
Abstract
Background
Hyoid bone chondrosarcoma is a very rare condition. This study presents a case report of low-grade chondrosarcoma of hyoid bone with cervical nodal metastasis. The study also presents preoperative radiological investigations, pathological examination and the follow-up of the case.
Case presentation
A 42 years old female had a hard mass in the left submandibular region of the neck. The mass was 5.5 cm × 7.5 cm and mobile with deglutition.
Conclusions
Although the tumor was low grade, it showed cervical lymph node metastasis months after its surgical excision. This shows the importance of scheduled CT scan of the neck during follow-up of these cases.
1 Introduction
Chondrosarcoma is one of the most common types of primary bone tumors in adults, second only to osteosarcoma.Citation1 It constitutes around 11% of all bone tumors. It mostly arises in the pelvic bones, proximal femur, proximal humerus, distal femur, and the ribs.Citation2 A small percent of the cases of chondrosarcoma arise in the head and neck region (1–12% of cases), where it usually involves the nose and paranasal sinuses, mandible, temporal bone, and larynx.Citation3
Chondrosarcoma rarely involves the hyoid bone with only 20 cases reported in the literature.
This is a description of a case of hyoid chondrosarcoma treated in our institute, and a review of the literature.
2 Case report
42 years female patient presented with painless left sided submandibular neck mass for 1 year.
On examination the mass is about 5.5 cm × 7.5 cm hard, not fixed to the surrounding structures, mobile with deglutition non-tender and without any inflammatory signs.
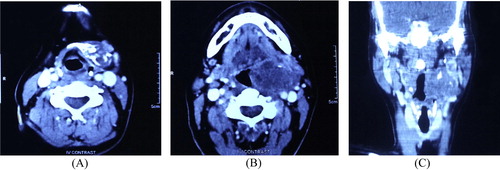
Contrast enhanced CT scan was done and demonstrated that the mass is based on the region of the left greater and lesser cornua of hyoid bone (). Associated destructive changes were noted in the hyoid bone. The matrix showed osseous density ossification foci. The mass was encroaching upon the oropharyngeal, left pyriform fossa, and supraglottic larynx and laterally reaching the submandibular and carotid space.
Figure 1 Preoperative CT scan of the patient contrast enhanced CT scan axial view of the neck showing the chondrosarcoma of the hyoid bone on the left side with heterogeneous consistency and peripheral calcification (A), (B) axial view and (C) coronal view.
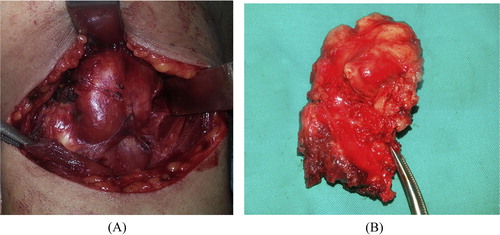
It was resected with the whole body of the hyoid bone as a safety margin, measuring 8 × 6 × 4 cm in dimensions ().
Figure 2 Operative demonstration of the tumor (A) showing the mass attached to the left side of hyoid bone deep to the sternomastoid muscle and (B) the surgical specimen.
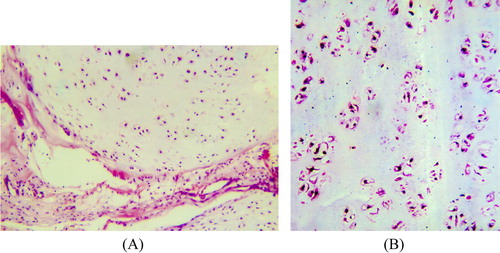
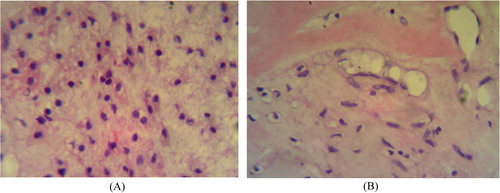
Histopathological examination of the mass revealed lobules of atypical cartilaginous tissue (). The cartilaginous matrix included numerous chondrocytes in their lacunae, having slight hyperchromatic nuclei, with focal areas of myxoid changes. Fibrous stromal tissue was intersecting the growth with few scattered bony spicules.
Figure 3 Histopathological examination of the tumor (A) part of a nodule of malignant cartilaginous growth made up of crowded hyperchromatic chondrocytes lying on a chondroid matrix. H&E 200×. (B) Closer view of the hyperchromatic multiple chondrocytes residing in their lacunae and lying on a basophilic chondroid matrix. H&E 300×.
The patient developed, 5 months later, left upper deep cervical nodal enlargement level II and III. Selective neck dissection of these levels was done. Histopathological examination of these lymph nodes revealed reactive lymphoid hyperplasia with no tumor tissue.
Surprisingly, follow-up enhanced CT scan after 3 months showed ring enhancing lymph node in the left parapharyngeal space (). Transoral excision was done. Pathological examination revealed metastatic deposits of low-grade chondrosarcoma in the lymph node, with large areas of hyaline material incorporating numerous islands of chondroid tissue formed of trabeculae and nests of cartilaginous cells exhibiting nuclear pleomorphism and mild hyperchromatism embedded in chondroid matrix ().
Figure 4 Postoperative imaging contrast enhanced CT scan axial view showing left parapharyngeal metastatic lymph node (white arrow).
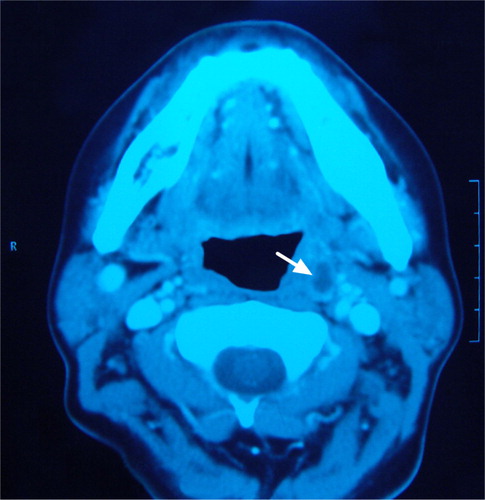
Figure 5 Histopathology of metastatic lymph node (A) showing deposits of chondroid tissue with chondrocytes showing nuclear pleomorphism and mild hyperchromatesia in chondroid matrix H&E 300× (B) with higher magnification H&E 400×.
3 Discussion
Hyoid chondrosarcoma is an infrequent condition with 20 cases reported in the literature till now. The diagnosis of chondrosarcoma is usually suspected after radiological investigations. Yet, it is not possible to differentiate chondroma from low-grade chondrosarcoma based on radiological criteria only.Citation4 The diagnosis is confirmed histopathologically after surgical excision. Other tumors of the hyoid bone include osteoma, chondroma, osteosarcoma, plasmacytoma, giant cell tumor, aneurysmal bone cysts. Chondrosarcoma may arise from any part of the hyoid bone.Citation4,Citation5
Hyoid chondrosarcoma usually presents with painless mass and sometimes dysphagia. It is more common in males. The age of presentation ranges from 28 to 82 years. Most of the cases reported were grade 1.Citation6
Unlike the present case, which showed lymph node metastasis after 8 months, previous studies did not show nodal metastasis in cases of hyoid chondrosarcoma (although some cases showed distant metastasis to the lung in most of the cases).Citation7 In Lee et al. study, there was a case of tonsillar recurrence in a case of thyroid cartilage chondrosarcoma.Citation8
Generally speaking, chondrosarcoma shows distant metastasis in 6.7% of cases.Citation8 Ozaki et al. studied intermediate and high-grade chondrosarcoma and found that the incidence on distant metastasis was 21% and 60% respectively.Citation9 There are 2 published case reports of humeral chondrosarcoma with nodal metastasis in the literature.Citation10,Citation11 In another report, among 46 cases of chondrosarcoma only 1 case showed lymph node metastasis.Citation12 It worth mentioning that, chondrosarcoma shows a relatively higher rate of local recurrence.Citation8
Contrast enhanced CT scan is the radiological investigation of choice for assessment of the nature and extension of the tumor. In most of the cases it shows bone destruction, and intrinsic calcification.Citation4 Other lesions that may show similar CT scan features include enchondroma and osteoblastoma, but they are very rare in the head and neck.Citation13
MRI gives a better idea regarding the surrounding soft tissue involvement. Chondrosarcoma appears heterogeneously hypointense in T1 weighted images, with strong peripheral enhancement. On T2 weighted image the lesion shows hyperintensity, with areas of signal voids due to intrinsic calcifications.Citation5 Other lesions that may show similar MRI characteristics include osteogenic tumor and aneurismal bone cysts. PET scan does not have a role in the diagnosis of chondrosarcoma as it cannot differentiate between chondroma and low-grade chondrosarcoma, but it may predict the grade of the tumor before surgery.Citation14
Pathologically chondrosarcoma is graded 1–3 based on the mitotic rate, cellularity, and nuclear size.Citation15 ()
Table 1 Histopathological grades of chondrosarcoma.
The treatment of choice in this condition is surgical resection. During surgery it is very important to ensure safe margins, because leaving residual disease is a well known cause of recurrence. Elective neck dissection is not indicated because of low incidence of cervical lymph node metastasis.
Postoperative complications may include dysphagia or dysphonia, but these sequelae did not happen in our case, and she returned back to her normal lifestyle after recovery from surgery. Postoperative radiation does not have a specific role in the treatment plan till now. It may be indicated if the patient is unfit for surgery.
The prognosis of this condition depends on the adequacy of surgical resection, and the histological grading of the tumor. Throughout the body 5 years survival rates are 90%, 81%, and 29% for grade 1, 2, and 3 respectively.Citation15 The rates of distant metastasis from chondrosarcoma are 0%, 21%, and 60% for grade 1, 2, and 3 respectively. Distant metastasis from chondrosarcoma frequently affects the lung.Citation9
The current NCCN guidelines for the follow-up of these patients are that, for the low-grade tumors CT of the chest and primary site should be done every 6–12 months for 2 years, then every year as appropriate. For the high-grade tumors CT chest should be done every 3–6 months for 5 years, and regarding the primary site CT should be done as clinically indicated.
4 Conclusion
The present study adds the 21st chondrosarcoma of the hyoid bone with an exceptional course. Although it was a low grade, the patient developed a positive parapharyngeal node, an unusual site after and usual period of time. The present case dictates obeying the NCCN guideline literally (regular CT scan neck every 6 months at least).
Conflict of Interest
Author states that there is no conflict of interest.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- B.B.KochL.H.KarnellH.T.HoffmanL.W.ApostolakisR.A.RobinsonW.ZhenNational cancer database report on chondrosarcoma of the head and neckHead Neck2242000408425
- D.S.SpringfieldM.C.GebhardtM.H.McGuireChondrosarcoma: a reviewInstr Course Lect451996417424
- B.B.BurkeyH.T.HoffmanS.R.BakerA.F.ThorntonK.D.McClatcheyChondrosarcoma of the head and neckLaryngoscope10012199013011305
- A.DemeyereF.De SomerD.PerdieusL.Van Den HauweL.LemmensJ.SchillebeeckxChondrosarcoma of the hyoid boneEur Radiol1022000308309
- K.ItohT.NoboriK.FukudaS.FurutaM.OhyamaChondrosarcoma of the hyoid boneJ Laryngol Otol10771993642646
- R.ThomeD.C.ThomeR.A.de la CortinaLong-term follow-up of cartilaginous tumors of the larynxOtolaryngol Head Neck Surg12462001634640
- I.ZhangN.G.ZaorskyJ.A.AbrahamM.TulucJ.M.CurryV.Bar-AdChondrosarcoma of the hyoid bone: case report and review of current management optionsHead Neck3672014E65E72
- S.Y.LeeY.C.LimM.H.SongJ.Y.SeokW.S.LeeE.C.ChoiChondrosarcoma of the head and neckYonsei Med J4622005228232
- T.OzakiA.HillmannN.LinderS.BlasiusW.WinkelmannMetastasis of chondrosarcomaJ Cancer Res Clin Oncol122101996629632
- A.GuliaA.PuriS.JainS.DhandaS.GujralChondrosarcoma of the bone with nodal metastasis: the first case report with review of literatureIndian J Med Sci6582011360364
- K.MatsumotoS.HukudaM.IshizawaY.SaruhashiH.OkabeY.AsanoParosteal (juxtacortical) chondrosarcoma of the humerus associated with regional lymph node metastasis. A case reportClin Orthopaed Relat Res2901993168173
- Y.FongD.G.CoitJ.M.WoodruffM.F.BrennanLymph node metastasis from soft tissue sarcoma in adults. Analysis of data from a prospective database of 1772 sarcoma patientsAnn Surg217119937277
- E.KaramanY.AlimogluF.OzGiant chondroma of the head and neck causing gross facial deformityEar Nose Throat J9122012E1E3
- H.TachinoH.FushikiM.IshidaY.WatanabeA low-grade chondrosarcoma presenting as an unusual cervical mass in the hyoid bone: a case reportJ Med Case Rep6201221
- H.L.EvansA.G.AyalaM.M.RomsdahlPrognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic gradingCancer4021977818831