
Abstract
Background
The WHO has recognized a variant of pituitary adenomas with potential aggressive behaviour which have been termed atypical pituitary adenomas. This group of tumours are recognized by their mitotic rate of more than >3%, p53 expression and invasion of surrounding structures. There has however been no study of the occurrence of these tumours in a black African population. This study is a preliminary attempt to examine this group of tumours in blacks.
Methods
This study retrospectively reviewed fifty-seven histologically diagnosed and immunohistochemically characterized pituitary adenomas received in our department over a twenty-one year period. Specimens were stained with ki67, a nuclear marker of cell proliferation which has been identified as the single best predictor of atypical pituitary adenoma.
Results
Twelve of the tumours showed atypical features with eight (67%) of these tumours being prolactinomas. Two of the tumours were gonadotrophs and two were null cell adenomas. There was no correlation with age or gender. Two of the tumours required neurosurgical re-exploration with one of these showing a higher mitotic index in the second biopsy.
Conclusion
The study suggests similarity in the rate of occurrence of pituitary adenomas with atypical features in a black African population with what is seen in Caucasians. Prolactinomas constitute a significant percentage of the tumours with this feature.
1 Introduction
The most common tumour occurring in the sellar area is the pituitary adenoma and it constitutes about 10–15% of all intracranial tumours.Citation1–Citation3 Pituitary adenomas are benign epithelial tumours composed of adenohypophyseal cells, some of which secrete hormonal substances.Citation3,Citation4 Most of the tumours are slow growing with the cells appearing monomorphic. They often grow in an expansive pattern and do not invade surrounding structures. Occasional tumours show invasion of surrounding structures with increase in proliferation.Citation4 The WHO classification of 2004 has identified this group of tumours as atypical adenomas and they are characterized by local invasion and increased mitosis.Citation5,Citation6 The atypical adenomas usually show an increased MIB-1 labelling index of more than 3% and often show p53 reactivity which is not seen in benign tumours.Citation2,Citation5 This group of tumours are known to confer a poor prognosis due to their high recurrence rate.Citation7 There is no proof at present to describe these tumours as premalignant lesions despite their clinical behaviour. However, the clinical relevance of these tumours has been questioned based on studies which have not been able to show any correlation with invasiveness and rate of proliferation.Citation7–Citation9 Several studies have shown that the ki67 index is the single best predictor of atypia in pituitary adenoma compared with the other parameters.Citation10,Citation11
Many studies have shown prolactinomas, and corticotroph adenomas as the most common tumours showing atypical features, while null cell and gonadotroph adenomas as the least common; others have shown lack of uniformity in the secretory status of cells showing invasion.Citation2,Citation12,Citation5,Citation13 No study has been carried out in an African population to determine the occurrence of this variant of pituitary adenomas in the black African population. This is a preliminary study examining the occurrence of pituitary adenomas with atypical features in a predominantly black African population.
2 Materials and method
This study was conducted on immunohistochemically characterized pituitary adenomas from surgical specimens obtained at the University College Hospital, Ibadan over a twenty-one year period. The tumours were removed via Pterional craniotomy with microsurgical total tumour removal for the giant tumours and endoscopic trans-septal trans-sphenoidal pituitary resection for the intrasellar tumours. The pituitary adenomas had been identified according to the earlier described method.Citation14 Ethical approval for the study was obtained from the joint University of Ibadan/University College Hospital ethical committee. The age, sex and clinical history of the patients were obtained from their records. There was no record of accompanying dura in the gross description of any of the biopsies. The archived slides and paraffin wax blocks were retrieved and the slides were reviewed to ascertain the accuracy of the initial diagnoses.
Each of the tissue blocks was stained with antibodies for ki67. The streptavidin-biotin-peroxidase method was used and the protocol followed that of previous researchers.Citation12,Citation13,Citation15
Three serial sections, cut at 5 μm each, were obtained from the archived paraffin blocks for each case and deparaffinised. Antigen unmasking, using the heat induced epitope retrieval method, was done by first pre heating the retrieval buffer to a temp of 90–95 °C in an incubator (microwave) and subsequently immersing the slides in preheated citrate buffer diluted to 1:10 with distilled water for 10–20 min. They were then allowed to cool for 20 min in cold water and thereafter rinsed in TBST (Tris buffered saline with Tween). Blocking of enzyme activities/peroxidase was done with 3% hydrogen peroxide for 10–15 min. Each specimen was incubated for 20–30 min with 40–130 μl of an appropriately characterized and diluted (1:200) KI67 rabbit primary antibody (Thermofisher scientific Clone SP6). This was followed by incubation with an undiluted labelled polymer Horse Radish Peroxidase (HRP) conjugated anti-mouse secondary antibody for 30 min. Diaminobenzidene [DAB] solution was added to cover the specimen. Counterstaining was done with Haematoxylin. A tonsil biopsy with a histological diagnosis of reactive follicular hyperplasia and a normal pituitary gland were used as positive and negative controls respectively.
The proliferation index was assessed using a modification of the earlier described methods.Citation8,Citation9 A total of 1000 nuclei from the neoplastic cells were counted from ten randomly selected fields with the aid of a graticle. This was done on each slide at 40× magnification. The total number of stained nuclei was expressed as a percentage of the absolute number of counted nuclei. Using modified 2004 World Health Organisation criteria, adenomas with a Ki67 index of ⩾3% were classified as atypical adenomas.Citation6 Statistical analysis was performed using Student t-test for comparison of continuous variables and chi-squared test for comparison of discontinuous variables, to determine whether there was any association between the clinical and immunohistochemical data. The level of statistical significance was set at p ⩽ 0.05.
3 Result
A total of 134 patients were diagnosed with pituitary adenoma from the institutional cancer registry record during the study period. However only seventy-two of the biopsies were received in the surgical department during the study period (many of the patients received drug therapy while some defaulted and were lost to follow up). Fifty-seven of the surgical biopsies of pituitary adenomas were included in the study. Fifteen of the biopsies were excluded either due to unavailability of their tissue blocks while some had been exhausted during earlier diagnostic procedures. The specimens were obtained from patients with ages ranging from 9 to 73 yrs. The tumours occurred more frequently in patients in their fifth decade with 17 (30%) pituitary adenomas seen in this age group ().
Table 1 Distribution of benign and atypical adenoma according to age in decades.
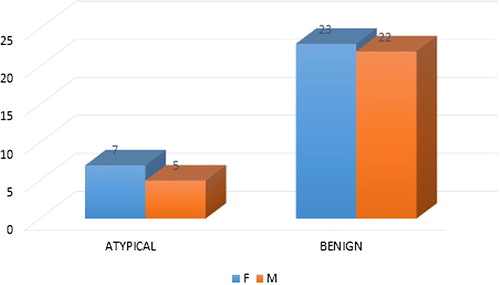
The ki67 index in the tumours ranged from 0.2 to 10.2 with a mean index of 2.05. The benign tumours were 45 (79%) while the pituitary adenomas with atypia constituted 12 (21%). Eight of the pituitary adenomas with atypia (67%) occurred in patients in the fourth and fifth decades. There was however no statistical significance between the age and the level of atypia in these tumours (p = 0.456). Thirty (52.6%) of the tumours were from female patients while 27 (47.4%) were obtained from male patients. Seven of the pituitary adenomas with atypical features occurred in females while five occurred in males (). There was no statistical significance between the sex and tumour atypia (p = 0.751).
Figure 1 Sex distribution of the patients with pituitary adenoma variants in the study.
Eight (67%) of the pituitary adenomas with atypia showed positive staining for prolactin. This was significant (p = 0.001). Only two gonadotroph and null cell adenomas had atypical features, even though they are the most frequent adenomas seen (). Twenty-two (38.6%) of the pituitary adenomas showed microscopic dural invasion while only three (13.6%) of these invasive tumours showed high ki67 index.
Table 2 Hormone expression of pituitary adenomas in the study.
Four out of the fifty-seven pituitary adenomas had surgical re-exploration with two of these tumours having features of atypia. Only one of the recurrent adenoma with atypical features was a prolactinoma while the other was a null cell adenoma. The lone case of prolactinoma required re-exploration after the pathologist identified the tumour as atypical and the second biopsy from the re-exploration showed a markedly higher index score ().
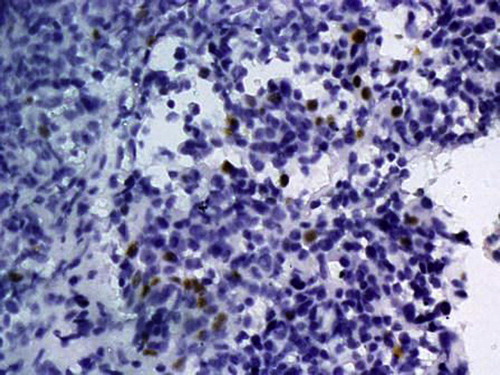
Figure 2 Ki67 expression in an atypical adenoma with nuclear staining of proliferating cells in the cell cycle. 400× magnification.
4 Discussion
Invasive pituitary adenomas do not show typical histological features of malignancy that identify tumours in other organs.Citation18 The exact pathway that determines progression in pituitary adenomas is yet to be fully understood although the Ras gene mutation has been identified in some cases of pituitary carcinoma.Citation4,Citation19 Ikeda and Yoshimoto have also demonstrated that adenomas with increased ki67 index tend to show increased expression of both c-myc and bcl-2 genes.Citation20 Protein kinase C (PKC) and Pituitary Tumour Transforming Gene (PTTG-1) are among the few other identified gene mutations associated with increased aggressiveness.Citation1,Citation4,Citation21 Several growth factors have however been associated with increased ki67 index including epithelial growth factor receptor (EGFR) and isoforms of basic fibroblast growth factor receptor (FGFR4).Citation4,Citation19,Citation21
The 2004 WHO definition of atypical adenomas identified several characteristics which include high mitotic rate, ki67 index greater than 3%, increased expression of p53 gene or gross invasion of neighbouring structures.Citation6,Citation21 The proliferation index can be measured using several different immunohistochemical markers but many studies have shown the greater utility of ki67, a nuclear marker that is active at all the stages of cell division.Citation15,Citation22–Citation24 Our study used ki67 proliferation rate alone which has been shown in some studies as the best single predictor of atypical behaviour in pituitary adenoma.Citation10,Citation11
Eight of the twelve adenomas with atypical features identified in this study were prolactinomas which is in keeping with earlier studies which noted that prolactinomas and ACTH adenomas tend to have higher MIB index compared to the other tumour types while null cell and gonadotroph adenomas often show low values.Citation1,Citation4,Citation7 Other studies, however do not agree with this finding and have shown that the rate of atypical features seen in different adenoma groups vary, although some tumour types such as the silent corticotroph adenomas are more likely to show atypia.Citation17,Citation22
Although none of the specimen seen in our study had evidence of gross dural invasion, some of the tumours showed microscopic dural invasion. The percentage of the tumours seen in this study with this feature (38.6%) is much lower than the 85% observed in the study by Scheithauer et al. for dural invasion of all pituitary adenoma tumour types.Citation18 Their study also noted that the incidence of dural invasion is often under reported due to the fragmented nature of the specimen usually received, which emphasizes the importance of very careful observation by the pathologists for detection of microscopic dural invasion.Citation18 Another possibility may be the absence of dura in the biopsy specimen received by the pathologist. This may have also contributed to the low number of tumours with microscopic dural invasion identified in this study. It is noteworthy however, that the 2004 WHO classification does not consider microscopic dural invasion a criterion for designation of atypia.Citation6 Neuroradiological and surgical observation, with the operating microscope, of gross dural invasion is however considered a feature of invasiveness.Citation6,Citation16
Several workers have shown a lack of correlation between MIB labelling index in pituitary adenomas and the incidence of tumour recurrence, after surgical removal.Citation8,Citation9,Citation12,Citation13 The lack of consistency in the behaviour of the tumours has made many clinicians to re-consider the usefulness of the MIB index in pituitary adenomas to patient management.Citation7 In our series the prolactinoma with atypical features which required re-exploration was detected via its high proliferation index. The increase in the proliferation rate of the second biopsy showed a potentially aggressive tumour; a point in favour of the prognostic value of the MIB index.
4.1 Limitations
The number of samples in this study is small and epidemiological conclusions could not be made based on our results. The study however serves as a preliminary study on the occurrence of pituitary adenomas with atypical features in blacks. The study was conducted in a national center catering to patients from distant parts of the country who are often lost to follow up after discharge due to distance. A true description of the rate of recurrence of this group of tumours cannot be proffered in this study.
4.2 Conclusion
The behaviour of pituitary adenomas is yet to be fully understood. However, it appears that the occurrence of pituitary adenoma with atypical features in a predominantly black population, as shown in this study, is similar to what is seen in Caucasian populations. However, due to the low number of samples in this study, an epidemiological conclusion cannot be made. There is a need for a larger study with a view to deriving more definitive epidemiological data and characterizing the genetics of pituitary adenomas in this patient population represented by our study subjects.
supplementary Material 1
Download MS Excel (22 KB)Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 31 December 2016
Related Research Data
References
- N.Y.Y.Al-BrahimS.L.AsaMy approach to pathology of the pituitary glandJ Clin Pathol5920061245125310.1136/jcp.2005.031187
- S.EzzatS.L.AsaMechanisms of disease: the pathogenesis of pituitary tumorsNat Clin Pract Endocrinol Metab2200622023010.1038/ncpendmet0159
- J.W.IronsidePituitary gland pathologyJ Clin Pathol1722003561568
- S.L.AsaS.EzzatThe cytogenesis and pathogenesis of pituitary adenomasEndocr Rev19199879882710.1210/edrv.19.6.0350
- K.KovacsThe 2004 WHO classification of pituitary tumors: commentsActa Neuropathol1112006626310.1007/s00401-005-1095-4
- R.V.LloydK.KovacsW.F.YoungJrPituitary tumoursR.V.LloydR.A.DellelisP.U.HeitzC.EngPathology and Genetics of Tumours of Endocrine Glands2004IARC PressNew York945
- B.K.Kleinschmidt-DeMastersPituitary GlandR.JuanRosai and Ackerman’s Surgical Pathology10th ed.2011ElsevierEdinburgh24412459
- A.FuscoM.C.ZatelliA.BianchiPrognostic significance of the Ki-67 labeling index in growth hormone-secreting pituitary adenomasJ Clin Endocrinol Metab9320082746275010.1210/jc.2008-0126
- Syro LV, Rotondo F, Ramirez A, Ieva A Di, Sav MA. Progress in the diagnosis and classification of pituitary adenomas. 2015;6(June):1–8.
- C.P.MiermeisterS.PetersennM.BuchfelderHistological criteria for atypical pituitary adenomas – data from the German pituitary adenoma registry suggests modificationsActa Neuropathol Commun [Internet]. Acta Neuropathologica Communications201511110.1186/s40478-015-0229- [Available from]
- M.LosaR.L.BarzaghiP.MortiniDetermination of the proliferation and apoptotic index in adrenocorticotropin-secreting pituitary tumors: comparison between micro- and macroadenomasAm J Pathol156200024525110.1016/S0002-9440(10)64725-6
- B.W.ScheithauerE.HorvathR.V.LloydK.KovacsPathology of pituitary adenomas and pituitary hyperplasiaK.ThaparK.KovacsB.W.L.R.ScheithauerDiagnosis and Management of Pituitary Tumors2001Humana pressNew Jersey91154
- D.R.HintonS.L.AsaPituitaryR.J.CoteN.WeidnerS.W.L.SusterModern Surgical Pathology2009Saunders ElsevierPhiladelphia19491979
- A.SalamiA.MalomoT.ShokunbiE.AkangImmunohistochemical analysis of pituitary adenomas in a West African hospitalAJNS3220137280
- F.SalehiK.KovacsB.W.ScheithauerImmunohistochemical expression of pituitary tumor transforming gene (PTTG) in pituitary adenomas: a correlative study of tumor subtypesInt J Surg Pathol18201051310.1177/1066896909356105
- D.B.DeStephanoV.Lloyd RA.M.PikeB.S.WilsonPituitary adenomas. An immunohistochemical study of hormone production and chromogranin localizationAm J Pathol1161984464472http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve%26db=PubMed%26dopt=Citation%26list_uids=6089568
- A.C.RishiM.SharmaC.SarkarA clinicopathological and immunohistochemical study of clinically non-functioning pituitary adenomas: a single institutional experienceNeurol India582010418423
- B.W.ScheithauerK.T.KovacsE.R.J.LawsR.V.RandallPathology of invasive pituitary tumors with special reference to functional classificationJ Neurosurg65198673374410.3171/jns.1986.65.6.0733
- A.LaniaG.MantovaniA.SpadaGenetics of pituitary tumors: focus on G-protein mutationsExp Biol Med Maywood NJ228200310041017http://www.ncbi.nlm.nih.gov/pubmed/14530508
- Ikeda H, Yoshimoto T. Tumor growth and biological markers in pituitary adenomas. 1998;(June 1996):167–173.
- O.MeteS.EzzatS.L.AsaBiomarkers of aggressive pituitary adenomasJ Mol Endocrinol492012R69R7810.1530/JME-12-0113
- C.Y.HsuW.Y.GuoC.P.ChienD.M.T.HoMIB-1 labeling index correlated with magnetic resonance imaging detected tumor volume doubling time in pituitary adenomaEur J Endocrinol16220101027103310.1530/EJE-09-1100
- L.MastronardiA.GuiducciF.PuzzilliLack of correlation between Ki-67 labelling index and tumor size of anterior pituitary adenomasBMC Cancer120011210.1186/1471-2407-1-12
- L.MastronardiA.GuiducciC.SperaF.PuzzilliF.LiberatiG.MairaKi-67 labelling index and invasiveness among anterior pituitary adenomas: analysis of 103 cases using the MIB-1 monoclonal antibodyJ Clin Pathol52199910711110.1136/jcp.52.2.107
Appendix A
Supplementary material
Supplementary data associated with this article can be found, in the online version, at http://doi:10.1016/j.ajme.2016.11.003.