory and data are sent quarterly to the Ministry of Health, together with data on abortions for social reasons. In 2006, 8.1% (n=404) of all second trimester abortions were done in hospitals and this proportion has been increasing over the last years. However, there is no information available about the reason for abortion in these data and according to the Evaluation Report of the Abortion Law in 2005,Citation5 hospital abortion data are often insufficient in comparison with the clinics:
“Some hospitals have mentioned not reporting abortions carried out on the grounds of antenatal diagnosis; according to them, this trajectory is different from abortion on social grounds and therefore abortion after antenatal diagnosis is not subject to the obligatory registration according to the abortion law. Other hospitals make a distinction on the grounds of method of treatment: a curettage is reported within the framework of the abortion law but an induction of labour is held to be a premature birth and is not reported. One hospital recently started to report abortions after antenatal diagnosis…” Citation5 [our translation]
Since 2006, antenatal screening has become more widely available and since 2007 it has become policy in the Netherlands that it should be offered to all pregnant women, not just those over 36 years of age, and paid for under the national health insurance schemeCitation12. There is a lot of debate as to whether more pregnancies will in future be terminated on the grounds of fetal abnormalities (Hajo Wildschut, Personal communication, February 2008). According to the Ministry of Health, the increase in second trimester abortions in hospitals is probably due to the development of new antenatal screening technology and greater use of screening. However, in view of the lack of reliable data and no information on the views of the hospitals mentioned above, it could also be that the increase is at least partly due to improved reporting.
Discussion
It is important to note that access to early medical abortion does not appear to have an influence on the number of second trimester abortions in the Netherlands. This is important in response to anti-choice assertions, which are not based on evidence, that it does.
Although the group of women in our exploratory study are not necessarily representative of all women with second trimester abortions in the Netherlands, the information presented is interesting because recent literature on this subject, apart from National Abortion Registry data, is scarce. Our exploratory study shows that women who are having second trimester abortions fall into two main categories. The first is women already in the second trimester of pregnancy coming to the Netherlands from other countries, who were unable to access a second trimester abortion in their own country. Until the countries they come from make it possible for women to get a second trimester abortion at home, these abortions will continue to be needed and the Netherlands, alongside Spain, England and Wales, have an important responsibility in Europe in this regard.
The second group are pregnant women resident in the Netherlands who have relationship problems, or whose circumstances change, or who learn through antenatal diagnosis of fetal anomalies, or who have few or no warning signs of pregnancy (or do not recognise them as such), or who deny they are pregnant, or for whom the decision whether to continue the pregnancy is very difficult to make. There is only so much that can be done to mitigate any of these factors. What can be done as part of health and sexuality education is for information to be provided on coping with relationship problems, early awareness of pregnancy, use of contraception, where to go for abortion and find counselling if help is needed to make a decision, which will hopefully also lead to a reduction in fear about seeking abortion. Young women, women from immigrant groups and women without any experience of being pregnant are especially likely to benefit from this.
Acknowledgements
We want to thank our colleagues from the participating clinics Mirjam Denteneer and Anke Thijssen for supplying us with their data.
References
- Netherlands abortion policy. Population Policy Data Bank. Population Division, UN Department for Economic and Social Affairs. At: <www.un.org/esa/population/publications/abortion/doc/nether.doc. >.
- HP David, J Rademakers. Lessons from the Dutch abortion experience. Studies in Family Planning. 27(6): 1996; 341–343.
- Inspectie voor de Gezondheidszorg. Annual statistics on pregnancy termination [Dutch]. 2007; Inspectie voor de Gezondheidszorg: Den Haag.
- C Wijsen. Landelijke Abortus Registratie 2006 [National Abortion Registry]. 2008; Rutgers Nisso Groep: Utrecht.
- C Wijsen, L Van Lee, H Koolstra. Abortion in the Netherlanda 2001–2005 [Dutch]. 2007; Rutgers Nisso Groep: Utrecht, 66.
- E Ketting. Second trimester abortion as a social problem: delay in abortion seeking behaviour and its causes. MJND Kierse. Second Trimester Pregnancy Termination. 1982; Martinus Nijhoff: The Hague, 12–19.
- Visser MRM, Janssen AJGM, Enschedé M, et al. Evaluation of the law on pregnancy termination. [Dutch]. Den Haag: ZonMw, 2005. p.83/134.
- R Ingham, E Lee, SJ Clements. Reasons for second trimester abortions in England and Wales. Reproductive Health Matters. 16(31 Supplement): 2008; 18–29.
- H de Graaf, S Meijer, J Poelman. Sex under 25 years of age [Dutch]. 2005; Rutgers Nisso Groep: Utrecht, 34–35.
- J Garssen, H Nicolaas. Recent trends in fertility of non-western immigrant women. Population trends in the first quarter of 2006 [Dutch]. 2006; Centraal Bureau voor de Statistiek: Den Haag, 15–31.
- EA Drey, DG Foster, RA Jackson. Risk factors associated with presenting for abortion in the second trimester. Obstetrics and Gynecology. 107: 2006; 128–135.
- Ministerie von Volksgezondheid, Welzijn en Sport. Prenatal screening [Dutch]. <www.minvws.nl/dossiers/prenatale-screening/default.asp. >. Accessed 21 March 2008.