
Abstract
Population-Health-Environment (PHE) is an interdisciplinary model of programme design which recognises the complex interconnections between people, their health and their environment. PHE responds holistically to the challenges faced by ecosystems and the communities dependent on them, with thematically distinct but interconnected work strands sharing the same infrastructure, resources and goals. This has been shown to achieve better outcomes than tackling health and environmental issues in isolation. This paper shows how PHE programme design has been used by Blue Ventures for providing family planning services in a remote, biodiverse coastal region in southwest Madagascar. The PHE programme has integrated family planning services into a pre-existing, community-based conservation programme, aided by the established infrastructure and good community relations developed by the conservation workers. Implementation of the programme has led to a strong uptake of family planning services, and couples in the region are now able to make their own family planning choices. Successes and challenges of the programme are discussed.
Résumé
Le projet PHE (Population-Santé-Environnement) est un modèle interdisciplinaire de conception des programmes qui tient compte des interconnections complexes entre les individus, leur santé et leur environnement. Le modèle PHE répond globalement aux difficultés rencontrées par les écosystèmes et les communautés qui en dépendent, avec des axes de travail thématiquement distincts, mais interconnectés, qui partagent la même infrastructure, les mêmes ressources et les mêmes objectifs. Cette méthode a obtenu de meilleurs résultats que lorsque les questions sanitaires et environnementales sont abordées séparément. Cet article montre comme Blue Ventures a utilisé une conception de programme PHE pour assurer des services de planification familiale dans une région côtière isolée, à la riche biodiversité, du sud-ouest de Madagascar. Le programme PHE a intégré des services de santé dans un programme communautaire préexistant de conservation, où les agents de santé ont pu rapidement et efficacement fournir des services de planification familiale, aidés par l’infrastructure établie et les bonnes relations communautaires nouées par les agents de conservation. La mise en łuvre du programme a abouti à une forte utilisation des services de planification familiale, et les couples de la région sont désormais capables de faire leurs propres choix de planification familiale.
Resumen
Población-Salud-Medio Ambiente (PSM) es un modelo interdisciplinario para el diseño de programas, que reconoce las complejas interconexiones entre las personas, su salud y el medio ambiente. PSM responde holísticamente a los retos que enfrentan los ecosistemas y las comunidades que dependen de estos, con líneas de trabajo temáticamente distintas pero interconectadas, que comparten la misma infraestructura, recursos y objetivos. Se ha demostrado que con este modelo se logran mejores resultados que al abordar asuntos de salud y medio ambiente de manera aislada. En este artículo se muestra que el modelo PSM para el diseño de programas ha sido utilizado por Blue Ventures para ofrecer servicios de planificación familiar en una región costera remota y biodiversa del suroeste de Madagascar. El programa de PSM integró los servicios de salud en un programa de conservación comunitario preexistente, donde trabajadores de salud lograron proporcionar rápida y eficazmente servicios de planificación familiar, con la ayuda de la infraestructura establecida y buenas relaciones con la comunidad forjadas por los trabajdores en conservación. La implementación del programa ha producido una sólida aceptación de los servicios de planificación familiar, y las parejas de la región ahora pueden elegir de entre las diferentes opciones de planificación familiar.
The Population-Health-Environment approach, or PHE, is an interdisciplinary model of programme design which responds to the interconnected challenges faced by ecosystems and the communities dependent on them. These challenges include poor health, unmet family planning needs, environmental degradation, food insecurity, gender inequality and vulnerability to climate change. This holistic approach seeks to reflect the way in which pressures affecting people and their environment are connected, and often work to compound each other. This can result in a vicious cycle, with unsustainable natural resource use, environmental degradation and deepening poverty impacting and interacting in increasingly negative and synergistic ways. The sustainable management of natural resources is difficult for communities with significant unmet family planning needs, with growing numbers of people placing increasing pressure on resources, and poor health outcomes limiting the ability of communities to engage in biodiversity conservation. Dwindling natural resources are in turn likely to lead to poorer health outcomes and deepening poverty.
With PHE, key work strands are identified – i.e. addressing biodiversity conservation, natural resource management, health needs and livelihood diversification – and implemented in an integrated way, with shared infrastructure, resources and goals. PHE programmes are often located in remote areas of high biodiversity, with the aim of improving the health of ecosystems (ranging from coastal to forest habitats) as well as the health of the communities that are reliant upon them. PHE programmes encompass a range of health interventions, typically including family planning services but also maternal and child health, nutrition, and water and sanitation interventions. The rationale behind this approach is to stop and reverse the vicious cycle described above, with the potential for generating sustained improvements in human and ecosystem health. It also serves to respond to the challenges communities face as they experience them, rather than dealing with natural resource use, food security and health as separate and unrelated issues. The individual work strands are closely coordinated to maximise efficiency, such as through sharing resources or opportunities for community engagement. Where possible, work across different sectors is integrated, such as in the development of messages to the community about the relationships between family size, natural resource management and food security. Efficiencies and synergies are created by addressing issues in this integrated way, leading to cost savings and better outcomes (such as increased contraceptive use and women’s greater involvement in natural resource management) than if these activities were carried out in isolation.Citation1–4
Over one billion people currently live in “biodiversity hotspots”—areas where exceptional concentrations of unique plant and animal species are under threat due to human activity.Citation5 Communities living in remote areas (with high biodiversity) in low-income countries often also have a significant unmet need for family planning services.Citation6 Numerous biodiversity conservation programmes are already operating throughout the tropical developing world, with established infrastructure and strong working relations with local communities. This paper discusses the experiences of Blue Ventures, a British marine conservation organisation operating in southwest Madagascar; it describes how integrating family planning services into the organisation’s pre-existing community-based conservation programme proved to be an effective way of giving partner communities access to these services. The authors discuss the successes and challenges experienced, and introduce the potential for more widespread adoption of this approach as a strategy for addressing unmet family planning needs in other remote areas of high biodiversity.
The need for an interdisciplinary approach in Madagascar
Poverty
The World Bank identified Madagascar as the eighth poorest country in the world in 2012, with a GDP per capita of just USD$ 447, and 92% of the population living on less than US$2 per day.Citation7 Political instability since 2009 has led to a reduction in international investment and donor support,Citation8 contributing to the reduction in the Government of Madagascar’s spending on basic services, including health. In 2011, the health expenditure was US$19 per capita, while in 2012 the health budget was half that, resulting in worsening health service provision and extended public health worker strikes.Citation9,10 A lack of basic infrastructure and years of inadequate investment in education and health services, especially in rural areas, is exacerbating poverty levels.Citation7 This is despite Madagascar’s mineral and oil reserves and potential for ecotourism, as revenues from these industries seldom benefit the local population.
High fertility
According to the UN medium population projection, the average total fertility rate in the least developed countries was projected to fall to 2.8 by 2045–2050. However, the decline has been slower than expected over the last decade, leaving this projection in some doubt.Citation11–13 In Madagascar, the average total fertility rate has steadily fallen from 7.3 births per woman in 1950 to 4.8 births in 2010.Citation14 This, combined with a current life expectancy at birth of 66 years, means that more than 47% of the population is below 15 years of age.Citation15 However, there is significant variation in fertility rates across different regions in Madagascar. In the Atsimo-Andrefana region, the site of Blue Ventures’ PHE programme, the fertility rate is 6.2 births per woman.Citation15
Food insecurity
Persistent food insecurity is a serious problem for the people of Madagascar, with 65% of the population affected.Citation16 More than 50% of children aged below 5 years suffer from stunted growth due to chronically inadequate nutrition.Citation15 This is despite strong agricultural potential, owing to the climate and range of soil types. Natural hazards such as cyclones, floods, droughts and locusts have had a significant impact on Madagascar’s agricultural output.Citation7
Biodiversity and environmental degradation
Madagascar is a priority country for international conservation efforts, due to its unparalleled levels of endemism (80% of species in Madagascar are found nowhere else on earth), biodiversity (it is home to approximately 5% of the world’s plant and animal species) and rates of habitat loss, especially through deforestation to open up farming land, industrial logging and mineral resource extraction.Citation17–19 Expansion of these agricultural and industrial activities and the resulting loss of habitat, is widely accepted as a primary driver of biodiversity loss.Citation20–22
Climate change
Madagascar is predicted to experience significant climate change, threatening food, water security and biodiversity, and increasing the likelihood of extreme weather events.Citation23 Madagascar, along with other least developed countries, conducted an analysis of their vulnerability to climate change, identifying both the range of contributing factors and prioritising interventions likely to be the most effective in building resilience and adaptive capacity, resulting in the development of a National Adaptation Programme of Action (NAPA). This programme included better management of water and sanitation, improvements in agriculture, reforestation and other plans to reduce soil erosion and strengthening of health services, in order to be able to respond to climate change-related disease outbreaks.
The Madagascar NAPA identified population growth as a key factor contributing to the vulnerability of populations and impairing their capacity to adapt to climate change, yet they did not allocate funding for family planning programmes. Short-term projects have been favoured for funding, rather than investing in the development strategies to address longer-term issues.Citation24
PHE in Madagascar
With Madagascar facing such pressing and inter-related challenges, several PHE programmes were implemented in the country, from 1988 until Madagascar’s political crisis of 2009, when funding for biodiversity conservation work in Madagascar was cut significantly.Citation8,25 These programmes, including health and conservation components, have been implemented either by large conservation NGOs such as the World Wildlife Fund (WWF) or Conservation International, or small, locally focused environmental organisations. There is a wide base of PHE experience in Madagascar, but progress on implementation and scale-up of these interventions has been limited, with very few examples of scale-up or replication, often as a result of difficulties in sustaining funding for programmes.Citation25
Blue Ventures: starting from a foundation of marine conservation
Southwest Madagascar is home to one of the largest coral reef systems in the Indian Ocean,Citation26 with a diversity of marine habitats unparalleled in the region.Citation27 Blue Ventures has been working with coastal fishing communities, based in the remote village of Andavadoaka, in the Atsimo-Andrefana region, since 2003, when a group of marine biologists undertook their first expedition to the area.
Blue Ventures’ work initially consisted of marine and coastal conservation, research and education initiatives.Citation28 These conservation activities centre around protecting the region’s extensive coral reef, mangrove and seagrass ecosystems, whose health has been in dramatic decline.Citation29
The region is home to the Vezo ethnic group, who live in semi-nomadic fishing communities and are reliant on coastal resources for their livelihoods and income. Rapid population growth related to unmet family planning needs, a lack of alternatives to fishing and a lack of access to any other resource have been driving the unsustainable use of the coastal and marine resources upon which these communities depend.Citation30
Initial discussions with fishermen and community representatives revealed that their most pressing concern was the rapid decline in their octopus fishery, with octopus being their most valuable cash crop. Working in close partnership with fishermen and women, temporary closures of the octopus fishery were undertaken, lasting two to three months, allowing the octopus population to recover. Owing to their short life spans and extremely rapid growth cycles, octopus populations responded very well and these temporary fishery closures led to a significant increase in octopus landings and fisher revenues (Blue Ventures, unpublished data). The success of these temporary octopus closures led to a widespread replication of this approach by villages all along the southwest coast.
Having witnessed first-hand the ecological and economic benefits of these temporary octopus reserves, and of working cooperatively to manage their marine resources more sustainably, these communities expressed an interest in managing all of their fisheries using the same principles.Citation30 This culminated in the development of a locally-managed marine area (LMMA) of 678 km2 known as Velondriake – meaning ‘to live with the sea’ – which includes Andavadoaka and 24 surrounding villages. Communities from these 25 villages work cooperatively to ban destructive fishing practices and protect key ecological sites within the marine ecosystem. This protected area is governed by a committee of locally elected village representatives, with support from Blue Ventures. In order to monitor the impact of these interventions, Blue Ventures monitors fisheries, marine habitats and the socioeconomic status of communities throughout the area.Citation30
In addition to these efforts to support more sustainable management of marine resources, alternative livelihoods were needed to reduce pressure on the marine environment (as well as help to provide an alternative source of income). Community-based aquaculture, whereby community members cultivate and sell seaweed or sea cucumber to seafood exporters, was introduced. This new income-generating activity is enabling people to become less reliant on fishing, with women in particular standing to benefit, as 44% of sea cucumber farms and 55% of seaweed farms are led by women. The programme is generating a monthly income of up to US$20 per sea cucumber farmer and US$42 per seaweed farmer (Blue Ventures, unpublished data). A series of small business management training workshops are supporting the management of these aquaculture enterprises, and providing farmers with transferrable financial management skills.
Supporting the Velondriake LMMA and community-based aquaculture, along with associated community-based ecological monitoring activities, enabled Blue Ventures to build strong relationships with coastal communities, and required the organisation to invest significantly in local human resources and infrastructure. Local, national and international staff were recruited, vehicles and communication equipment were purchased, and systems were established to ensure effective coordination between Blue Ventures and communities within the LMMA. This provided a valuable foundation and platform for the community health work that was to follow. Some of the challenges faced in the implementation of marine conservation are discussed later in the paper, in the section on challenges and successes.
Integrating health and family planning services to become a PHE programme
The process of developing and integrating family planning services is described below. Current service provision comprises:
outreach clinics in different villages run by the Blue Ventures midwife,
community-based distribution of contraceptives and provision of basic family planning counselling by Blue Ventures’ trained community health workers
quarterly visits from Marie Stopes Madagascar’s mobile outreach team offering long-acting and reversible methods of contraception, and
reproductive health education.
Blue Ventures’ conservation workers saw first-hand their partner communities’ lack of access to contraceptive services and the strain that high fertility levels were placing both on local families and their coastal resources. Of the 25 villages within Velondriake, condoms were only available in the village of Andavadoaka.Citation28 State-run health clinics in the region suffered chronic staff and supply shortages, and three out of the four state-run clinics in the Velondriake LMMA were staffed solely by male health workers, a major barrier to access reported by many women in the region. Due to its geographical isolation, there was no non-governmental health organisation (NGO) presence in the region to fill the gap in service provision.
In 2007, 56% of girls living within the Velondriake LMMA aged 15–19 already had children or were pregnant – placing them at highest risk of maternal and infant mortality.Citation15 Surveys showed that most girls became pregnant before the age of 16, with 20% of births in the previous year being from young women under the age of 18 (Blue Ventures, unpublished data). Women were having an average of seven children, despite indicating that they did not plan or want to have such large families.Citation28
In regular, informal discussions with community representatives, including representatives from women’s groups, and in discussions at Velondriake LMMA meetings, communities expressed a strong desire for improved access to family planning services. Responding to these informal discussions, focus groups were held with groups of women and with adolescent girls, set up specifically to discuss reproductive health and family planning. These groups comprised 6–8 girls or women each, and were facilitated by a trained health care professional and a local staff member trained in group facilitation. The focus groups were complemented by large group discussions, held separately with groups of men and women, and adolescent boys and girls, aimed at facilitating discussions about reproductive health and family planning. These discussions were held over a six-month period and included approximately 20% of the population of Andavadoaka, as well as small numbers of representatives from all the LMMA villages. These discussions all unearthed a significant unmet need for contraceptive services and a general lack of awareness about contraception, with women clearly articulating a wish for Blue Ventures to facilitate provision of these services. Importantly, it also clearly identified a broad absence of social barriers and resistance to offering contraception to those who wanted to use it.Citation28
Training session for community-based distributors

In 2007, with the approval of community leaders and government health bodies, Blue Ventures opened the Velondriake LMMA’s first family planning clinic in the village of Andavadoaka, staffed initially by an expatriate health care professional employed by Blue Ventures (whose primary role had been to provide health care to Blue Ventures staff and volunteers). This new service empowered local couples to freely choose the number and spacing of their births, and so the project came to be known as Safidy, which means ‘the freedom to choose’ in Malagasy. On the opening day of the family planning clinic, 20% of all women of reproductive age in Andavadoaka attended, requesting contraception (Blue Ventures, unpublished data).
In 2009, against the backdrop of the political crisis and in spite of the more challenging working conditions that ensued, a dedicated Safidy clinician was recruited, initially a local clinical technician practising under the supervision of the Blue Ventures health professional. In 2013 she moved to work with the Blue Ventures fisheries team and was replaced by a midwife. The family planning service was gradually expanded from 2009 to 2011 to include outreach clinics in nine villages within the Velondriake LMMA, with Blue Ventures staff travelling by boat or oxcart to deliver services in these villages. In order to ensure that couples in all 25 villages within the LMMA had access to contraceptive services, local women were trained to serve as community-based distributors of contraceptives. Training was delivered in partnership with Population Services International, who have expertise in community-based distribution models.
Thirty-three women (community representatives with no previous medical training) were trained and supported to offer contraceptive methods to couples in their own and neighbouring villages. Contraceptive methods were provided to them at cost price to sell at the nationally fixed and affordable retail price, enabling them to generate a small income from this otherwise voluntary work, a model which has proven capable of delivering high quality family planning services.Citation31 They were also trained by Blue Ventures staff to offer antenatal and post-natal education. By using this social enterprise model of community-based distribution alongside the family planning clinics, the programme was able to grow to cover 40 villages along Madagascar’s southwest coastline, providing services to a total of 12,000 people. The 15 villages that are not part of the Velondriake LMMA fall within areas where other conservation groups have started similar community-based conservation programmes. Blue Ventures’ extension of health services into these new areas therefore means that the integrated PHE approach is implemented throughout this extended area.
Ensuring the community-based distributors (CBDs) remain motivated to provide services for such a modest income continues to prove challenging. So far this has been tackled by ensuring regular follow-up training for CBDs, for which they are paid to attend, and close supervision and support from the Safidy team.
In the family planning clinics, opened in ten villages, the Blue Ventures midwife is able to offer the combined oral contraceptive pill, the progestogen-only pill, the injectable Depo-Provera, and condoms. Contraceptive services are complemented by antenatal and post-natal care, and prenatal counselling. (Intra partum care is currently not being provided; the reasons for this are discussed in the following section.) The CBDs are able to offer the combined oral contraceptive pill and condoms, with 10 CBDs trained to administer Depo-Provera according to clinical guidelines, with regular supervision from the midwife.Citation28 To further extend the range of contraceptive options available, Blue Ventures has partnered with Marie Stopes Madagascar, who send mobile outreach teams to visit on a quarterly basis to offer contraceptive implants and intrauterine device fittings and removals, with the Blue Ventures midwife offering aftercare.
Feedback on contraception use and acceptability is sought regularly by the midwife and community based distributors. With this range of different methods now available, women will frequently switch methods until they have found a method they are happy with, often continuing to use contraception until they wish to become pregnant (Caroline Savitsky, Safidy Coordinator, personal communication, April 2014). Breakthrough bleeding, a symptom which arouses significant fear amongst the women in the region, is one the commonest reasons for discontinuation or switching of a contraceptive method (Laura Faranarindra, Safidy Midwife, personal communication, August 2013).
Analysis of client data suggests that women below the age of 25 are using the services less than women over 25, with very few nulliparous women using the service (Blue Ventures, unpublished data). Waiting to use contraception until after having had at least one child, and thus being sure they are fertile, appears to be common practice among women in the region (Caroline Savitsky, Safidy Coordinator, personal communication, April 2014). This practice may impact upon the programme’s ability to reduce pregnancy in girls aged 18 or under.
Health services are complemented by a community education programme, designed to support the adoption of healthier behaviours and empower couples to make their own reproductive choices. Interventions target people at all stages of the behaviour change process, from raising awareness to influencing attitudes and encouraging the sustained adoption of healthier practices. Messages and activities are specifically tailored for various demographic groups, profiled according to gender and age. The educational programme has been developed with input from the local Safidy team and UK-based support staff, combining international best practice for behaviour change communication with social marketing principles to develop locally meaningful interventions. Implementation is overseen by the local Safidy health education officer, and draws upon input from all Safidy and Blue Ventures staff, community-based distributors and other community members.
The mainstay of the educational programme is the village outreach tour. Every three months, health and conservation staff travel to 20 villages and engage communities in integrated education topics including family planning, maternal and child health, sustainable fisheries management, alternative coastal livelihoods and marine conservation. Tours comprise classroom teaching sessions and presentations for the whole village, including interactive group discussions, the use of educational films and songs, and personal testimonies. Combining health and environmental messages enables educational messages to reach a much broader audience. For example, men are engaged in reproductive health issues by linking family planning and family size with food security concerns, while women, who may have attended to hear about family planning, also get to learn about natural resource management. Other educational interventions include radio broadcasts, the production of merchandise such as T-shirts and sarongs with social marketing messages, annual football tournaments to engage young men, and small group discussions with youth clubs and women’s groups.
Having been working in the region for four years before starting to offer health care, Blue Ventures has been able to offer services in a way that demonstrates a respect for and understanding of Vezo culture and traditions. This has included ensuring that clinics are held once women are back from gleaning for octopus, maintaining an awareness of fishermen’s migratory patterns so that couples are issued with adequate supplies of contraceptives in line with annual migrations and ensuring that men’s wishes about family size are taken into consideration. Traditionally women defer to men’s wishes about family size. Women using the service seldom state that they have completed their families, preferring instead to assert that they are simply spacing their children by using contraception, regardless of age or parity, and that their husband will decide if he wants more children. The impact on total fertility of providing this service has yet to be established.
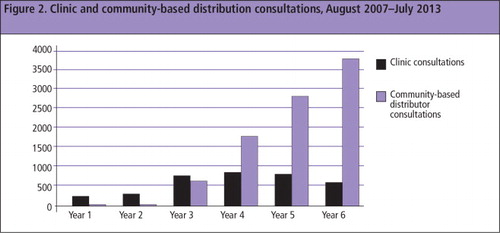
During the first six years of the programme, 9,730 months of oral contraceptives, 3,101 Depo-Provera injections, 293 implanon implants and 60 intra-uterine devices were provided to approximately 3,000 women of reproductive age during the first six years of the programme, August 2007–July 2013. shows couple-years of protection of contraceptive methods distributed during those six years. Long-acting reversible methods were introduced the third year. shows the total number of consultations for contraception during those years. The community-based programme was introduced in the third year, resulting in many more consultations overall.
Figure 1 Couple-years of contraceptive protection provided, August 2007–August 2013.
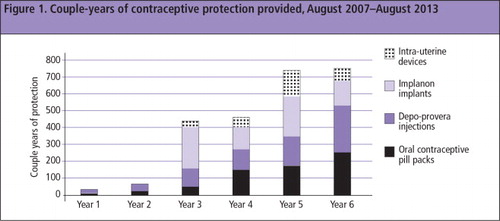
Figure 2 Clinic and community-based distribution consulations, August 2007–July 2013.
Integration of health services and education completes the PHE model: biodiversity conservation, livelihood diversification, health and education. While this model clearly does not address all the needs of the community, nor all the threats to the ecosystems upon which they depend, it represents an attempt to think and act more holistically than traditional single-sector approaches.
Challenges and successes of this integrated approach
Integrating health interventions into environmental programmes helps conservationists with a common problem: namely, the difficulty of sustaining long-term community engagement in conservation work. Even successful conservation initiatives produce relatively few short-term benefits for communities. Within the Velondriake LMMA, rapid economic gains resulting from temporary octopus closures fuelled community interest in more ambitious marine conservation initiatives; however, securing buy-in for the LMMA itself has proved more challenging, as the benefits of restrictions on destructive fishing practices or creating permanent marine reserves are less immediately apparent. Engaging women in natural resource management, traditionally a domain dominated by men, has proved particularly difficult until recently.
In contrast, family planning services are empowering couples to take immediate control over their own fertility, offering much more obvious and tangible benefits to themselves and their families. With the two initiatives intertwined, the immediacy of family planning service benefits can help to bolster the long-term support needed for the ‘slow-burn’ progress of conservation initiatives. Conservation colleagues within Blue Ventures have said that the provision of health services is helping to strengthen support for the LMMA (Shawn Peabody, In-Country Director, personal communication, August 2012).
Integrating family planning services into their work is also offering conservationists many more entry points and opportunities for engaging with communities and, should couples choose to space or limit the number of their children, will help to reduce human pressure on ecosystems. Healthier, more engaged communities are more likely to be effective custodians of the natural resources upon which their livelihoods depend, increasing the likelihood that biodiversity conservation efforts will lead to sustainable natural resource management. Reports from other PHE programmes suggest that when women are able to manage their fertility, they gain a greater sense of self-efficacy, and have more time and confidence to engage in educational, economic and natural resource management activities.Citation32 Initial indications from within the LMMA suggest that women are indeed taking greater interest in decisions about natural resource use (Caroline Savitsky, Safidy Coordinator, personal communication, August 2013). This is considered to be important, as experience from conservation programmes elsewhere has shown that greater women’s involvement has enhanced programme effectiveness.Citation33
Integrating health services into an existing conservation programme has enabled Blue Ventures to deliver family planning services to remote communities, to a degree not managed by government agencies or NGOs. Because of the trust that Blue Ventures has earned from communities in the Velondriake LMMA, and because Blue Ventures is meeting an expressed need, the team has received universal support for providing these services, resulting in their rapid uptake. By utilising the organisation’s pre-existing communications and transport infrastructure, and through effective coordination of activities between different programmes, the initial costs of offering contraceptive services in the area were kept to a minimum, allowing time to raise funds for consolidation and expansion of these services. In addition, Blue Ventures has found that working in an integrated way generates significant community awareness about the links between reproductive health, family size and food security. Community surveys conducted in 2013 showed that 82% of the population now think that using family planning will enable them to better provide for their families (Blue Ventures, unpublished data). Whether couples will actually choose to have fewer children as a result of this will require longer term follow up and monitoring of total fertility rates.
The greatest challenge faced by Blue Ventures health workers has proven to be the lack of adequate state-provided health care. Effective coordination with public health services, particularly relating to the provision of safe birthing care for the women for whom Blue Ventures provides antenatal and post-natal care, has proven to be difficult. Resource limitations and poor transportation links between the 40 villages covered means that it is not possible for the Blue Ventures midwife to provide intrapartum care herself. As a result, serious unmet reproductive health needs remain for the women of the region, and this is likely to limit improvements in health outcomes.Footnote*
Another unexpected challenge to providing safe and reliable family planning services has been the intermittent appearance of travelling “medicine sellers”. These are people with no medical or pharmacological training who sell a variety of medications without offering any form of clinical supervision or appropriate advice, including oral and injectable contraceptives. These visits are only discovered by Safidy staff when women come to clinics for aftercare, or come with questions about their contraceptives, having been given inappropriate advice by these sellers. Encouraging women to think of Safidy as providing contraceptive services, and that this has value over and above simply buying a contraceptive of their choice when a medicine seller passes through, remains an important aim of Blue Ventures’ educational programme.
Conclusion
Quite apart from the strong conceptual rationale for tackling the interconnected challenges of unmet health needs and environmental degradation in a holistic way, there is increasing evidence of the benefit of taking an integrated approach.Citation1–3 Integrating family planning and other health services into conservation projects to form PHE programmes has the potential to provide practical, immediate and long-lasting benefits in poverty reduction, health, gender equity, food security, biodiversity conservation and resilience to climate change.Citation28 It also provides governments and the international family planning community with a mechanism for delivering services to remote and under-served communities in areas of high biodiversity. For those working to ensure universal access to reproductive health, innovative models such as PHE must be considered.
Acknowledgements
Thanks to all staff of Blue Ventures Conservation, Andavadoaka, and in particular to Caroline Savitsky and Safidy staff members. Special thanks to Laura Robson for editorial input. Blue Ventures’ community health programme has been funded by the John D and Catherine T MacArthur Foundation, UN Population Fund Madagascar, US Agency for International Development and Leona M and Harry B Helmsley Charitable Trust. It has been implemented with support from Marie Stopes Madagascar, Population Services International and the Madagascar Ministry of Health.
Notes
* Nationally, Madagascar’s maternal mortality ratio currently stands at 440 deaths per 100,000 live births, with the 2015 target being 178.Citation34
References
- L D’Agnes, H D’Agnes, JB Schwartz. Integrated management of coastal resources and human health yields added value: a comparative study in Palawan (Philippines). Environmental Conservation. 37(4): 2010; 398–409.
- T Belachew, M Sinaga, A Mohammed. Effectiveness of the PHE approach for achieving family planning and fertility outcomes in Ethiopia: a comparative study in the Gurage zone. MEASURE Evaluation PRH Working Paper Series. 2013. http://www.cpc.unc.edu/measure/publications/wp-13–134
- J Pielemeier, L Hunter, R Layng. Assessment of USAID’s population and environment projects and programming options. 2007; Global Health Technical Assistance Project: Washington, DC.
- BT Johnson, CA Redding, RJ DiClemente. A network-individual-resource model for HIV prevention. AIDS and Behavior. 14(2/Suppl): 2010; 204–221.
- N Myers, RA Mittermeier, CG Mittermeier. Biodiversity hotspots for conservation priorities. Nature. 403: 2000; 853–858. http://www.nature.com/nature/journal/v403/n6772/full/403853a0.html.
- G Sedgh, R Hussain, A Bankole. Women with an unmet need for contraception in developing countries and their reasons for not using a method. Occasional Report No.37. 2007; Guttmacher Institute: New York.
- World Bank News. Madagascar: Measuring the impact of the political crisis. 5 June 2013. http://www.worldbank.org/en/news/feature/2013/06/05/madagascar-measuring-the-impact-of-the-political-crisis
- IRIN News. Madagascar: A poor country gets poorer. 18 March 2011. http://www.irinnews.org/report/92236/madagascar-a-poor-country-gets-poorer
- IRIN News. Madagascar: A decaying health sector. 25 May 2012. http://www.irinnews.org/report/95533/madagascar-a-decaying-health-sector
- World Bank data. Health expenditure per capita (current US$). 2013. http://data.worldbank.org/indicator/SH.XPD.PCAP/countries
- Royal Society Policy Centre. People and the Planet. Royal Society Science Report, 26 April 2012.
- JG Cleland, RP Ndugwa, EM Zulu. Family planning in sub-Saharan Africa: progress or stagnation?. Bulletin of World Health Organization. 89: 2011; 137–143. 10.2471/BLT.10.077925.
- J Bongaarts. Fertility transitions in developing countries: progress or stagnation?. Studies in Family Planning. 39(2): 2008; 105–110.
- Population Division Department of Economic and Social Affairs United Nations. World Population Prospects: the 2010 Revision. http://esa.un.org/wpp/Documentation/pdf/WPP2010_Volume-I_Comprehensive-Tables.pdf
- Institut National de la Statistique ICF Macro. Enquête Démographique et de Santé de Madagascar 2008–2009, Antananarivo, Madagascar: INSTAT and ICF Macro, 2009. http://www.instat.mg/pdf/eds2008-2009.pdf
- A Black-Michaud, F de Meulder. Randrianasolo, et al. Rapport d’Evaluation de l’Intervention Prolongée de Secours et de Redressement à Madagascar (Ipsr 10442.0)–Aide Pour Faire Face aux Catastrophes Naturelles et à l’insecurité Alimentaire Saisonnière (Juillet 2006–Juin 2009). 2009; World Food Programme: Rome.
- S Goodman, J Benstead. Updated estimates of biotic diversity and endemism for Madagascar. Oryx. 2005; 39. http://bama.ua.edu/˜jbenstead/Publications_files/Madagascar%20biodiversity%20copy.pdf.
- TM Brooks, RA Mittermeier, GAB da Fonseca. Global biodiversity conservation priorities. Science. 313: 2006; 58–61.
- World Wildlife Fund. Madagascar, West Indian Ocean Programme Office. Treasure Island: New biodiversity on Madagascar, 1999–2010. http://assets.wwf.org.uk/downloads/madagascarspeciesreport.pdf
- PR Ehrlich, RM Pringle. Where does biodiversity go from here? A grim business-as-usual forecast and hopeful portfolio of partial solutions. Proceedings of the National Academy of Sciences of the United States of America (PNAS). 105: 2008; 11579–11586.
- JK McKee, PW Sciulli, CD Fooce. Forecasting global biodiversity threats associated with human population growth. Biological Conservation. 115(1): 2004; 161–164.
- SD Gehrt. The human population problem: educating and changing behaviour. Conservation Biology. 10: 1996; 900–903.
- United Nations Framework Convention on Climate Change. http://unfccc.int/resource/docs/napa/mdg01f.pdf
- K Hardee, C Mutunga. Strengthening the link between climate change adaptation and national development plans: lessons from the case of population in National Adaptation Programmes of Action (NAPAs). Mitigation and Adaptation Strategies for Global Change. 15(2): 2009. http://www.unfpa.org/webdav/site/global/users/schensul/public/CCPD/papers/Hardee%20and%20Mutunga%20Paper.pdf.
- L Gaffikin. Scaling up population and environment approaches in Madagascar: a case study. 2008. http://www.k4health.org/sites/default/files/crc11_Gaffikin_WWFScaleUpMadag.pdf
- A Cooke, O Ratomahenina, E Ranaivoson. Madagascar. C Sheppard. Seas at the Millennium: An Environmental Evaluation. Vol. 2 Ch.60: 2000; Elsevier Science Press: Oxford, 113–131.
- A Harris. Out of sight but no longer out of mind: a climate of change for marine conservation in Madagascar. Madagascar Conservation & Development. 6(1): 2011; 6–14. http://www.ajol.info/index.php/mcd/article/download/68058/56150.
- A Harris, V Mohan, M Flanagan. Integrating family planning service provision into community-based marine conservation. Oryx. 46(2): 2012; 179–186.
- A Harris, G Manahira, A Sheppard. Demise of Madagascar’s once great barrier reef – change in coral reef condition over 40 years. Atoll Research Bulletin. 574: 2010; 1–18.
- A Harris. “To live with the Sea” Development of the Velondriake Community-Managed Protected Area Network, Southwest Madagascar. Madagascar Conservation and Development. 2: 2007; 43–49.
- MF Gallo, J Walldorf. Kolesar R, et al. Evaluation of a volunteer community-based health worker program for providing contraceptive services in Madagascar. Contraception. 88(5): 2013; 657–665. 10.1016/j.contraception.2013.06.008.
- World Wildlife Fund. Healthy People, Healthy Ecosystems – A Manual on Integrating Health and Family Planning into Conservation Projects. 2008; WWF: Washington, DC.
- B Agarwal. Gender and forest conservation: the impact of women’s participation in community forest governance. Ecological Economics. 68: 2009; 2785–2799.
- UN Population Fund. The State of the World’s Midwifery 2011, Madagascar country profile, p.98. http://www.unfpa.org/sowmy/resources/docs/country_info/profile/en_Madagascar_SoWMy_Profile.pdf