
Abstract
Background
Colorectal cancer (CRC) is the third most common cancer worldwide after lung and breast cancers with two-thirds of all CRCs occurring in the more developed regions of the world. CRC affects men and women of all racial and ethnic groups, and is most often found in those aged 50 years or older.
Aim
The aim of the study was to determine the prevalence of CRC among patients undergoing colonoscopy in Egypt.
Materials and methods
This was a descriptive cross-sectional hospital-based study. A total of 412 consecutive patients who underwent planned pancolonoscopy from January 2000 to January 2012 at our institution were assessed. All endoscopic examinations leading to a diagnosis of CRC were evaluated. The following parameters were analyzed: frequency of CRC, patient characteristics, indication for endoscopic examination, endoscopic findings, localization of CRC and histopathology.
Results
CRC was diagnosed in 57 patients (14% of all colonoscopies). Fifty-six percent were female. The mean age was 51 ± 15 years (age range: 16–80 years). Twenty-five percent of cancers occurred in patients aged less than 40 years. The most frequent indication for colonoscopy was rectal bleeding (39%). The most common colonoscopy finding was mass (96%). Sixty-eight percent of CRC were located in the left colon and rectum. Ninety-one percent of CRC were adenocarcinoma.
Conclusions
CRC is not uncommon among Egyptian patients subjected to colonoscopy. There are relatively higher CRC rates in patients under 40 years of age than reported in the West. This has implications relating to future epidemiological trends in Egypt. Physicians must have a greater awareness of the potential for CRC in young people in the Middle East.
Abbreviation:
KEYWORDS:
1 Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide after lung and breast cancers with two-thirds of all colorectal cancers occurring in the more developed regions of the world.Citation1,Citation2 CRC affects men and women of all racial and ethnic groups, and is most often found in those aged 50 years or older.Citation3 Colonoscopy plays a central role in the detection and prevention of CRC.Citation4 In a study of 505 patients who underwent colonoscopy in the United Kingdom, CRC was detected in 2.1% of patients.Citation5 Estimates are that only 2–6% of CRC cases are found in patients 40 years or younger.Citation6–Citation7Citation8
Egypt is a developing Middle-Eastern country. Bolak Eldakror Hospital is a secondary-care governmental hospital in Giza, Egypt. The gastrointestinal endoscopy unit was set up in 1999. The aim of the study was to determine the prevalence of CRC among patients undergoing colonoscopy in our catchment’s area.
2 Materials and methods
This was a descriptive cross-sectional hospital-based study. All patients having CRC detected during colonoscopy were included in the study. Patients were referred from outpatient clinics and the medical department. Two gastroenterologists performed all colonoscopies. Pathological examination was performed by two expert pathologists.
A total of 412 consecutive patients who underwent planned pancolonoscopy from January 2000 to January 2012 at our institution were assessed. All endoscopic examinations leading to a diagnosis of CRC were evaluated. A detailed clinical history was taken. A thorough physical examination was performed. The following parameters were analyzed: frequency of CRC, patient characteristics (age and gender), indication for endoscopic examination, endoscopic findings, localization of CRC and histopathology.
3 Results
There were a total of 57 cases of CRC detected during this period, accounting for 14% of all procedures. Fifty-six percent of patients were female. The mean age was 51 ± 15 years (age range: 16–80 years). Peak frequencies were in the 5th and 7th decade (). Twenty-five percent of cancers occurred in patients aged less than 40 years. The age distribution is shown in . None of the affected patients had a history of inflammatory bowel disease or polyposis. One patient (2%) had undergone a previous operation for CRC. Two patients (4%) fulfilled the Amsterdam criteria for hereditary non-polyposis CRC. The most frequent indication for colonoscopy was rectal bleeding in 22 patients (39%). The overall indications for colonoscopy are shown in . The colonoscopy findings were mass in fifty-five patients (96%) and stenosis in 2 (4%). Thirty cancers (53%) were located in the left colon (sigmoid colon, descending colon and splenic flexure) and nine (16%) in the rectum (). Eighteen (32%) were sited in the proximal colon (cecum, ascending colon, hepatic flexure and transverse colon). Synchronous tumors occurred in one patient (2%). Histopathology revealed 52 adenocarcinoma (91%), two signet-ring cell carcinoma (4%), two mucoid carcinoma (4%) and one anaplastic carcinoma (2%). Patient characteristics, indication for colonoscopy, localization and histopathology of CRC in patients 40 years or younger are shown in .
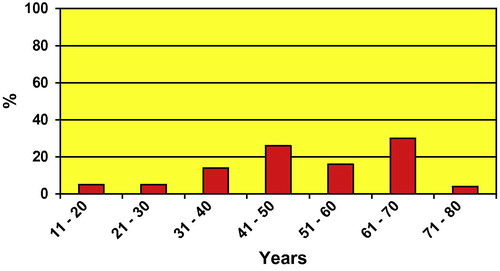
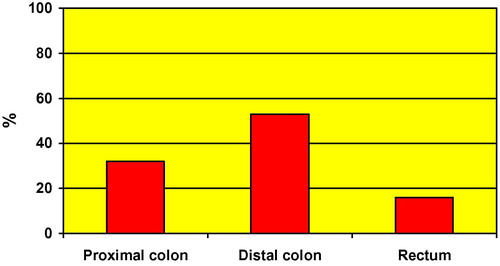
Table 1 Indications for colonoscopy in patients with colorectal cancer.
Table 2 Patient characteristics, indication for colonoscopy, localization and histopathology of CRC in patients aged 40 years or younger.
4 Discussion
CRC is a common cancer worldwide. CRC affects men and women of all racial and ethnic groups, and is most often found in people aged 50 years or older in developed countries.Citation3 No age group is exempt; an adenocarcinoma of the colon has been reported in a nine-month-old girl.Citation6
In our study, CRC accounted for 14% of all colonoscopies performed at our hospital. The mean age of patients was 51 years with 25% of cancers occurring in patients aged less than 40 years. Our data are similar to those reported in other Middle-Eastern countries and are much higher than in Western countries.
Reports from Middle-Eastern countries show a higher prevalence of CRC in patients undergoing colonoscopy than in the West. CRC was detected in 2.1% of patients who underwent colonoscopy in the United Kingdom and 9–11% in Morocco and Sudan.Citation5,Citation9,Citation10 Also reports from Middle-Eastern and African countries show higher CRC rates in younger patients than in the West. CRC was diagnosed in patients aged 40 years or younger in 2–6% of CRC cases in Italy, France and Taiwan and in 17–36% in Saudi Arabia, Sudan and Iran.Citation6–Citation7Citation8,Citation11–Citation12Citation13Citation14 In Egypt reports showed that CRC was detected in 11–15% of patients who underwent colonoscopy and diagnosed in 29–31% of patients aged 40 years or younger.Citation15–Citation16Citation17Citation18
Population based studies comparing large populations have shown that rates of CRC differ dramatically among countries, varying by as much as 10-fold, from low-incidence areas in Asia and Africa, to much higher rates in Northern Europe and the United States.Citation19–Citation20Citation21 Globally, the age-standardized incidence rate of CRC is 20.1 per 100,000 males and 14.6 per 100,000 females. The incidences of CRC in the Arab world and Middle East countries are relatively low.Citation19,Citation20 In Egypt, low rates of CRC (6.9/105 for males and 5.1/105 for females) were reported by the Middle East Cancer Consortium for the period of 1999–2001 Citation19 The low rates of CRC in Egypt were also reported from the Gharbiah cancer registry for the period of 2000–2002, where the age-standardized incidence rates for CRC were 6.5/105 for males and 4.2/105 for females.Citation21 The exceptionally high CRC rates noted in this and other hospital based studies relate to the relative paucity of screening procedures, even in symptomatic patients compared to the population as a whole.
CRC is common in the Western world and usually ranks high in incidence and mortality among malignancies in those countries.Citation19 Westernization is often associated with higher incidence rates of CRC. Diet and lifestyle factors are implicated risk factors for the disease. Fruit and vegetable-deficient diet, calorie-dense foods, physical inactivity, obesity, and smoking increase the risk for developing colorectal cancer.Citation21 While developing countries historically have a low rate of CRC, the transition to a more western diet has been associated with increasing rates of disease.Citation21 A study from South Africa showed that among patients admitted to hospital with CRC the proportion of African patients under 40 years of age was 19%; but only 4% in the white population.Citation22 The authors reported that the patients lived in Soweto and Johannesburg. In the urban context described, these Africans have considerably more advantages, socio-economically, dietary and in other respects, than their rural counterparts. The authors suggested that, with ongoing transitional changes – in diet and other factors – the relatively high proportion of younger African patients probably indicates a rising occurrence of CRC in the urban African patients with colon neoplasm. Population based studies as well as hospital based studies in Egypt and Arab countries have shown high CRC rates in patients aged 40 years or younger.Citation12,Citation13,Citation17,Citation18,Citation20,Citation21 A population based study showed that the incidence rate of CRC for those under 40 years of age in Egypt was slightly higher than the United States incidence rate for the same age group.Citation21 It is unclear if the high young-onset rate is due to adoption of a more “westernized” lifestyle and diet, particularly in the younger generation or due to intense environmental exposures with more susceptibility among the younger generations.Citation21
One concern of CRC affecting the younger population (<40 years old) is the poor prognosis attached to it.Citation23 Dukes and Bussey suggested a much higher rate of lymphatic metastasis in patients less than 40 years of age due to a more rapid progression of the disease in young patients.Citation23 Reports from Europe demonstrate that the 5 year survival rate for young patients (30 years old or younger) is only 25–30%.Citation24,Citation25 The need for early recognition of CRC in young adults is emphasized by the greater incidence of advanced disease and the high treatment failure rate.Citation26 However, if detected early, young patients with Dukes’ stage A or B lesions have better overall 5 year survival rates.Citation27 A second concern is that the high incidence of CRC in this younger age group suggests that in the Middle East we may be seeing the start of a birth cohort effect. If so the implication is that as time passes the incidence of cancer in those now aged below 40 will rise higher as they become older and those now in their twenties may have a higher incidence as they age.
All cases of CRC at our institution were referred to the National Cancer Institute for further management but unfortunately the majority was diagnosed at an advanced stage (unpublished). The factors responsible for delay in detection are underuse of diagnostic tests, late referrals for colonoscopy, under use of surveillance colonoscopy and misdiagnosis.
Detecting CRC at an early, more treatable stage is important for cure and survival. Patients presenting with altered bowel habit, rectal bleeding, anorexia and weight loss should be regarded as having alarm symptoms, suggestive of cancer, and at relatively high risk of CRC. Factors increasing the time to diagnosis are assumption that symptoms are due to hemorrhoids or irritable bowel syndrome, inadequate investigation of iron deficiency anemia and inadequate rectal or abdominal examination. The need to increase awareness about CRC in Egypt is recommended. An awareness campaign should be performed to promote detection of CRC at its earliest and most curable stage by recognizing early symptoms and enabling early referrals for colonoscopy. Those at higher risk should be offered more intensive surveillance. CRC screening can find adenomatous polyps so that they can be removed before turning into cancer. Screening also helps find CRC at an early stage, when treatment often leads to a cure. Tests recommended for CRC screening are fecal occult blood test, digital rectal examination, flexible sigmoidoscopy, colonoscopy and double-contrast barium enema test. Regarding colonoscopy there are wide variations in the expertise available to conduct colonoscopy. An adequate level of training and possibly certification for colonoscopists are required, and national standards for this are desirable. Each screening test has unique advantages, has been shown to be cost-effective, and has associated risks and limitations. Ultimately, patient preferences and availability of testing resources guide the selection of screening tests. Cost of investigations, inadequate referral centers, paucity of trained colonoscopists and cultural issues are other challenges in constructing CRC screening program.
This study showed a high prevalence of CRC in patients who underwent colonoscopy and high CRC rates in patients aged less than 40 years. Larger sample and multi-center studies are required to determine the prevalence and identify causes and risk factors of CRC in Egypt. Also further studies are required to establish criteria for a screening program and if possible to find causes of the occurrence of CRC more frequently in younger population.
In conclusion, our study showed that CRC is not uncommon among Egyptian patients subjected to colonoscopy and CRC rates are high in patients under 40 years of age. Our analysis of daily clinical practice provided valuable information as all consecutive patients of a secondary-care governmental hospital were included. The future needs of this demographic variation must be anticipated. A greater awareness of the potential for CRC in young people must be emphasized to all physicians. Further study is required to be undertaken to find out whether CRC affecting young population is due to regional factors or whether it is indicative of a changing pattern of occurrence of CRC. If the latter, additional studies are required to define genetic factors. Additional studies are also required to determine the value and cost-effectiveness of a screening program and the appropriate age for screening in a developing country like Egypt.
Conflict of interest
None declared.
Acknowledgments
The authors wish to thank Prof. El-Hindawi A, Cairo University and Prof. Akl M, Theodor Bilharz Research institute for their contribution in the pathological examination.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 12 April 2013
Related Research Data
References
- Bowel (colorectal) cancer – UK incidence statistics; 2011. March [Internet]. Available from: http://info.cancerresearchuk.org/cancerstats/types/bowel/incidence/index.htm.
- Dragovich T, Tsikitis V. Colon Cancer, Adenocarcinoma; 2012. February [Internet]. Available from: http://emedicine.medscape.com/article/277496-overview.
- CDC Data & Statistics|Feature. Top 10 Cancers Among Women; 2011. May [Internet]. Available from: http://198.246.98.21/Features/dsWomenTop10Cancers/.
- D.G.HewettC.J.KahiD.K.RexDoes colonoscopy work?J Natl Compr Canc Netw820106776
- S.Thomas-GibsonC.ThaparS.ShahB.SaundersColonoscopy at a combined district general hospital and specialist endoscopy unit: lessons from 505 consecutive examinationsJ R Soc Med952002194197
- D.CascinuE.Del FerroC.GriantiM.LigiG.CatalanoS-phase fraction and tumor aneuploidy in colorectal carcinoma of young patientsCancer78199618571860
- J.C.CusackG.G.GiaccoK.ClearyB.S.DavidsonF.IzzoJ.SkibberSurvival factors in 186 patients younger than 40 years old with colorectal adenocarcinomaJ Am Coll Surg1831996105112
- P.Y.LeeW.S.FletcherE.S.SullivanJ.T.VettoColorectal cancer in young patients: characteristics and outcomeAm Surg601994607612
- G.HassanN.KabbajL.AmraniI.SerrajM.GuediraM.NyaA Moroccan experience with colonoscopy: a review of 1157 CasesArab J Gastroenterol920088284
- H.MudawiS.NanakalyM.El TahirS.SulimanS.IbrahimIndications and findings of colonoscopy in patients presenting to the endoscopy unit at Soba University hospital in Khartoum, SudanArab J Gastroenterol112010101104
- M.AdloffJ.P.ArnaudM.SchloegelD.ThibaudR.BergamaschiColorectal cancer in patients under 40 years of ageDis Colon Rectum291986322325
- M.S.Al-AhwalA.A.Al-GhamdiPattern of colorectal cancer at two hospitals in the western region of Saudi ArabiaSaudi J Gastroenterol112005164169
- A.AbdallaM.MusaR.KhairPresentation of colorectal cancer in Khartoum teaching hospitalSudan J Med Sci242007263267
- P.PahlavanR.KanthanThe epidemiology and clinical findings of colorectal cancer in IranJ Gastrointest Liver Dis1520061519
- M.S.ZakariaA.HashemM.S.AbdelbaryA.AmerK.SeragS.LashinThe pattern of colonic diseases in Egypt: a colonoscopic studyArab J Gastroenterol720065358
- H.ElbateaM.EnabaG.ElkassasF.El-KallaA.ElfertIndications and outcome of colonoscopy in the middle of Nile Delta of EgyptDig Dis Sci56201121202123
- A.S.SolimanM.L.BondyB.LevinM.R.HamzaK.IsmailS.IsmailColorectal cancer in Egyptian patients under 40 years of ageInt J Cancer7119982630
- W.KhafagyM.El-GhazalyM.El-ShobakyM.KhafagyColorectal cancer in Egypt – does it differ?Coloproctology22000109115
- Barchana M. Colorectal cancer – middle East cancer consortium; 2006. [Internet]. Available from: http://seer.cancer.gov/publications/mecc/mecc_colorectal.pdf.
- E.SalimM.MooreJ.Al-LawatiJ.Al-SayyadA.BawazirS.BazarbashiCancer epidemiology and control in the Arab world – past, present and futureAsian Pac J Cancer Prev102009316
- D.VeruttipongA.SolimanS.GilbertT.BlachleyA.HablasM.RamadanAge distribution, polyps, and rectal cancer in the Egyptian population-based cancer registryWorld J Gastroenterol18201239974003
- A.WalkerI.SegalColorectal cancer in an African city population in transitionEur J Cancer Prev112002187191
- M.PalProportionate increase in incidence of colorectal cancer at an age below 40 years. An observationJ Can Res Ther220069799
- Y.MiyakeH.MishimaI.NishishoN.KikkawaM.MondenUse of microsatellite analysis in young patients with colorectal cancer to identify those with hereditary nonpolyposis colorectal cancerJ Surg Oncol792002157165
- A.Y.BedikianH.KantarjianR.S.NelsonJ.R.StroehleinG.P.BodeyColorectal cancer in young adultsSouth Med J741981920924
- A.BehbehaniM.SakwaR.EhrlichmanP.MaguireS.FriedmanG.SteeleColorectal carcinoma in patients under age 40Ann Surg2021985610614
- J.B.O’ConnellM.A.MaggardE.H.LivingstonC.K.YoColorectal cancer in the youngAm J Surg1872004343348