Abstract
Introduction
The soleus muscle is a powerful plantar flexor of the ankle joint and receives its blood supply from several different sources.
Aim
This study was done to describe the distribution of the arterial supply of the soleus muscle.
Materials and methods
The study was carried out at the Faculty of Medicine, University of Alexandria. Forty limbs were dissected, which included specimens from both male and female cadavers. The pattern of arterial supply of the soleus muscle and the distribution of the perforators were studied.
Results
The soleus muscle is supplied by perforators of the popliteal, posterior tibial and peroneal arteries, the posterior tibial artery gave 38.80% of total perforators while the peroneal artery gave 33.30% of total perforators and the popliteal artery gave 27.80% of total perforators. Perforators of popliteal artery were larger; 12.9 ± 2.07 cm in length and 2.55 ± 0.214 mm in diameter while those of the posterior tibial artery had a length of 5.1 ± 0.99 cm and a diameter of 1.93 ± 0.25 mm and perforators of the peroneal artery had a length of 3.8 ± 0.98 cm and a diameter of 1.49 ± 1.03 mm.
Conclusion
The soleus muscle is richly supplied by many arterial pedicles and can be used safely as a free flap, hemisoleus flap or composite flap to cover defects in the lower limb.
1 Introduction
The soleus is a bipiniform (double feather) shaped muscle; its width encompasses the posterior two-thirds of the calf. It originates from the upper one-third of the dorsum of the fibula and mid-posterior tibia and inserts into the tendocalcaneus.Citation1 When the muscle is freed from its insertion and based proximally, covers defects into the mid-tibia and has become the flap of choice for coverage of distal tibial defects.Citation2
Its blood supply according to the classification of Mathes and Nahai Citation3 is type II: it is supplied by large dominant vascular pedicles from the popliteal artery superiorly and the posterior tibial and the proximal part of peroneal arteries inferiorly and minor pedicles from the posterior tibial and distal part of peroneal arteries so the muscle can be used in various ways to create different types of flaps according to its vascular supply.Citation1,Citation4
The management of lower extremity trauma has evolved over the last two decades to the point that many extremities that would have required amputation are routinely salvaged.Citation5,Citation6 This is mainly because of better understanding of anatomy and vascular patterns of the areas, resulting in expansion of available choices to cover a wider range of defects. Free tissue transfer has become a gold standard option for large complex defects of lower limb.Citation5 Soleus muscle flap can be proximally or distally based, hemisoleus flap or composite flap. All these flaps are based on the vascular supply of the muscle. Citation7
The aim was to study the patterns of the vascular supply of the soleus muscle.
2 Materials and methods
Forty cadaveric lower limbs were obtained from the Anatomy Department of Alexandria University to study the vascular supply of soleus. The limbs were taken from male and female cadavers equally. Injection of latex into the popliteal artery in the popliteal fossa was done after ligation of the artery proximally. Dissection commenced two weeks after latex injection. A longitudinal incision was made along the posterior midline of the leg; then the skin, superficial fascia and deep fascia were reflected on both sides to identify both heads of gastrocnemius.
Both heads of gastrocnemius were cut and reflected upwards and downwards or split longitudinally and reflected medially and laterally to show the superficial surface of soleus muscle. Branches from the popliteal artery supplying the muscle were identified. The soleus muscle was dissected more deeply through an incision along its midline to identify the branches to the deep surface. Branches of the tibial and posterior tibial nerves accompanying the vessels were also identified; then the soleus muscle was cut transversely at the upper border of tendocalcaneus and the upper part of the muscle was reflected upwards, while the lower part was left inserted into tendocalcaneus. Branches from the posterior tibial artery were identified supplying the medial and lower parts of the muscle while the branches of the peroneal artery were identified supplying the lateral part of the muscle. Measurements of the length (at the origin from the main artery) and diameter (at the entrance into the muscle) of the muscular perforators of different arteries using vernier caliber was done.
Statistical analysis of the number and distribution of different perforators (muscular branches) in relation to sex was done.Citation8. The data was collected and entered into the personal computer. Statistical analysis was done using Statistical Package for Social Sciences (SPSS/version 17 software). Arithmetic mean and standard deviation were calculated. For categorized parameters, Chi square test was used while for numerical data t-test was used to compare the two groups. The level of significant was 0.05.
3 Results
In all the limbs, the arterial blood supply of soleus muscle was from the popliteal, peroneal and posterior tibial arteries. The posterior tibial artery gave 38.80% of total perforators, while the peroneal artery gave 33.30%. The popliteal artery gave 27.80% of total perforators (the least number of perforators). There was a little statistically non-significant difference between the number of perforators in relation to sex (P = 0.966) ().
Table 1 Distribution of different studied perforators in relation to sex.
In all cases, the popliteal artery in the popliteal fossa gave at least one or two muscular branches that entered and supplied the middle of the proximal part of the superficial surface of the muscle and further divided into several medial and lateral branches that supplied the deep part of the muscle and stopped 5 or 6 cm above the insertion of the muscle (–). The popliteal artery in four cadavers gave three main vascular pedicles to the lateral, middle and medial parts of soleus muscle (). Branches of tibial nerve were seen accompanying the muscular branches of popliteal artery (–). There was no statistically significant difference between males and females as regards the length and diameter of the muscular perforators of the popliteal artery to soleus ().
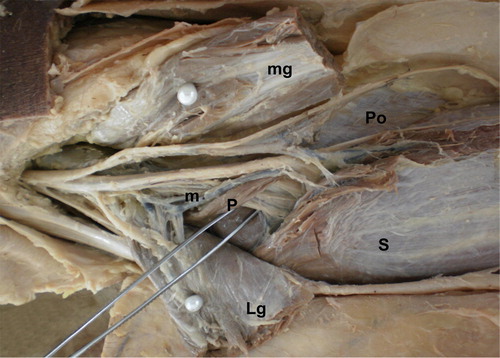
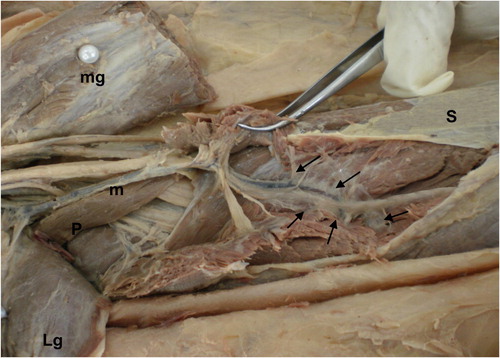
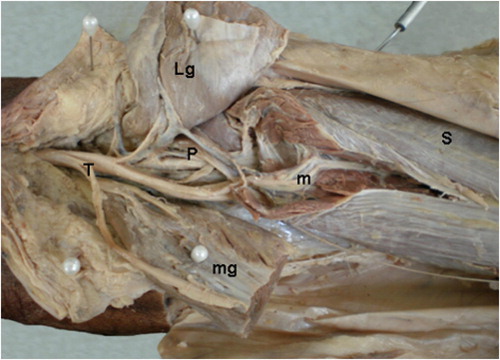
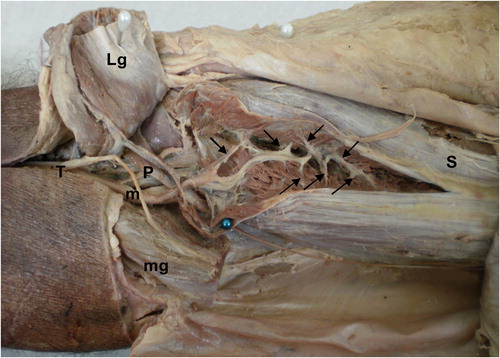
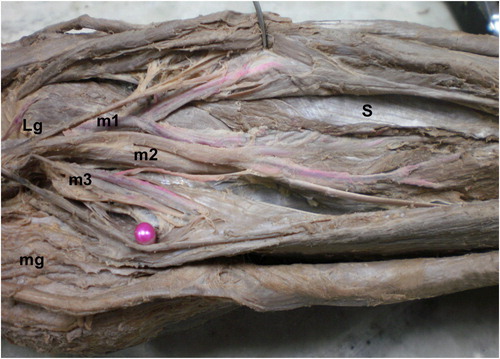
Table 2 Comparison between length and diameter of muscular branches of popliteal artery in both male and female.
In all cases, the medial part of soleus was supplied by muscular branches of the posterior tibial artery through its deep surface (–). An average of three muscular perforators entered the muscle through its deep surface and supplied the upper, middle and lower parts of the muscle and even supplied tendocalcaneus (). In two legs, the perforators entered the muscle through its medial border (). There was no statistically significant difference between males and females as regards the length and diameter of the muscular perforators of the posterior tibial artery (). The mean distance of the perforators of the posterior tibial artery from the medial malleolus was 14.17 ± 6.65 cm in males and 14 ± 7.02 cm in females with no significant difference (P = 0.316) ().
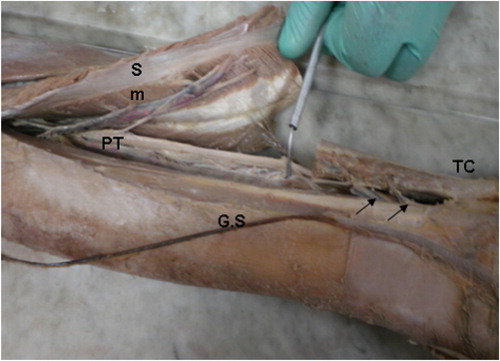
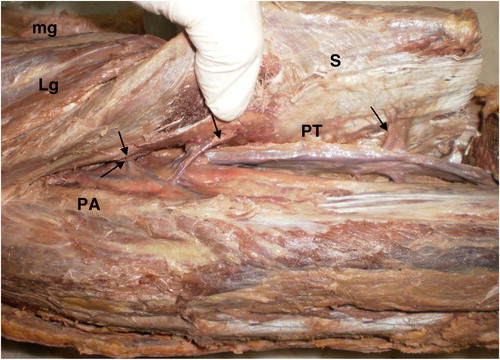
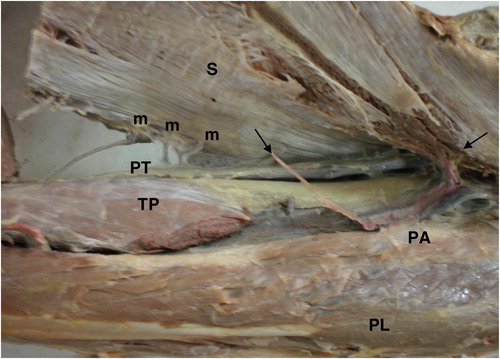
Table 3 Comparison between length and diameter of muscular branches of posterior tibial artery in both male and female.
Table 4 Comparison between the distance of muscular branches of posterior tibial artery from medial malleolus in male and female in cm.
In all cases, the soleus muscle was supplied by muscular branches of peroneal artery; two or three perforators supplied the lateral part of the muscle through its deep surface (–). Perforators of the peroneal artery also supply the fibula and the overlying skin (). In two cadavers, the perforators of the peroneal artery passed through the lateral border of the muscle (). There was no statistically significant difference between males and females as regards the length and diameter of the perforators of the peroneal artery (). The mean distance of the perforators of the peroneal artery from the lateral malleolus was 11.45 ± 4.06 cm in males and 11.56 ± 4.28 cm in females with no significant difference (P = 0.448) (). Perforators of popliteal artery were the largest; 12.9 ± 2.07 cm in length and 2.55 ± 0.214 mm in diameter. Perforators of the posterior tibial artery had a length of 5.1 ± 0.99 cm and a diameter of 1.93 ± 0.25 mm. Perforators of the peroneal artery were the smallest with a length of 3.8 ± 0.98 cm and a diameter of 1.49 ± 1.03 mm.
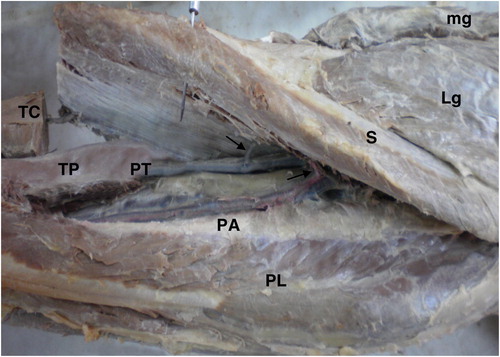
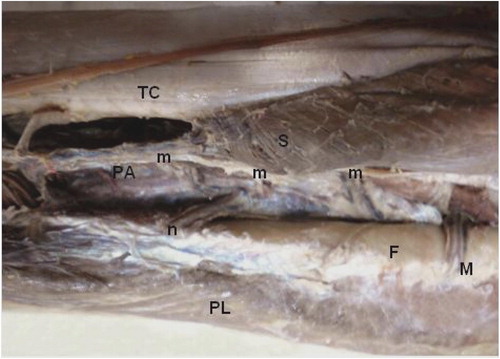
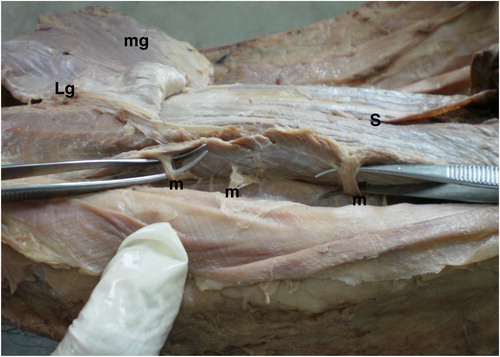
Table 5 Comparison between length and diameter of muscular branches of peroneal artery in both male and female.
Table 6 Comparison between the distance of muscular branches of peroneal artery from lateral malleolus in both male and female in cm.
There is a relatively avascular plane in the middle of the proximal part of the muscle along the superficial surface where the muscle can be divided between the medial and lateral perforators of the popliteal artery. There is another avascular plane in the distal part of the muscle along its deep surface between the perforators of the posterior tibial and peroneal arteries.
4 Discussion
The present study showed the following pattern of blood supply to the soleus muscle; the popliteal artery supplied the superficial surface of soleus through one or two muscular branches to its middle part that divided into multiple branches to supply the deep surface; this was in agreement with Mahdi et al.Citation9 who found that the vascular supply of soleus is from the popliteal artery and its major divisions in 66.7% of the limbs through two branches to the proximal part of the muscle; this was also in agreement with Taylor et al.Citation10 who stated that the soleus has a mixed blood supply from popliteal, posterior tibial and peroneal vascular pedicles to the proximal muscle, peroneal pedicles to distal lateral belly, and segmental posterior tibial pedicles to distal medial belly, they mentioned that proximal vasculature arises directly from the popliteal vessels and can reliably carry all but the distal 4–5 cm of the muscle and stated that for a proximally based soleus flap, distal perforators from posterior tibial artery are ligated and divided until the muscle can be transposed to cover the defect.
In this study, it was found that the medial part of soleus was supplied by large muscular branches of posterior tibial artery through its under surface, this was in agreement with Raveendran and KumaragamaCitation11 who found that the medial part of soleus muscle was supplied throughout its whole length by perforators arising from the posterior tibial artery and they said that this constant feature makes the medial part of the muscle reliable as a proximally or distally based flap, they also found that the average distances of the lower perforators arising from the posterior tibial artery were 6.5, 11.6 and 16.8 cm from the medial malleolus. While in this study, the mean distance of the muscular branches from the medial malleolus was 14.17 ± 6.65 cm in male and 14 ± 7.02 cm in female and the range was from 6 to 24 cm. Mahdi et al.Citation9 mentioned that the posterior tibial artery gave a series of branches (3–6) with a mean of 4.3 ± 0.7 to soleus throughout its course along the muscle and the mean distance from the medial malleolus was 15 ± 3.4 cm which was in agreement with our findings. Sadasivan et al.Citation12 identified two vascular patterns: a segmental posterior tibial artery (type 1) and a proximally dominant posterior tibial artery (type 2); type 1 was seen in 77.8% of cases, and type 2 in 22.2% of cases. PuCitation13 used the medial hemisoleus flap based on these large perforators to cover defects in the middle or distal third of the leg without sacrificing the prime ankle flexor. Knowing the sizes and the sites of the muscular perforators is of great importance for plastic surgeons to plan their flaps accurately.
In the present work, it was found that the peroneal artery supplied the lateral part of soleus by multiple branches (about three) and also itself supplied the deep part of the muscle, these perforators pass through the deep surface or the lateral border of the muscle and this was in agreement with the results of Dominique et al.Citation14 who found a main pedicle for the lateral soleus emerging from the peroneal artery, and in all cases the blood supply of the proximal part of the muscle was of segmental distribution by way of multiple branches originating from the peroneal artery, they raised soleus flaps with distal pivot point represented by the perforating branch of the peroneal artery to cover an ankle and dorsal foot defect up to the metatarsal heads. Raveendran and KumaragamaCitation11 stated that the branches of the peroneal artery were mostly distributed in the upper half of the muscle; these large pedicles allow a composite transfer of the soleus with the fibula, lower perforators were demonstrated to arise from the peroneal artery in 60% of limbs but the scarcity of perforators in this region limits the clinical usefulness of an inferiorly based lateral hemisoleus flap.
The soleus is a powerful plantar flexor of the ankle. At least half of the muscle is needed to maintain its action. Therefore a hemisoleus muscle flap after splitting the muscle longitudinally at the level of the midline raphe thus saving as much perforators and as much muscle as possible is the best choice.Citation15 Our results as well as TobinCitation16 demonstrated an intramuscular septum as a distinct watershed in the blood supply of the proximal half of the muscle and fine vascular communications between intramuscular vascular territories. Fayman et al.Citation17 demonstrated significant vascular communications between the medial and lateral systems contradicting most of the studies and suggesting careful dissection and ligation of communicating vessels during hemisoleus flap. Therefore the medial hemisoleus flap as well as the lateral soleus–fibula free transfer flap can be used to cover defects on the medial or the lateral sides of leg and foot, respectively.Citation13,Citation18,Citation19
The lack of significant difference between male and female in our results could be explained by the small sample size and the old age of the cadavers.
5 Conclusion
The proximal part of soleus is supplied by the popliteal artery and this constitutes the basis of the proximally based soleus flap. The main blood supply of the medial part of the muscle is from the posterior tibial artery through large and constant perforators and this constitutes the basis of the medial hemisoleus flap. The main blood supply of the lateral part of the muscle, its overlying skin and the fibula is from vascular pedicles of the peroneal artery and this constitutes the basis of the soleus–fibula free transfer flap.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 26 June 2012
References
- A.WilliamsR.L.M.NewellM.S.DaviesThe legS.StandringGray's anatomy39th ed.2005Elsevier Churchill LivingstoneNew York, Edinbrugh and London1500
- A.R.KumarStandard wound coverage techniques for extremity war injuryJ Am Acad Orthop Surg142006862865
- S.J.MathesF.NahaiClinical application for muscle and musculocutaneous flaps1982CV MosbySt. Louisp.87
- D.J.MackenzieA.E.SayferReconstructive surgery: lower extremity coverageS.J.MathesV.R.HentzPlastic surgery2nd ed2006Saunders ElsevierPhiladelphia13551381
- A.K.KasabianN.S.KarpLower extremity reconstructionC.H.ThomeR.W.BeasleyJ.S.AstonS.P.BartlettGrabb and Smith's plastic surgery6th ed2007Williams & WilkinsPhiladelphia, Lippincott676688
- C.A.MareckO.PullRefinements of free tissue transfer for optimal outcome in lower extremity reconstructionAm Plast Surg522004270275
- G.G.HallockGetting the most from the soleus muscleAm Plast Surg361996139146
- J.F.JekelEpidemiology, biostatistics, and preventive medicine1996W.B. Saunders CompanyPhiladelphia
- F.MahdiM.H.AzarA.A.KheradmAnatomy of arterial supply of the soleus muscleActa Med Iran4942011237240
- G.I.TaylorJ.H.PalmerThe vascular territories of the body: experimental study and clinical applicationsBr J Plast Surg4021987113141
- S.S.RaveendranK.G.J.L.KumaragamaArterial supply of the soleus muscle. Anatomical study of fifty lower limbsClin Anat162003248252
- K.K.SadasivanJ.T.OgdenJ.A.AlbrightAnatomic variations of the blood supply of the soleus muscleOrthopedics1461991679683
- L.L.Q.PuFurther experience with the medial hemisoleus muscle flap for soft tissue coverage of a tibial wound in the distal third of the legPlast Reconstr Surg121200820242028
- L.DominiqueC.RizzoW.HuThe island hemisoleus flap on distal vascular pedicle: anatomical bases and clinical applicationsSur Rad Anat3192009715721
- A.HagM.N.TararF.S.MalikHemisoleus muscle flap, a better option for coverage of open fractures involving middle third of tibiaJ Ayub Coll Abbottabad2142009154158
- G.R.TobinHemisoleus and reversed hemisoleus flapsPlast Reconstr Surg76119858796
- M.S.FaymanF.OrakB.HugoS.D.BersonThe distally based split soleus muscle flapBr J Plast Surg401119872026
- P.PelissierV.CasoliE.DemiriD.MartinSoleus–fibula free transfer in lower limb reconstructionPlast Reconstr Surg10522000567573
- D.C.ChuangH.C.ChenF.C.WeiM.S.NoordhoffCompound functioning free muscle flap transplantation (lateral half of soleus, fibula and skin flap)Plast Reconstr Surg8921992335339