Abstract
There will always be women who need abortions after 12 weeks of pregnancy, and their reasons are often compelling. Although second trimester abortions carry relatively more risks than first trimester abortions, abortion is still very safe throughout the second trimester if done in safe conditions. This paper is about law and policy on second trimester abortions, which are allowed on more restrictive grounds than first trimester abortions in most countries, if at all. It focuses on countries where most or at least some second trimester abortions are allowed, including in Europe, where many women are still forced to travel for second trimester abortions, and countries in the developing world, where most second trimester abortions remain unsafe. The need for second trimester abortion should be met in a safe, timely and sympathetic manner. Abortion should be legal at the woman's request up to 24 weeks and on therapeutic grounds after that, and no other barriers or hurdles should be imposed on women seeking second trimester abortion. In-depth, country-based research is needed, to bring out the facts on second trimester abortion, as evidence of why it should be treated as a legitimate form of women's health care and supported in public health policy.
Résumé
Il y aura toujours des femmes qui devront avorter après 13 semaines de grossesse, pour des raisons souvent impérieuses. Même si les avortements du deuxième trimestre comportent relativement plus de risques que les avortements du premier trimestre, ils sont encore très sûrs tout au long du deuxième trimestre s'ils sont pratiqués dans de bonnes conditions. Cet article décrit la législation et les politiques sur les avortements du deuxième trimestre, qui sont autorisés, le cas échéant, pour des motifs plus restrictifs qu'au premier trimestre dans la plupart des pays. Il se concentre sur des pays où la plupart ou du moins quelques avortements du deuxième trimestre sont autorisés, notamment en Europe, où beaucoup de femmes sont encore obligées de voyager pour avorter au deuxième trimestre, et des pays en développement, où la plupart des avortements du deuxième trimestre demeurent non médicalisés. Il faut satisfaire la demande d'avortements du deuxième trimestre en toute sécurité, ponctuellement et avec bienveillance. L'avortement devrait être légal à la demande de la femme jusqu'à 24 semaines et passé ce délai pour raisons thérapeutiques, et aucun autre obstacle ne devrait être imposé aux femmes souhaitant avorter au deuxième trimestre. Une recherche approfondie, à base nationale, est nécessaire pour rassembler des données sur l'avortement du deuxième trimestre qui montreront qu'il doit être traité comme une forme légitime de soins de santé féminine et soutenu dans la politique de santé publique.
Resumen
Siempre habrá mujeres que necesiten abortos después de 12 semanas de embarazo, y sus motivos a menudo son convincentes. Aunque el aborto en el segundo trimestre acarrea relativamente más riesgos que el del primer trimestre, el aborto continúa siendo muy seguro a lo largo del segundo trimestre si se efectúa en condiciones seguras. Este artículo trata sobre las leyes y políticas de aborto en el segundo trimestre, el cual, cuando es permitido, es por motivos más restrictivos que el de primer trimestre en la mayoría de los países. Se centra en los países donde se permite la mayoría, o por lo menos algunos de los abortos en el segundo trimestre, como en Europa, donde muchas mujeres aún se ven forzadas a viajar para tener abortos en el segundo trimestre, y en países en desarrollo, donde la mayoría de los abortos en el segundo trimestre continúan siendo inseguros. La necesidad de aborto en el segundo trimestre debe atenderse de manera segura, oportuna y comprensiva. El aborto debería ser legal a petición de la mujer, hasta las 24 semanas y por motivos terapéuticos de ahí en adelante, y no se debe imponer ninguna otra barrera u obstáculo en las mujeres que buscan servicios de aborto en el segundo trimestre. Se necesitan investigaciones a profundidad en los países de estudio a fin de revelar los hechos sobre el aborto en el segundo trimestre, como evidencia de por qué debe tratarse como una forma legítima de atención a la salud de las mujeres y apoyarse en las políticas de salud pública.
Women seek second trimester abortions for much same reasons as first trimester abortions, but they tend to be quite young women with little awareness of pregnancy symptoms, poor women who need time to raise the money to pay the higher costs of a second trimester abortion, women who do not know where to seek help, those who come up against barriers created by the health system, women who only learn of fetal indications in the second trimester, and women whose personal situations are complicated and whose reasons for seeking abortion are often compelling. A qualitative study in the United States, for example, among 398 urban women seeking abortion at 5–23 weeks of pregnancy, found that the women first presenting in the second trimester came an average of 70 days later than those presenting in the first trimester. In 58% of cases, this was due to delayed recognition of pregnancy and delayed confirmation of pregnancy with a pregnancy test. Logistical delays occurred in arranging insurance to pay for the abortion, problems locating a provider and time lost due to an inappropriate initial referral, which were experienced in almost two-thirds of cases.Citation1
Some people consider all abortions after the first trimester as “late”. When they say this, they often mean they think they are “too late”, and that there is something wrong with the women who seek them, whom they think should be treated punitively as a result. This is found even where abortion laws have been liberalised in the first trimester; the stigma of abortion shifts to those in the second trimester. This is reflected in many laws covering second trimester abortion, which either do not allow second trimester abortion at all or restrict the grounds and create barriers to obtaining a second trimester abortion.
This paper looks briefly at data on the safety of second trimester abortion and the proportion of abortions that take place in the second trimester. Its main focus is on the laws and regulations governing second trimester abortion. It focuses on countries where most or at least some second trimester abortions are allowed, including in Europe, where women are still forced to travel for second trimester abortions, and countries in the developing world, where most second trimester abortions remain unsafe. Examples are taken from the United Nations' Abortion: A Global Review, reports by the Center for Reproductive Rights and Guttmacher Institute, articles in Reproductive Health Matters, relevant articles indexed in PubMed, news stories and personal communications. Some of the countries whose laws are covered in other papers in the publication where this paper appearsFootnote* are not included to avoid repetition. This paper is not a systematic review of countries and their laws or the literature, and it does not go into the differences between what exists in law and practice, which would have taken more time and resources than were available and would require a lengthy thesis or a book.
Mortality and morbidity related to unsafe second trimester abortion
Approximately 42 million pregnancies were terminated in 2003, of which nearly 20 million were unsafe. 98% of the unsafe abortions took place in developing countries with restrictive abortion laws, resulting in an estimated 66,500 deaths.Citation2 Approximately five million women are hospitalised each year with complications following unsafe abortion. By comparison, complications from safe abortion procedures and hospitalisation for these are very rare.Citation3 The proportion of complications related to unsafe second trimester abortion among women who have been hospitalised is unknown.
Today, in a growing number of settings where abortion is legally restricted, women are using the drug misoprostol (Cytotec) to cause a miscarriage, whether under a doctor's care or self-administered. This includes most of Latin America and the Caribbean, parts of Asia, several countries in Africa and a few European countries.Footnote† This has greatly reduced the severity of complications and meant that many women are seeking hospital care primarily for incomplete abortions, which can be treated most of the time with vacuum aspiration.Citation4 Although it is not recommended that women attempt to use misoprostol outside a clinical setting after nine weeks of pregnancy, anecdotal reports indicate that women who have no other option are doing so anyway, including after 13 weeks. No one knows how common this is nor how many women use an effective regimen or need additional treatment afterwards.
Few population-based studies in legally restricted settings, where almost all unsafe abortions take place, distinguish how many take place in the second trimester. Both complications and deaths in the second trimester are also often hidden in clinical records and reports of deaths. A study in 2001 in two sites in two states of Mexico, for example, with about 1.5 milllion inhabitants, found no officially registered second trimester abortion-related deaths. However, verbal autopsy and review of clinical records and death certificates found, among the 32 registered maternal deaths, four misclassified deaths that were actually second trimester abortion-related deaths,Citation5 that were probably purposely covered up to avoid investigation and prosecution.
A revealing study in Kenya in 2002 examined records of all women presenting prior to 22 weeks of pregnancy with abortion-related complications at 54 district hospitals in a three-week period. 809 patients were identified with abortion complications, of which approximately 16% were aged 14–19 years. Most (80%) presented with incomplete abortion. Approximately 34% of the 809 women were in the second trimester of pregnancy. Those with second trimester abortion complications were 3.6 times as likely to have signs of mechanical injury as women with first trimester complications, and the second trimester complications were 1.7 times as likely to be of moderate or high severity as the first trimester complications. Moreover, six of the seven women who died were in the second trimester. Even though it is thought that first trimester abortion deaths are declining in Kenya, the data on second trimester complications underscore the need to make second trimester procedures safer as well.Citation6
The Soviet Union was the first in the world to make abortion legal on request, in 1920. In Russia today, however, many second trimester abortions have remained unsafe even though the law allowed them on a wide range of grounds until 2003. A study analysing all abortions and abortion-related deaths in 1999 found that only 6.6% of all abortions were performed between 13 and 27 weeks, but 76% of abortion-related deaths were associated with these abortions, both inside and outside of medical institutions. Improving access to safe second trimester methods, preventing delays and better treatment of complications were the key strategies recommended for reducing second trimester abortion-related deaths.Citation7 Instead, in 2003, the Russian Federation restricted the legal grounds for abortions at 13–22 weeks from 12 to four,Citation8 with the likelihood of detrimental public health consequences.
The number of women who attempt an unsafe abortion is estimated to be 20–25% higher than the number who succeed. Some women may make more than one attempt before succeeding, each time risking their health and lives.Citation2 Laws that create barriers to obtaining an abortion thus mostly fail to stop women having them, but do force women to risk their lives doing so, and probably contribute to making complete abortions later than they need to be. How often this occurs with attempted second trimester abortions is unknown.
Second trimester abortions are safe with trained providers
In 1981, second trimester abortions comprised 10–15% of all reported terminations globally, but were responsible for two-thirds of all major complications and over 50% of all abortion-related maternal deaths.Citation9 More recent figures could not be found. Much has changed since 1981, however.
Abortion-related deaths have been declining globally in the past three decades because many more countries now have safe, legal abortion, abortion methods have become substantially safer and simpler, more providers have been trained, and women with complications are more likely to seek and to receive medical help, even where abortion is still legally restricted. Second trimester abortions carry relatively more risk and account for a greater proportion of complications than first trimester abortions, even when the procedure used is safe, the provider skilled and the quality of care high. This is because abortion procedures and pregnancy itself are riskier as pregnancy progresses.
Nevertheless, even throughout the second trimester, abortion with a skilled provider is very safe. Recent data from the United States, for example, show that there is only one death per 1,000,000 abortions in the first eight weeks of pregnancy, one death per 29,000 abortions at 16–20 weeks, and one death per 11,000 abortions at 21 weeks or later.Citation10 An estimation of pregnancy-related mortality in the US by pregnancy outcome found that abortion (induced and spontaneous) was associated with the lowest risk, live birth intermediate risk (one death per 14,000 live births), and ectopic pregnancy and fetal death the highest risk.Citation11
While the difference in risk underlines the importance of encouraging women with unwanted pregnancy to seek abortion as soon as possible after a missed period, it also reassures that deaths from abortion at all stages are rare when providers are trained. Complication rates with skilled provision of currently approved second trimester abortion methods (mifepristone–misoprostol and dilatation and evacuation (D&E)) are also very low.Citation12
Proportion of safe second trimester abortions to total abortions
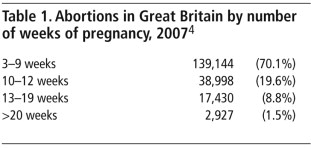
There will always be women who need abortions after 13 weeks of pregnancy, but the numbers diminish greatly by 20 weeks, becoming rare after 24 weeks. It is not the law that makes this happen, but women themselves. For example, in Britain in 2007, 90% of abortions took place by 12 weeks of pregnancy,Footnote* and only 1.5% of abortions took place after 20 weeks (Table 1),Citation13 in a context where the law permits abortions up to 24 weeks on exactly the same grounds as first trimester abortions and on more limited grounds only after that.
In South Africa, in contrast, reflecting the pre-law reform situation, over one-third of abortions in 1997 were after 12 weeks,Citation14 whereas now, second trimester abortions constitute 20% of all abortions.Citation15 This is in a context where the law allows abortion on request up to 12 weeks but restricts the reasons at 13–20 weeks to risk of injury to the woman's physical or mental health, substantial risk of severe fetal abnormality, rape or incest, or significant effect on the socio-economic circumstances of the woman, and after 20 weeks, to danger to the woman's life and severe fetal abnormality.Citation16 Although 20% is still a high proportion, the reduction following law reform shows the close association of legality with improved access to services.
Laws governing second trimester abortion: Footnote* intent to restrict
How late in pregnancy abortions should be permitted and carried out is treated as a matter of great controversy in the public policy arena, especially where there is an active anti-abortion movement. Given the lack of political support for second trimester abortions historically, almost all existing abortion laws and regulations are restrictive (if not punitive) in practice, even if not in intent, and serve to create barriers to obtaining a second trimester abortion, sometimes impassable ones. Abortion in both first and second trimesters is most commonly permitted on the following grounds:
to save the life of the woman
to preserve the physical health of the woman
to preserve the mental health of the woman
pregnancy resulting from rape or incest
risk of fetal impairment
economic or social reasons
at the woman's request.
Although legal grounds alone may not reflect the way in which the law is applied, nor the quality of services, in more than 160 countries where legislation allows abortion on broad indications, there is a lower incidence of and much lower mortality from unsafe abortions, than in countries where legislation greatly restricts abortion. Most abortions become safe mainly or only where women's reasons for abortion and the legal grounds for abortion coincide.Citation17
64% of the world's women live in countries where abortion is generally permissible, and one quarter where it is severely restricted.Citation18 Like many documents on global abortion law and policy, however, the source of these figures does not distinguish between law and policy in the first and second trimester. Some generalisations can be made, however. Where first trimester abortions are narrowly restricted, the law does not tend to permit second trimester abortion at all, except to save the life of the woman. Saving the woman's life is a crucial legal grounds, as its withdrawal in Nicaragua in 2006 has shown,Citation19 but overall very few abortions are carried out on this grounds except where serious ill-health in pregnant women is common.
In addition to protecting the woman's life, countries that do permit first trimester abortions also permit some second trimester abortions, usually on one or more of these grounds: the woman's health and sometimes mental health (narrowly or liberally interpreted), rape and incest, and fetal abnormality. Some allow second trimester abortion for all these reasons plus economic and social reasons, including South Africa.Citation14 Only a few allow second trimester abortion on request. Some countries require the approval of an appointed commission or one or more physicians, including in places where physicians are scarce. Some countries' laws are unclear as to what constitutes a legal second trimester procedure, for example, many countries whose laws are restrictive in intent do not distinguish according to weeks of pregnancy, e.g. in Latin America.
Britain since 1967, China since 1979 and the Netherlands since 1984 are among the few to have the same legal grounds for both first and second trimester abortions up to 24 weeks. Britain requires the authorisation of two doctors for all abortions with a broad list of grounds (not on request), while the Netherlands has abortion on request but with a required reflection period. In both countries, abortion is not permitted once the fetus is able to survive outside the womb. In the Netherlands, this is interpreted variously by physicians to mean after 22–24 weeks, after which abortions are virtually never done.Citation20Citation21 In Britain, viability was considered to be 28 weeks until the law was amended in 1990, reducing the time limit to 24 weeks, and creating exceptions after 24 weeks for which abortion would still be allowed. Those exceptions are: risk of grave permanent injury to the physical or mental health of the pregnant woman; risk to the life of the pregnant woman greater than if the pregnancy were terminated; and substantial risk that if the child were born it would suffer from such physical or mental abnormalities as to be seriously handicapped.Citation22
China has allowed abortion with the consent of the woman, since 1979, up to six months of pregnancy. Second trimester abortions are performed in a hospital by a physician. Abortion services are provided by the Government of China as a public service. The law allows 30 days of paid sick leave if the pregnancy is terminated after the first trimester.Citation23
Sweden has abortion on request up to the end of 18 completed weeks of pregnancy. After that, abortion may be performed only if the National Board of Health and Welfare has granted the woman permission for the procedure. Such permission may only be granted if exceptional grounds exist for the abortion, and may not be granted if there is reason to assume that the fetus is viable. In cases of grave danger to the life or health of the woman, on account of her having an illness or bodily defect, permission may be granted regardless of how far the pregnancy has progressed.Citation24
These four laws are among the most liberal in the world as regards second trimester abortion. Canada is unique, in that it has had no specific law on abortion at all since the highest court struck down the existing law as inequitable in 1989. This happened following a comprehensive study published in 1977 that found sharp disparities in women's access to therapeutic abortions. For example, approval of a committee was required but most hospitals had no committee, or the committee never met. Obtaining permission could take as long as eight weeks, which meant abortions requested early often occurred in the second trimester. Repeated efforts by anti-abortion activists to date have failed to impose a new law, though issues of access continue to make it difficult for rural women especially to obtain abortions without travelling great distances.Citation25
A court case in the United States, Roe v. Wade 1973, allows abortion on request through the second trimester, but access and funding for abortions are limited for many women, especially by a tangle of complicated regulations and restrictions imposed both by the federal government and many states. Since 2007, the so-called Partial Birth Abortion Ban Act, first passed in 2003 and challenged unsuccessfully in court, “asserts that the state's interests in how an abortion is performed and in fetal life override women's rights”. In banning a particular late abortion procedure, it has negative implications for evidence-based practice, the training of providers and clinical innovation, as well as opening a door for possible further restrictions in the law.Citation26
In the state of Victoria, Australia, women have access to abortion under common law, through a judge's 1969 ruling that permits abortion when it is necessary to protect the life or health of the woman. It was agreed in 2006 that abortion should be decriminalised. A 2007 report to the Victoria state parliament recommends three possible models for decriminalisation, up for a vote in 2008. One model would take abortion out of the Crimes Act, but keep the decision about whether a procedure was “necessary” in the hands of the medical profession and the law. The second model would allow women's consent for abortions up to 24 weeks of pregnancy, after which one or two doctors would have to assess whether the continuation of the pregnancy posed a risk of harm to the woman. The third model would make the woman the only decision-maker throughout; abortion would only be deemed unlawful if conducted by unqualified people and without the woman's consent. 80% of people polled in the state indicated their support for abortion as a woman's decision.Citation27
India's Termination of Pregnancy Act 1971 allows an unwanted pregnancy to be terminated up to 20 weeks of pregnancy, but requires a second doctor's approval if the pregnancy is beyond 12 weeks. The grounds include grave risk to the physical or mental health of the woman in her actual or foreseeable environment, as when pregnancy results from contraceptive failure, or on humanitarian grounds, or if pregnancy results from a sex crime such as rape or intercourse with a mentally-challenged woman, or on eugenic grounds, where there is reason to suspect substantial risk that the child, if born, would suffer from deformity or disease.Citation28 While these are inclusive and broad grounds for the second trimester, India falls down at the service delivery level, especially in rural areas. Getting a second doctor's approval, especially in a rural setting, would be punitive and restrictive in effect, if indeed it is adhered to.
Many of the generation of countries who reformed their laws after about 1995 have been less progressive. These include Albania, Cambodia, Nepal, Portugal, South Africa, Switzerland and the Federal District of Mexico City. All of the countries (and the city) in this group currently allow abortion on request up to 10, 12 and in a few cases 14 weeks of pregnancy. After that, the grounds become far more restrictive. This is similar to France and Italy, who reformed their laws in the mid- to late 1970s and included abortion at the woman's request, but only in the first trimester. In Cambodia, under a 1997 law whose aim was to reduce maternal deaths from unsafe abortions and contribute to fertility control, a woman may obtain an abortion on request during the first 12 weeks of pregnancy. After this, abortions are allowed only if there is a probability of the pregnancy developing abnormally or if the pregnancy poses a danger to the mother's life; if the baby who will be born can get an incurable disease; or if the pregnancy is caused by rape. In these cases, the abortion must be approved by a group of two or three medical personnel.Citation29 In some cases, e.g. Portugal and Mexico City, they were legislating changes in a context in which abortion was so contested that advocates felt they could only go so far and still hope to succeed. Portugal's 2007 law, for example, makes abortion legal on request only up to ten weeks of pregnancy. Thereafter, abortion is allowed up to 24 weeks only if there are sound reasons for assuming that the child will suffer from a serious incurable disease or congenital malformation (in the case of non-viable fetuses, termination may be performed at any time), or if abortion is the only way to avert risk of death or grave and irreversible damage to physical or mental health of the woman.Citation30
In Cuba, since 1979, abortion is legal at the request of the woman through 12 weeks. Abortions of 10–12 weeks require examination by a gynaecologist and counselling from a social worker. Women under 18 years of age must have parental consent and those under 16 require authorisation by a medical committee. For second trimester abortion, in addition to the conditions for first trimester procedures, the abortion must be authorised by a committee of obstetricians, psychologists and social workers.Citation31
Under Nepal's 2002 law, abortion is allowed up to 12 weeks with the woman's consent; up to 18 weeks if the pregnancy is the result of rape or incest, and at any time during the pregnancy on the advice of a medical practitioner if the life, or physical or mental health of the woman are at risk, or the fetus is deformed or incompatible with life. This law is a huge advance compared to the country's previous law, which allowed abortion only to save the life of the woman,Citation32 but problems of interpretation of what is allowed in the second trimester, e.g. the conditions for the mental health indication, are concerning providers and policymakers.
In Switzerland, a law dating from 2001 allows abortion on request up to 12 weeks and for therapeutic reasons thereafter. Before that, women had to obtain a second medical opinion confirming that their physical, mental or socio-medical health was at risk because of the pregnancy, without any upper time limit. In 2006, the percentage of abortions above 12 weeks was only 3.8%. It has always been difficult to obtain an abortion after 12–14 weeks in Switzerland, even before the new legislation and without an upper time limit. The law was simply interpreted more restrictively in the second trimester. Women without a compelling medical or socio-medical reason (e.g. maternal health, drug addiction, fetal anomaly) travelled to other countries (mostly Netherlands, Britain and more recently Spain) for abortion and still do, even though the new law allows for quite a liberal interpretation of health grounds (Anne-Marie Rey, Abortion-Information (formerly USPDA), Zollikofen, Personal communication, 2008).
Another group of countries whose laws were reformed in similar ways in the past ten years include Benin, Bhutan, Burkina Faso, Chad, Colombia, Ethiopia, Guinea, Mali, Saint Lucia, Swaziland, and Togo.Citation33 These laws contain restrictive grounds whereby abortion is legal to save the woman's life and protect her health (and in some cases also her mental health), and in some countries also in cases of rape and incest and/or fetal impairment. In most cases, these laws have replaced laws that narrowly allowed abortion only to save the woman's life and possibly her health in contexts where almost no legal abortions were being carried out. A large question in relation to these new laws, however, is whether or not, since their passage, more women have access to a safe second trimester abortion than before they were passed.
Moreover, it is not always clear whether these laws create the conditions to ensure safe abortions can be carried out in either trimester of pregnancy. Burkina Faso, for example, attached the following conditions to its 1996 law: voluntary interruption of pregnancy is allowed at all times during pregnancy if two physicians attest that the continuance of the pregnancy endangers the health of the woman or that a strong possibility exists that the unborn child will be afflicted with a condition of exceptional seriousness recognised as incurable at the time of diagnosis. Moreover, in a case of rape or incest established by the State prosecutor, a woman is authorised to request a physician to perform an abortion during the first 10 weeks of pregnancy.Citation34 With limited access to one doctor, let alone two, limited access to facilities for diagnosis of fetal anomalies, and even less chance of proving rape or incest within a ten-week window, these conditions are not likely to lead to legal abortions, let alone second trimester ones.
Brazil is an example of what happens when abortion for fetal indications is not legal. Women who cannot obtain an illegal abortion are forced to continue the pregnancy and deliver the baby, even if it will certainly die soon after birth, such as with anencephaly. In Brazil, in these cases, women can seek a judge's authorisation from the office of the Attorney General for an abortion. However, women carrying a fetus diagnosed with anencephaly felt it was embarrassing and humiliating to have to go to court during such a painful time.Citation35 A temporary Ministerial order in 2004 granted authorisation of all pregnancy terminations in cases of anencephaly until such time as the law could be changed,Citation36 only to rescind the order three months later. The Brazilian Supreme Court will be taking up a case on anencephaly again in August 2008 to re-review this decision. The presiding judge, Marco Aurelio, is quoted as saying he believes anencephaly falls under therapeutic abortion because the fetus is not viable outside of the uterus.Citation37
British obstetrician–gynaecologist David Paintin once wrote: “Although abortion after 24 weeks should be necessary only on the rare occasions when a fetal abnormality has not been discovered earlier in pregnancy, it should be regarded as ethical regardless of its timing.”Citation38 Debora Diniz from Brazil recommended that in cases of fetal anomaly incompatible with life, termination should be classified as therapeutic premature delivery, not as induced abortion, legally or medically, so that it is not regulated under abortion law.Citation39 It would be far preferable, however, if abortion laws did not create barriers in these cases.
Crossing borders for second trimester abortions in Europe
In most of Europe today, the state recognises that it has a duty of care to make abortion safe. Nevertheless, Northern Ireland, Ireland, Malta and Poland, where abortion is legally restricted, hypocritically count on other countries to take care of their “problem” for them.
Women travelling from one European country to another for abortion has been going on since eastern European countries followed the Soviet Union in legalising abortion in the 1950s, and western European women went to Poland and Yugoslavia for abortions. In 1975, in contrast, about 90% of the 100,000 abortions performed in Dutch clinics were women from abroad, mostly West Germans (Evert Ketting, personal communication, July 2008). At least 130,500 Irish women have travelled to England and Wales to date to have abortions since 1968.Citation13 In 1976, 30,000 Spanish women were travelling annually to Britain for safe abortionsCitation40 and at least one clinic in London specialised in abortions over 20 weeks for an international clientele. The number of women travelling to Britain declined from 56,591 in 1973 to 9,833 in 2000,Citation41 and the number visting the Netherlands for abortion also decreased, from 10,000 in 1990 to about 4,000 in 2004.Citation20 Since more countries made abortion legal and accessible in the first trimester, most women are now travelling for second trimester procedures.
Women over 12–14 weeks of pregnancy still have to travel elsewhere from France, Portugal and Italy. They and women who are 20–24 weeks usually go to the Netherlands or Britain and to Spain after 24 weeks, through clinic referrals. Those who travel to Spain at 25–28 weeks are a handful each year but a very vulnerable group. Because legal abortions are almost unobtainable in Poland, Polish women are travelling to Germany, Czech Republic, Austria, Netherlands and Belarus. They are probably also going to other Eastern European countries (Ukraine, Lithuania) if they live close to the border and have connections in those countries (Wanda Nowicka, personal communication, October 2007). The numbers seeking second trimester abortion are unknown.
The Spanish law of 1985 allows abortion in the first 22 weeks of pregnancy in cases of fetal malformation, in the first 12 weeks in cases of rape, and without a clear upper time limit if the woman's mental or physical health is at risk. Late second trimester abortion suddenly hit the news in November and December 2007 after police raided several Barcelona clinics accused by an anti-abortion group of carrying out late second trimester abortions illegally. Some of the patients were believed to have been from other European countries. Several doctors and clinic staff were detained, two Madrid clinics were closed and about 40 patients came under investigation. The events prompted a wave of minor attacks, such as phone threats or smashed windows, against abortion clinics.Citation42 In response, 40 abortion clinics all over Spain staged an unprecedented strike in January 2008, supported by feminist and other groups. The situation exposed ambiguities in the interpretation of the health grounds in the law, particularly mental health grounds, and the Socialist Prime Minister Zapatero pledged to carry out reforms after he was re-elected in March 2008. In April 2008, it was reported that charges against 21 women accused of having illegal abortions had been dropped because the women had acted with the conviction that they were not violating the law.Citation43 In July 2008, the Spanish government issued guidance that women's medical records could only be opened by court order, in order to protect the privacy of women who have abortions.Citation44
In what may or may not have been a related case, a 24-year-old Dutch–Moroccan woman was arrested in November 2007, under suspicion that she had had a late second trimester abortion (rumour said anything from 22 to 27 weeks) in one of the Spanish clinics being investigated there. Though legal under Spanish law, the abortion would have been illegal under Dutch law, and the Dutch clinic where she first sought help was also investigated, as it was alleged that they had referred her – quite legally if they did so – to Spain. The woman was not permitted to speak to anyone except her solicitor, and not released from prison for four weeks. It later emerged that she had told her partner she had had a stillbirth. He became suspicious and informed the police.Citation45Citation46 The case shocked both politicians and legal experts in the Netherlands, as it was the first time since the 1981 legislation was passed that anyone had been arrested, let alone imprisoned, for having terminated a pregnancy (E-mail communication, Maria Francès, Thea Schipper, FIAPAC board members, 14 December 2007). Both the Spanish and Dutch cases remain to be resolved at this writing. They signal that even in countries where late abortions have been legal for a quarter of a century and widely accepted, anti-abortion agitation can disrupt lives and threaten the provision of services literally overnight, as also happened in Poland.
Discussion and recommendation
It has been an eye-opener to learn, during the reading for this paper, how uncommon it is for global abortion statistics and other information on abortion produced by international institutions to be disaggregated or analysed in depth according to number of weeks of pregnancy. It is primarily in the clinical literature on abortion methods and data on maternal mortality that length of pregnancy is a central factor.
Second trimester abortion has become a popular target of anti-abortion campaigners. Because of the ambivalence of many people who are otherwise pro-choice with regard to early abortions, second trimester abortion has been relatively neglected in progressive abortion law reform in recent years. including in countries where first trimester abortion is available on broad grounds or on request. Where abortion remains legally restricted, the higher risk to the health and lives of women forced to seek unsafe second trimester procedures or travel to other countries for abortion has mostly been hidden or ignored. These are some of the many indications of the stigma attached to second trimester abortion. Countries' laws and regulations on second trimester abortion may perhaps be taken as a truer measure of the extent to which they are committed to voluntary motherhood and women's right to decide the number and spacing of their children, for this reason.
It is time for the restrictive nature of most second trimester abortions laws to be challenged. While everyone who supports safe, legal abortion agrees that women should be able to obtain an abortion as early as possible, the need for abortion in the second trimester will continue to exist, and should be acknowledged and supported.
A progressive, women-centred law on abortion should provide that:
the need for second trimester abortions is met in a safe, timely and sympathetic manner;
abortion is legal at the pregnant woman's request up to 24 weeks gestation and on therapeutic grounds after that (e.g. as per current British law), and
no other barriers or hurdles should be imposed on women seeking second trimester abortion.
In-depth, country-based research is needed, to bring out the facts on second trimester abortion, as evidence of why it should be treated as a legitimate form of women's health care and supported in public health policy.
Notes
* Second Trimester Abortion: Women's Health and Public Policy. Reproductive Health Matters 2008;16(31 Supplement). Berer M, editor, for the International Consortium for Medical Abortion.
† Reports at: Medical Abortion: An International Forum on Policies, Programmes and Services. International Consortium for Medical Abortion. Johannesburg, 17–20 October 2004.
* Britain has for many years had a lower proportion of total abortions before 13 weeks than several other European countries.
* Wording used to describe the laws in this section comes from the texts where they were found, with minor editing for clarity. Most are from translations, whether official or otherwise.
References
- EA Drey, DG Foster, RA Jackson. Risk factors associated with presenting for abortion in the second trimester. Obstetrics & Gynecology. 107(1): 2006; 128–135.
- World Health Organization. Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2003. 5th ed., 2007; WHO: Geneva.
- S Singh. Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. Lancet. 368: 2006; 1887–1892.
- M Arilha, RM Barbosa. Cytotec in Brazil: “At least it doesn't kill”. Reproductive Health Matters. 1(2): 1993; 41–52.
- D Walker, L Campero, H Espinoza. Deaths from complications of unsafe abortion: misclassified second trimester deaths. Abortion Law, Policy and Practice in Transition. Reproductive Health Matters. 12(24 Supplement): 2004; 27–38.
- H Gebreselassie, MH Gallo, MA Monyo. The magnitude of abortion complications in Kenya. BJOG. 112(9): 2005; 1229–1235.
- IA Zhirova, OG Frolova, TM Astakhova. Abortion-related maternal mortality in the Russian Federation. Studies in Family Planning. 35(3): 2004; 178–188.
- Decree No. 485 voids Decree No. 567 of May 8, 1996. Cited in: Center for Reproductive Rights. Abortion worldwide: twelve years of reform. Briefing Paper. July 2007.
- C Tietze. Second-trimester abortion: a global view. WE Brenner, LG Keith, GS Berger. Second-Trimester Abortion. 1981; John Wright: Boston.
- Guttmacher Institute. Facts on induced abortion in the United States. 2008; Guttmacher Institute: New York. At: <www.guttmacher.org/pubs/fb_induced_abortion.pdf. >.
- DA Grimes. Estimation of pregnancy-related mortality risk by pregnancy outcome, United States, 1991–1999. American Journal Obstetrics & Gynecology. 194(1): 2006; 92–94.
- D Grossman, K Blanchard, P Blumenthal. Complications after second trimester surgical and medical abortion. Reproductive Health Matters. 16(31 Suppl): 2008; 173–182.
- Department of Health. Abortion Statistics, England and Wales: 2007. Statistical Bulletin 2008/1. 19 June 2008. At: <www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_085508. >.
- Reproductive Rights Alliance. Barometer. 2(1): 1998
- J Harries, P Orner, M Gabriel. Delays in seeking an abortion until the second trimester: a qualitative study in South Africa. Reproductive Health. 4(1): 2007; 7.
- Choice on Termination of Pregnancy Act 1996: Republic of South Africa. Reproductive Health Matters. 5(9): 1997; 116–118.
- M Berer. National laws and unsafe abortion: the parameters of change. Reproductive Health Matters. 12(24 Suppl): 2004; 1–8.
- SA Cohen. New data on abortion incidence, safety, illuminate key aspects of worldwide abortion debate. Guttmacher Policy Review. 10(4): 2007
- Abortion ban passed; first pregnant woman dies [Round Up]. Reproductive Health Matters. 15(29): 2007; 210.
- S Gevers. Abortion legislation and the future of the ‘counseling model’. European Journal of Health Law. 13: 2006; 27–40.
- O Loeber, C Wijsen. Factors influencing the percentage of second trimester abortions in the Netherlands. Reproductive Health Matters. 16(31 Suppl): 2008. 30–36.
- R Ingham, E Lee, SJ Clements. Reasons for second trimester abortion in England and Wales. Reproductive Health Matters. 16(31 Suppl): 2008. 18–29.
- China: abortion policy. Abortion: A Global Review. United Nations Population Division, Department of Economic and Social Affairs, 2002. At: <www.un.org/esa/population/publications/abortion/profiles.htm. >.
- Ministry of Health and Social Affairs, Sweden. The Abortion Act 1974:595. With amendments up to and including Swedish Code of Statutes 2005:294. (Unofficial translation). At: <www.regeringen.se/content/1/c6/06/28/70/4755c9dc.pdf. >.
- Rodgers S. Abortion denied: bearing the limits of law. (Manuscript as at March 2007).
- S Yanow, TA Weitz. Implications of the federal abortion ban for women's health in the United States. Reproductive Health Matters. 16(31 Suppl): 2008. 99–107.
- M Windisch, citing Leslie Cannold of Pro-Choice Victoria. Decriminalise abortion now! Green Left Online. 14 June 2008. At: <www.greenleft.org.au/2008/755/39006. >.
- SS Hirve. Abortion law, policy and services in India: a critical review. Reproductive Health Matters. 12(24 Suppl): 2004; 114–121.
- Cambodia: abortion policy. Abortion Policies: A Global Review. United Nations Population Division, Department of Economic and Social Affairs, 2002. At: <www.un.org/esa/population/publications/abortion/profiles.htm. >.
- Portugal Law No.16/2007 of 17 April 2007 determining the cases in which voluntary termination of pregnancy is not illegal. (Diário da República, Part I, 17 April 2007, No. 75, pp. 2417–2418). WHO International Digest of Legislation. At: <www.who.int/idhl-rils/results.cfm?language=english&type=ByTopic&strTopicCode=VII&strRefCode=Port>.
- Cuba: abortion policy. Abortion Policies: A Global Review. United Nations Population Division, Department of Economic and Social Affairs, 2002. At: <www.un.org/esa/population/publications/abortion/profiles.htm. >.
- S Shakya, S Kishore, C Bird. Abortion law reform in Nepal: women's right to life and health. Reproductive Health Matters. 12(24 Suppl): 2004; 75–84.
- Center for Reproductive Rights. Abortion worldwide: twelve years of reform. Briefing Paper. July 2007.
- Burkina Faso: abortion policy. Abortion Policies: A Global Review. United Nations Population Division, Department of Economic and Social Affairs, 2002. At: <www.un.org/esa/population/publications/abortion/profiles.htm. >.
- LL Ferreira da Costa, E Hardy, MJ Duarte Osis. Termination of pregnancy for fetal abnormality incompatible with life: women's experiences in Brazil. Reproductive Health Matters. 13(26): 2005; 139–146.
- Freitas S. STF libera aborto em caso de anencefalia. Folha de São Paulo. São Paulo, 2 July 2004. Suplemento Folha Cotidiano. p.4. Cited in: Ferreira da Costa LL, et al.6
- Ipas. 2nd Brazil update. E-mail. 14 July 2008.
- D Paintin. Abortion after 24 weeks. British Journal of Obstetrics and Gynaecology. 104(4): 1997; 398–400.
- D Diniz. Antecipação terapêutica do parto: uma releitura bioética do aborto por anomalia fetal no Brasil. D Diniz, DC Ribeiro. Aborto por Anomalia Fetal. 2003; Debora Diniz: Brasília, 21–92. Cited in: Ferreira da Costa LL, et al.33.
- 30.000 women travel to London every year for abortions. El País Semanal No.1. 3 October 1976.
- Department of Health. Abortion statistics. 2006; DoH: London.
- Madrid pledges protection to abortion clinics striking over attacks. Deutsche Presse Agentur, 10 January 2008.
- El Periodico, 30 April 2008. Reported in: Womens Enews, 3 May 2008.
- Agence-France Presse, 11July 2008. Cited in: Cheers and Jeers of the Week. Women's E-news, 19 July 2008.
- Dutch woman fails to halt murder investigation linked to late abortion in Spain. Associated Press, 31 January 2008.
- Dutch woman freed after “illegal” abortion. 13 December 2008. At: <www.radionetherlands.nl/news/international/5555842/Dutch-woman-freed-after-illegal-abortion. >.