
Abstract
Background
The global prevalence of female genital mutilation (FGM) ranges from 0.6% up to 98%. It has many health psychological impacts including abnormalities of female sexual function.
Objectives
To study female genital mutilation and its effect on female sexual function, Alexandria, Egypt 2013.
Methods
A case–control study was conducted on a convenient sample of 272 circumcised women with their 272 control from 4 randomly selected primary health care centers. Specially designed format (including data about socio-demographic characters, gynecological obstetric histories, and FGM act) and female sexual function index (a 19-item self-reported questionnaire for assessing the key dimensions of female sexual function) were used. Bivariate analysis was conducted to test significant differences between cases and control.
Results
73.9% of cases experienced dysmenorrhea (OR = 3.750), 43.4% had obstructed labor (OR = 1.745) and 27.6% got postpartum hemorrhage (OR = 2.855). 48.9% of FGM was performed by dayas or midwives, 91.2% performed at home, 49.6% of type I, and 87.9% experienced complications. Cases had lower mean sexual function. 52.6% of cases were convinced with FGM.
Conclusion
FGM was a risk factor for dysmenorrhea, obstructed labor and postpartum hemorrhage. Cases had lower mean sexual function; moreover, half of them convinced with FGM practice and with its continuation.
1 Introduction
World Health Organization (WHO) defined female genital mutilation (FGM) as “all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons.”Citation1 Many countries throughout the globe perform it: Western, Eastern, and North-Eastern Africa, particularly Egypt and Ethiopia, and in parts of Asia and the Middle East (nearly half of its cases are in Egypt and Ethiopia). The prevalence of FGM ranges from 0.6% up to 98%.Citation2 It was performed for about 140 million women and girls, 101 million in Africa alone.Citation1
The practice is deep-rooted in gender disparity, cultural uniqueness, and ideas about purity, modesty, esthetics, status and honor. Moreover, it acts as a trial to manage women’s sexual life by reducing their sexual desire, thus promoting chastity and fidelity. This practice is encouraged by both women and men.Citation3
It is performed at the age of four years up to puberty. It is usually performed at home without anesthesia.Citation5 It has four types.Citation4 Type I is usually the removal of the clitoris and clitoral hood.Citation1 Type II is the removal of the clitoris and labia minora.Citation5 Type III involves the removal of all or part of the labia minora and majora, and usually the clitoris, with wound suture; a small hole is left for the passage of urine and menstrual blood, and the wound is re-opened for intercourse and childbirth.Citation5 Types I, II, and III are performed for 85% of cases. Type III is the most common procedure in Djibouti, Somalia and Sudan, and in parts of Eritrea, Ethiopia and Mali.Citation6 Type IV is the miscellaneous procedures at the external genitalia, for example symbolic piercing of the clitoris or labia, cauterization of the clitoris, and cutting into the vagina to widen it.Citation5
FGM has many health effects including recurrent urinary and vaginal infections, chronic pain, infertility, hemorrhaging, epidermoid cysts, and difficult labor.Citation7 It has also its psychological impact and abnormalities in the female sexual function.Citation8
Throughout Egypt, many studies have been conducted to determine the pattern and prevalence of FGM, but those studied the risks of FGM and its effect on women’s sexual life are scare.Citation8–Citation13 Therefore, this study was carried out.
2 Objective
To study the effects of female genital mutilation on female sexual function, Alexandria, Egypt 2013.
2.1 Subjects and methods
A case–control study was conducted during the period June through August 2013. A convenient sample of 272 currently married educated women had FGM with their 272 matched controls (their matching was for age, education and marital status); women were included from 4 randomly selected PHCC: 2 from urban and 2 from rural Alexandria (Abees region).
Approval of the authority was assured. Ethical consideration and confidentiality of the data were assured. Written signed consent was obtained from every participant after explanation of the objectives of the study. The response rate was 80% (272/340).
A specially designed interviewing format in Arabic was completed by the researcher followed by completion of Female Sexual Function Index (FSFI) by the women herself. The interviewing format included data about socio-demographic characters, gynecological and obstetric histories, and FGM act. The format also included female sexual function index (FSFI).Citation8 FSFI is a 19-item questionnaire, and has been developed as a brief, multidimensional self-report instrument for assessing the key dimensions of sexual function in women. It included 6 domains namely: desire, arousal, lubrication, orgasm, satisfaction and pain.Citation8 Satisfaction was measured using related 3 FSFI questions which measured in 3 choices modified Likert scale graded from 0 to 2, where unsatisfaction = 0, indifference = 1, and satisfaction = 2. Satisfaction is considered as (Yes) when the total scores ⩾4 and is considered as (No) when the total score <4.
2.2 Statistical analysis
Data were entered and analyzed using SPSS version 17.0. Data were presented using frequencies, means and standard deviation. Bivariate analysis was conducted to test significant differences between cases and control. Chi-square test was used for qualitative variables and Student t-test for quantitative one. The level of significance was at 95% level.
3 Results
The mean age of the studied cases was 32.7 ± 7.44 years and their mean age of marriage was 20.4 ± 2.47, with no significant statistical differences between cases and control. () Nearly two-fifths (39.3%) of cases got university education and more, 43.4% was working (p = 0.006), 49.6% belonged to middle social class (p = 0.021), and 74.3% lived in nuclear family ().
Table 1 Socio-demographic description of the studied women.
For cases, the mean age of menarche was 11.7 ± 1.40 year, the mean number of gravidity, parity, abortions, and female daughters were 4.1 ± 1.85, 3.1 ± 1.30, 1.1 ± 1.11and 1.5 ± 0.97 respectively with insignificant difference between cases and control (data were not presented).
Regarding gynecological and obstetric history of cases, 42.3% had irregular menses, 73.9% experienced dysmenorrhea (OR = 3.750), 43.4% had obstructed labor (OR = 1.745) and 27.6% got postpartum hemorrhage (OR = 2.855) ().
Table 2 Gynecological and obstetric history of cases and their control.
On describing the FGM act, the mean age of that act was 9.7 ± 2.12 year, 48.9% of cases were performed by dayas or midwives, 91.2% performed at home, 49.6% of type I, 87.9% experienced complications and for 44.4% of cases, grandma was the person who insisted for doing this act ().
Table 3 Description of FGM practice.
Regarding the sexual functions, the cases had lower mean sexual function than control in all aspects namely sexual desire, sexual arousal, lubrication, orgasm, satisfaction, and pain, with total score of 14.3 ± 5.93 for cases and 25.9 ± 3.44 for control (p = 0.000) ().
Table 4 Sexual function among cases and control.
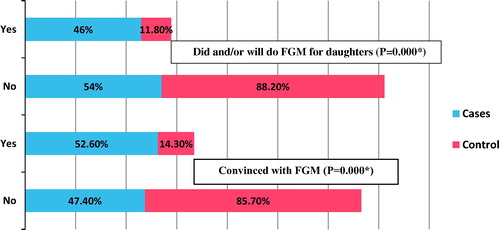
illustrates that 52.6% of cases were convinced with FGM (p = 0.000) and 46.0% of them actually did it or plan to do it for their daughters.
Figure 1 Attitude of women toward FGM practice.
4 Discussion
In Egypt, 91% of women aged 15–49 years have been circumcised despite banning of this practice by the government.Citation14
Rural women are more likely to be circumcised than urban one.Citation14 This was concomitant with the results of the present work, where 57.7% of cases were of rural origin.
Egyptian demographic health survey 2008 (EDHS) illustrated that the possibility of FGM also declined with educational level and was higher among women in lower social strata.Citation14 This was also proved by the current work (39.3% of cases got university education and more versus 43.3% of their control group and 44.9% with perceived low social class versus 33.8% of their control group).
EDHS 2008 stated that all circumcised women had this act before the age of 15 years. The tradition is that all girls are circumcised before puberty.Citation14,Citation15 The same was proved by this study, where the mean age of FGM was 9.7 ± 2.12 years. Nearly half (48.9%) of FGM was carried out by dayas or midwives, which was nearly similar to the results of EDHS 2008.Citation14
FGM has many frequent health impacts. They include infection (mainly urinary or vaginal), pain, infertility, hemorrhage and complications during childbirth.Citation7 That was concomitant with the results of the present work, where 87.9% of cases experienced complications. Cases were at risk of obstructed labor (OR = 1.745) and postpartum hemorrhage (OR = 2.855). Three-quarters of cases (74.6%) had assisted delivery (OR = 7.728).
Cases were at risk of dysmenorrheal (OR = 3.750). FGM may end in fibrosis which could predispose to dysmenorrheal.Citation16
The present work revealed a significant association between FGM and female sexual function, where reduction of all aspects was obtained (namely desire, arousal, lubrication, orgasm, satisfaction and pain). The total score of female sexual function for cases was significantly lower than their control (14.3 ± 5.93 for cases versus 25.9 ± 3.44 for control).
Women with FGM have more sexual adverse effects.Citation8,Citation12 One study that was conducted in Ismailia, EgyptCitation13, proved that women with FGM have higher rates of dyspareunia and lack of sexual desire. This could be explained by the fibrosis and rigid scar tissue following FGM which predisposes to narrowing of the vaginal orifice and muscular spasm which makes intercourse painful and difficult. These physical factors will predispose to psychological one, where the painful experience will drive women to lose both sexual desire and satisfaction.Citation16,Citation17
Despite all previously proved side effects of FGM, the present work revealed that 52.6% of cases convinced with this practice. Moreover, 46.0% actually re-did it or plan to do it for their daughters. EDHS 2008 stated that over the next 15 years in Egypt, there will be a steady decrease in the percent of women who will be circumcised from the level of 77% down to 45%.Citation8
5 Conclusion
FGM was a risk factor for dysmenorrhea, obstructed labor and postpartum hemorrhage. Cases had lower mean sexual function; moreover, half of them convinced with FGM practice and with its continuation.
Recommendation
Further researches are needed to study the full range of FGM effects on physical, mental and psychosocial life of women. Moreover, planned health education campaigns are mandatory to elude the drawbacks of FGM and hazards of continuation of this practice.
Conflict of interest
None.
Authors’ contribution
It is a single author paper. He carried out all the work from coordination of the work until drafting, revision of manuscript, statistical analysis, and design.
Financial support
None.
Acknowledgments
The author would like to thank all the nurses of primary health care centers who cooperate in communication with women and help in data collection. Special thanks for all women who participate in this study.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 22 April 2015
References
- World Health OrganizationFemale Genital MutilationFebruary 2013World Health OrganizationGeneva
- ARahmanN.ToubiaFemale Genital Mutilation: A Guide to Laws and Policies Worldwide2000Zed Books
- G.MackieEnding footbinding and infibulation: a convention accountAm. Sociol. Rev.61619969991017
- World Health OrganizationEliminating Female Genital Mutilation2008World Health OrganizationGeneva pp. 4, 22–8
- World Health OrganizationEliminating Female Genital Mutilation2008World Health OrganizationGeneva
- J.C.CaldwellI.O.OrubuloyeP.CaldwellFemale genital mutilation: conditions of declinePopul. Res. Policy Rev.1932000233254
- J.AbdulcadiraC.MargairazM.BoulvainO.IrionEffectiveness of interventions designed to prevent female genital mutilation/cutting: a systematic reviewSwiss Med. Weekly6142011
- R.RosenThe female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual functionJ. Sex Marital Ther.2622000191208
- M.A.Tag-EldinM.A.GadallahM.N.Al-TayebM.Abdel-AtyE.MansourPrevalence of female genital cutting among Egyptian girlsBull. World Health Org.862008269274
- T.K.Al-HussainiFemale genital cutting: types, motives and perineal damage in laboring Egyptian womenMed. Princ. Pract.122003123128
- M.F.AllamJ.de Irala-EstevezR.Fernandez-Crehuet-NavajasA.Serrano de CastilloJ.S.HoashiFactors associated with the condoning of female genital mutilation among university studentsPublic Health1152001350355
- A.ElnasharR.AbdelhadyThe impact of female genital cutting on health of newly married womenInt. J. Gynaecol. Obstet.972007238244
- M.H.El-DefrawiG.LotfyF.DandshH.RefaatM.EyadaFemale genital mutilation and its psychosexual impactJ. Sex Marital Ther.272001465473
- El-Zanaty F, Way AA. Egypt demographic and health survey 2008. Calverton, Maryland, USA: Ministry of Health and Population [Arab Republic of Egypt], National Population Council [Arab Republic of Egypt], and ORC Macro; 2009
- O.El-GibalyB.IbrahimB.S.MenschW.H.ClarkThe decline of female circumcision in Egypt: evidence and interpretationSoc. Sci. Med.542002205220
- World Health Organization. A systematic review of the health complications of female genital mutilation including sequelae in childbirth. WHO/FCH/WMH/00.2. Geneva; 2000
- Geletkanycz C. The practice of female circumcision. Report from Institution; U.S. Public Health Services. Dataset-reports. Washington: Office of International Health; 1993. p. 5–45.