
Abstract
Introduction
Various treatment techniques as breath hold techniques have been developed to spare the heart and lung in breast cancer patients receiving adjuvant radiotherapy.
Purpose
to compare the heart and lung dosimetric parameters of semi lateral decubitus technique with and without deep inspiration breath hold with standard supine techniques for left-sided breast cancer patients undergoing breast conservative surgery and adjuvant radiotherapy.
Methods
Fifty patients with left-sided breast cancer were simulated using standard supine, semi lateral decubitus and semi lateral decubitus and deep inspiration breath hold. The three plans carried out using two tangential opposed photon beams were compared.
Results
There was a significant reduction in heart V5Gy, V10Gy, V25Gy, V30Gy, mean dose & max dose with semi-lateral decubitus and breath hold technique compared to supine technique & semi-lateral decubitus technique (P < 0.001). There was also a significant reduction in the above mentioned heart DVPs with semi-lateral decubitus (P < 0.001) compared to supine technique.
There was a significant reduction in ipsilateral lung V20Gy and mean dose with semi-lateral decubitus and breath hold technique compared to supine technique (P < 0.001) & semi-lateral decubitus technique (P = 0.003 & 0.006) respectively. There was also a significant reduction in ipsilateral lung V20Gy and mean dose with semi-lateral decubitus (P < 0.001 & 0.007) compared to supine technique.
Conclusion
Semi-lateral decubitus techniques with and without breath hold for left sided breast cancer patients significantly reduce the dosimetric parameters of the heart and ipsilateral lung compared to supine technique with comparable target dose coverage.
Abbreviations:
- CTV
- clinical target volume
- PTV
- planning target volume
- RTOG
- Anatomical Boundaries of Breast Cancer Atlas for Radiation Therapy Planning of radiation therapy oncology group
- 3DCRT
- Three Dimensional Conformal Radiotherapy
- OARs
- organs at risk
- DVPs
- dose volume histogram parameters
- CT
- computed tomography
- MLCs
- multi-leave collimators
- DVH
- dose volume histograms
- HI
- homogeneity index
- DIBH
- deep inspiration breath hold
- FR
- free breath
- RT
- radiotherapy
- RSD
- Reverse semi Lateral Decubitus
- ILD
- Isocentric Lateral Decubitus
- IMRT
- Intensity Modulated Radiotherapy
- ICRU
- International commission on Radiological Units and Measurements
1 Introduction
Radiotherapy to the intact breast is considered a major part of breast cancer conservation management to prevent recurrences. But it has been shown that radiation increases the risk of heart and lung diseases so increases their mortality. This is more common in the left sided breast cancer patients.Citation1,Citation2
Various simulation and treatment techniques have been developed in order to reduce the volume of the heart and lung received high dose in breast cancer patients underwent adjuvant radiotherapy specially when treating the left side.Citation3,Citation4 These techniques include free breath hold, respiratory gating and voluntary deep inspiration. Simulation and treating the patients in prone,Citation5,Citation6 lateral and semi-decubitus positions could also improve cardiac and lung dosimetry.Citation7,Citation8 Another ways of cardiac sparing are intensity modulated radiotherapy (IMRT) and proton beam radiotherapy.Citation9
Breath hold reduces the heart dose because the heart volume exposed to radiation is reduced as the heart moves away from the chest wall. Respiratory gating is an alternative technique for cardiac sparing as the distance between the heart and the radiation fields is enlarged during respiratory expansion of the thorax.Citation5,Citation6
In prone positioning technique the breast moves away from the chest wall so the radiation beam edge is positioned away from the heart. However the benefit of the prone technique in cardiac protection is limited to the patients with large breast.Citation10,Citation11
Treatment of the patient in lateral decubitus position appears to be associated with a limited risk of heart and lung complications as the irradiation of the heart and lungs is extremely low.Citation8
The semi-decubitus (RSD) technique is an alternative method for cardiac and lung sparing for patients who are unable to tolerate breath hold.Citation7
Computerized leaves of IMRT allow for radiation field shaping and help dose escalation to the target with significant reductions in the cardiac dose. IMRT is successfully used as a class solution for cardiac protection in left sided breast cases especially for patients with large breast.Citation12–Citation15 Proton beam radiotherapy allows rapid dose fall off beyond the Bragg peak. This reduces cardiac toxicities as it causes dose reduction to the organs beyond the target volume such as the heart.Citation16
Purpose: to compare the heart and lung dosimetric parameters of semi lateral decubitus technique with and without deep inspiration breath hold with standard supine techniques for left-sided breast cancer patients undergoing breast conservative surgery and adjuvant radiotherapy.
2 Materials and methods
2.1 Patient selection and simulation technique
Fifty patients with early stage left sided breast cancer who referred to Alexandria university main hospital and Alexandria Ayadi Al Mostakbal Oncology Center to undergo breast conservative surgery and adjuvant radiotherapy from October 2015 to April 2016 were enrolled in this study.
The patients were scanned on CT simulator in three positions with 5 mm slices from the level of the larynx to the level of the upper abdomen including both lungs.
In the first scan; patients underwent CT simulation in supine position on ordinary breast board. The ipsilateral arm was abducted above the head (A). In the second scan; patients were immobilized using a special breast board with lateral angle enabled the left side elevation by 20 cm from the couch on reveres semi decubitus. The ipsilateral arm was abducted above the head. Both CT simulation scans were performed free breathing (B).
Figure 1 Standard breast board (A) & special breast board (B).
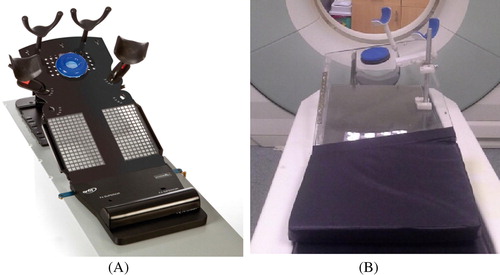
The special board allows reproducible arm positioning and semi lateral adjustment as the breast board provides arm supports above the head to give unimpeded access to the treatment area. It also has lateral angle in order to achieve semilateral decubitus with the breast elevated up in a consistent comfortable position (B).
In the third scan; patient position was the same as in the second scan with deep inspiration breath hold for 20 s. There was a training session before the simulation for each patient to ensure that the patient is able to hold his breath for 20 s. During this session the patient was trained to hold his breath gradually for 5 s, 10 s, 15 s then 20 s.
2.2 Target definition and organs at risk
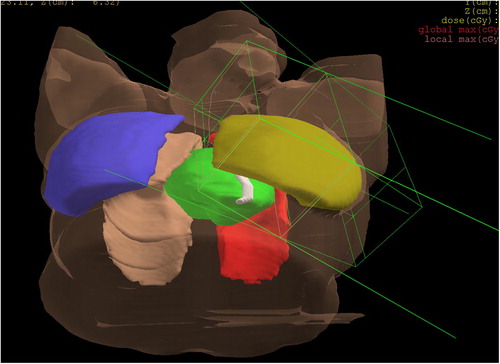
CT slices of selected patients were transferred to Electa Xio treatment planning system. Target volumes include clinical target volume (CTV) and planning target volume (PTV) were outlined according to the Anatomical Boundaries of Breast Cancer Atlas for Radiation Therapy Planning of radiation therapy oncology group (RTOG).Citation17 Organs at risk (OARs) include heart, ipsilateral and contralateral lung were also outlined. The heart was contoured from the cardiac apex to the level of the pulmonary trunk superiorly including the myocardium (excluding pericardium and the major vessels). Right and left lung were contoured separately with the automatic contouring tool of the planning system ().
Figure 2 Room eye view shows PTV in yellow, ipsilateral lung in red, heart in green, contra lateral lung in brown and contra lateral breast in blue.
2.3 Planning process
To define the conventional field borders the border of medial field was marked at mid sternum, and that of lateral field was placed 20 mm dorsally from the lateral palpable breast. The borders of the cranial and caudal field were marked 20 mm beyond the palpable breast.
For each patient in the three positions 3DCRT plans were carried out using two tangential opposed wedged photon beams (6 and 15 MV). To optimize PTV dose coverage the field size was adjusted using beam eye view. Multi leaf collimator (MLCs) was used to shape the PTV and to shield OARs to achieve maximum avoidance of the heart and ipsilateral lung as possible. Gantry angle, wedge angle, and beam weighting were also adjusted. A dose of 50 Gy is prescribed to normalization point according to (ICRU) reference point.Citation18,Citation19
The three plans were compared for target dose coverage, dose homogeneity and organ at risk sparing using dose volume histogram (DVH), dose volume histogram parameters (DVPs) and visual inspection of the dose distribution. Target coverage was assessed using D95% (dose to 95% of the PTV) and Dmax (maximum dose). Dose homogeneity within target volume was assessed by homogeneity index (calculated as D5%/D95%).Citation20 Regarding organs at risk (OARs); lung sparing was assessed using V20Gy (volume of the lung in% that receives 20 Gy or more) and mean dose. Heart sparing was assessed by V5Gy, V10Gy, V25Gy, V30 Gy (volume of the heart in% that receives 5 Gy or more, 10 Gy or more, 25 Gy or more, and 30 Gy or more), mean and maximum heart dose.
2.4 Statistical analysis
Dose volume histograms of the PTV, lungs and heart of the three plans were generated for the fifty patients. Relevant dose volume parameters (DVPs) of the three plans were compared and the differences and percent of reduction of these DVPs among the plans were calculated and tested for any statistically significant differences using Wilcoxon Signed-Ranks test of SPSS version 20 (SPSS Inc., Chicago, IL). A P value of <0.05 was considered statistically significant.
This study had approval of Institutional Review Board as a prospective one in which informed consent was taken from the patients.
3 Results
This study consisted of 50 left sided breast cancer patients. Breast volume ranged from 367 cc to 1366c (mean 930 cc). By reviewing the DVPs of the three treatment plans of all patients, the followings are the results as regard the dose distribution of the PTV and OARs ( & ).
Figure 3 DVH for PTV in yellow, heart in green and Ipsilateral lung in red comparing the target coverage and sparing of ipsilateral lung & heart in supine (A), semi-lateral (B) and semi-lateral decubitus + breath hold techniques (C).
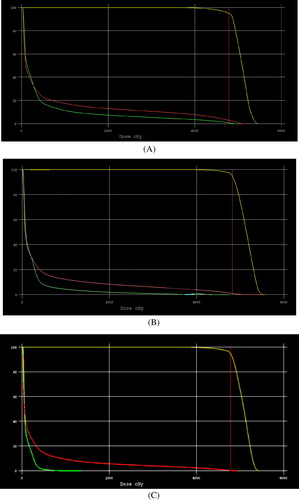
Table 1 Comparison of the average of PTV DVPs in cGy for left sided breast cancer patients irradiated by three different decubitus techniques. P values for the differences between the plans are also shown.
3.1 PTV dose coverage & dose homogeneity
gives the statistical analysis and DVPs for the PTV comparing the three plans. The PTV coverage was adequate and comparable among the three techniques as the differences in PTV D95% & PTV Dmax among the three techniques were not statistically significant (P = 0.304, 0.769 & 0.354) & (P = 0.561, 0.108 & 0.939) respectively. The dose homogeneity within PTV was also comparable for the three techniques (P = 0.444, 0.109 & 0.290) respectively ().
3.2 Dose distribution within organs at risk
gives the statistical analysis and DVPs for heart and both lungs comparing the three plans.
Table 2 Comparison of the average of heart and lung DVPs in cGy and in% for left sided breast cancer patients irradiated by three different decubitus techniques. P values for the differences between the plans are also shown.
3.2.1 Heart
shows a significant reduction of (76%, 72%, 96%, 97%, 54%, 57%, P ⩽ 0.001) & (62%, 70%, 87%, 87%, 27%, 38%, p ⩽ 0.001) respectively in heart V5Gy, V10Gy, V25Gy, V30Gy, mean heart dose & max heart dose with semi-lateral decubitus and breath hold technique compared to supine technique & semi-lateral decubitus technique. There was also a significant reduction in heart V5Gy, V10Gy V25Gy V30Gy and mean heart dose and max heart dose with semi-lateral decubitus (52%, 64%, 73%, 75%, 35%, 25%, P ⩽ 0.001) compared to supine technique ().
3.2.2 Ipsilateral lung
shows a significant reduction in lung V20Gy with semi-lateral decubitus and breath hold technique (25%, P ⩽ 0.001) & (13%, P = 0.003) respectively compared to supine technique & semi-lateral decubitus technique. There was also a significant reduction in lung V20Gy with semi-lateral decubitus (16%, P ⩽ 0.001) compared to supine technique.
also shows a significant reduction in mean lung dose with semi-lateral decubitus and breath hold technique (14%, P ⩽ 0.001) & (5%, P = 0.006) respectively compared to supine technique & semi-lateral decubitus technique. There was also a significant reduction in mean lung dose with semi-lateral decubitus (15%, P = 0.007) compared to supine technique ().
3.2.3 Contralateral lung
shows a none significant reduction of (20%, P = 0.659 & 11%, P = 0.700) & (17%, P = 0.572 & 32%, P = 0.950) in lung V20Gy & mean lung dose with semi-lateral decubitus and breath hold technique compared to supine technique & semi-lateral decubitus technique. There was also a non significant reduction of (12%, P = 0.972 & 37%, P = 0.449) in lung V20Gy & mean lung dose with semi-lateral decubitus compared to supine technique. So the sparing of contra lateral lung was comparable among the three techniques.
This study could not find any significant correlation between the breast volume and the above mentioned heart and lung DVPs (P values >0.05).
4 Discussion
Several treatment techniques have been developed to spare the heart and lung and so to reduce the risk of late cardiac and pulmonary toxicities in women with cancer breast receiving adjuvant radiotherapy.Citation3,Citation4
Breath hold techniques can improve cardiac sparing in the supine treatment position. However some patients are not able to tolerate breath-holds to allow effective treatment delivery so these patients need another method for cardiac and pulmonary structures sparing.Citation21,Citation22
In this regard the current study was undertaken to evaluate and compare the differences in lung and heart dose volume parameters among three simulation techniques; standard supine technique, semi lateral decubitus and semi lateral decubitus and deep inspiration breath hold techniques for left-sided breast cancer patients who underwent breast conservative surgery and adjuvant radiotherapy.
As regard the target coverage; current study revealed that supine, semi lateral decubitus and semi lateral decubitus and deep inspiration breath hold techniques achieved adequate and comparable target coverage. These results are in accordance with the results of Capezzali et al.Citation8 who achieved good coverage of the breast with reduced heart and lung irradiation in the lateral position using three dimentional isocentric technique. The results of the current study are also in accordance with the results of Joo J H et al.Citation4 who found that the use of deep inspiration breath hold (DIBH) during radiotherapy of the left-sided breast reduced the doses delivered to the heart with similar target coverage compared to free breath.
As regard sparing of organs at risks (OARs); in the current study semi-lateral decubitus technique showed greater heart and ipsilateral lung sparing compared to supine technique. Moreover semi-lateral decubitus and breath hold technique provided superior sparing compared to both supine and semi-lateral decubitus techniques.
As regard heart sparing; although the current study showed that the semi-lateral decubitus techniques resulted in greater heart sparing compared to supine technique the semi-lateral decubitus and breath hold technique resulted in superior heart sparing compared to supine and semi-lateral decubitus techniques. Niglas M et al.Citation7 found that mean heart dose and heart V25Gy were significantly lower for both reverse semi lateral decubitus (RSD) and deep inspiration breath hold (mDIBH) when compared to supine technique (P < 0.001 to 0.006). The average values of mean heart dose using these techniques were 10 Gy, 6 Gy and 3.0 Gy respectively. There was a significant dose reductions of (62.4% versus 40.0%, P = 0.004) & (84.9% versus 50.4%, P = 0.003) in mean heart dose & heart V25Gy for mDIBH and RSD compared to supine dose. These results are matched with the results of the current study. Even the current study showed more significant reduction in the heart mean dose, V5Gy,V10Gy,V25Gy, and V30Gy because the semi lateral decubitus and mDIBH were combined. Bartlett F R et al.Citation23 found that the breath-hold techniques reduced the amount of radiation received by heart during left breast radiotherapy. These results are also in accordance with the results of the current study. Stranzl H & Zurl BCitation24 achieved significant reduction of 56% in the mean heart dose for the DIBH technique compared to the normal breathing (mean heart dose 2.3 Gy vs. 1.3 Gy; P = 0.01). These results are in accordance with the results of the current study. Smyth L M et al.Citation25 carried out ten studies about the benefits of DIBH during left breast irradiation. They found that DIBH reduced the mean heart dose by up to 3.4 Gy when compared to a free breathing technique. These results are in accordance with the results of the current study where 1.8 Gy reduction in mean heart dose was achieved with semi lateral decubitus and breath hold technique compared to supine technique with free breathing.
In the current study the average values of mean cardiac dose were (304.45 cGy, 183.34 cGy and 119.8 cGy) in supine, semi lateral and semilateral decubitus and breath hold techniques respectively. V5Gy, V10Gy, V25Gy and V30Gy values for supine, semi lateral, semilateral and breath hold decubitus techniques were (V5Gy 8.9%, 5.13%, 1.81%) & (V10Gy 5.73%, 2.47%, 0.66%) & (V25Gy 3.05%, 1.02%, 0.19%) and (V30Gy 2.27%, 0.78%, and 0.13%) respectively. The heart maximum dose was 4552 cGy, 3536 cGy and 2006 cGy for supine, semi-lateral decubitus and semi-lateral decubitus and breath hold techniques respectively. These results are matched with the results achieved by Joo J H et al.Citation4 In their study they evaluated cardiac dose reduction of tangential breast irradiation with deep inspiration breath hold. They found that the average of heart mean dose also decreased from 724.1 cGy in FB to 279.3 cGy in DIBH (P < 0.001). The relative amount of heart volume irradiated with 10 Gy–50 Gy was consistently reduced with DIBH. The V10Gy, V20Gy, V30Gy, V40Gy, and V50Gy values for FB vs DIBH were 14.6% vs 4.0% (−73%), 12.3% vs. 2.7% (−78%), 10.7% vs. 2.0% (−82%), 8.7% vs. 1.3% (−85%), and 2.5% vs. 0.2% (−91%) respectively.
As regard Ipsilateral Lung sparing; although the current study showed that the semi-lateral decubitus techniques resulted in greater ipsilateral lung sparing compared to supine technique the semi-lateral decubitus and breath hold technique resulted in superior Ipsilateral Lung sparing compared to supine and semi-lateral decubitus techniques.
The results of the current study are in accordance with Kirova Y M et al.Citation26 study who achieved excellent dosimetric profile, with low doses to the heart and ipsilateral lung with the lateral decubitus position for patients with large breasts and early-stage breast cancer. The results of the current study are also in accordance with Capezzali G et al.Citation8 who found that irradiation of the heart and lungs is extremely low in the isocentric lateral decubitus (ILD) position despite the good coverage of the breast. In accordance with the results of the current study Campana, F et al.Citation27 found that breast radiotherapy in the lateral decubitus position reduced lung and heart irradiation over the conventional technique with opposing tangential fields. In contrast to the results of the current study Niglas M et al.Citation7 found no significant reduction for lung V20Gy or V5Gy cardiac dose sparing using the reverse semi-decubitus technique for left breast and internal mammary chain irradiation.
5 Conclusions
Semi-lateral decubitus techniques with and without breath hold for left sided breast cancer patients significantly reduce the dosimertic parameters of the ipsilateral lung and heart compared to supine technique with comparable target dose coverage.
Conflict of interest
I declare that there is no conflict of interest with any financial organization regarding the material in this manuscript.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 9 January 2017
References
- A.JemalR.SiegelJ.XuE.WardCancer statistics, 2010CA J Clin602010277300
- J.P.JulienN.BijkerI.S.FentimanRadiotherapy in breast- conserving treatment for ductal carcinoma in situ: first results of the EORTC randomized phase III trial 10853. EORTC breast cancer cooperative Group and EORTC Radiotherapy GroupLancet3552000528533
- ChiragShahShahedBadiyanSameerBerryCardiac dose sparing and avoidance techniques in breast cancer radiotherapyRadiother Oncol1122014916
- R.E.BeckL.KimN.J.YueB.G.HafftyA.J.KhanS.GoyalTreatment techniques to reduce cardiac irradiation for breast cancer patients treated with breast-conserving surgery and radiation therapy: a reviewFront Oncol42014327
- V.M.RemouchampsF.A.ViciniM.B.SharpeSignificant reductions in heart and lung doses using deep inspiration breath hold with active breathing control and intensity-modulated radiation therapy for patients treated with locoregional breast irradiationInt J Radiat Oncol Biol Phys552003392406
- J.H.JooCardiac dose reduction during tangential breast irradiation using deep inspiration breath hold: a dose comparison study based on deformable image registrationRadiat Oncol102015
- M.NiglasC.McCannB.M.KellerA dosimetric study of cardiac dose sparing using the reverse semi-decubitus technique for left breast and internal mammary chain irradiationRadiother Oncol11812016187193
- G.CapezzaliLeft breast cancer treated in Isocentric Lateral Decubitus (ILD) position: an alternative technique sparing Organs at Risk (OAR)Glob J Breast Cancer Res120135357
- A.FogliataA.BolsiL.CozziCritical appraisal of treatment techniques based on conventional photon beams, intensity modulated photon beams and proton beams for therapy of intact breastRadiother Oncol622002137145
- Y.HamaProne positioning causes the heart to be displaced anteriorly within the thorax: implications for breast cancer treatmentInt J Radiat Oncol Biol Phys7212008302
- T.E.MerchantB.McCormickProne position breast irradiationInt J Radiat Oncol Biol Phys301994197203
- L.CozziA.FogliataG.NicoliniClinical experience in breast irradiation with intensity modulated photon beamsActa Oncol442005467474
- A.FongR.BromleyM.BeatD.VienJ.DineleyG.MorganDosimetric comparison of intensity modulated radiotherapy techniques and standard wedged tangents for whole breast radiotherapyJ Med Imaging Radiat Oncol5320099299
- SafaeMansouriAsmaaNaimLuisGlariaHugoMarsigliaDosimetric evaluation of 3-D conformal and intensity-modulated radiotherapy for breast cancer after conservative surgeryAsian Pacific J Cancer Prevent1511201447274732
- R.JagsiJ.MoranR.MarshEvaluation of four techniques using intensity modulated radiation therapy for comprehensive locoregional irradiation of breast cancerInt J Radiat Oncol Biol Phys78201015941603
- M.FagundesE.B.HugM.PankuchProton therapy for local-regionally advanced breast cancer maximizes cardiac sparingInt J Particle Ther142015827844
- http://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx.
- Prescribing, recording and reporting photon beam therapy. International commission on Radiological Units and Measurements (ICRU) Report # 50: ICRU 1993.
- Prescribing, recording and reporting photon beam therapy. International commission on Radiological Units and Measurements (ICRU) Report # 62: ICRU 1997.
- A.HelalA.OmarHomogeneity index: effective tool for evaluation of 3DCRTPan Arab J Oncol8220152023
- K.E.HensonRadiation-related mortality from heart disease and lung ancer more than 20 years after radiotherapy for breast cancerBr J Cancer10812013179182
- S.C.DarbyRisk of ischemic heart disease in women after radiotherapy for breast cancerNew Engl J Med368112013987998
- F.R.BartlettVoluntary breath-hold technique for reducing heart dose in left breast radiotherapyJ Vis Exp892014
- H.StranzlB.ZurlPostoperative irradiation of left-sided breast cancer patients and cardiac toxicity. Does deep inspiration breath-hold (DIBH) technique protect the heart?Strahlenther Onkol18472008354358
- L.M.SmythK.A.KnightY.K.AaronsJ.WasiakThe cardiac dose-sparing benefits of deep inspiration breath-hold in left breast irradiation: a systematic reviewJ Med Radiat Sci62120156673
- Y.M.KirovaWhole breast radiotherapy in the lateral decubitus position: a dosimetric and clinical solution to decrease the doses to the organs at risk (OAR)Radiother Oncol11032014477481
- F.CampanaBreast radiotherapy in the lateral decubitus position: a technique to prevent lung and heart irradiationInt J Radiat Oncol Biol Phys615201513481354