
Abstract
Objective
To evaluate the role of MRI in differentiation of benign from malignant breast lesions using dynamic contrast enhanced MRI (DCE-MRI) and diffusion weighted MRI (DW-MRI).
Patients and methods
The study included 33 female patients with clinically suspicious breast lesions detected by mammography and/or breast ultrasound. Cases were referred from general surgery departments in Tanta university hospital. The patients underwent full history taking and clinical examination, full field digital mammography and US, for those patients cases diagnosed on sonomammography as BI-RADS 3 & 4 were selected for MRI examination.
Results
Quantitative analysis of DWI was done for the 33 breast lesions and their ADC values are recorded at 3 different b-values (250, 600, and 1000). Seventeen lesions showed facilitated diffusion, proved to be benign and 10 lesions showed restricted diffusion, 9 lesions of them proved to be malignant and one proved to be benign. There are 6 lesions showed mixed restricted and facilitated diffusion proved to be malignant.
Conclusion
DWI improves the diagnostic ability of the DCE-MRI of the breast. It is a better method for detecting breast lesions than either T1- or T2-weighted imaging, but it is better to be performed in conjunction with contrast enhanced MRI.
1 Introduction
Breast cancer is now a significant cause of worldwide morbidity and mortality. Further, the increasing rate of breast cancer continues to be a major area of concern for both clinicians and researchers. Increased awareness in the affected population leads to more frequent physical examinations and diagnostic imaging procedures which results in earlier diagnosis and hence improved prognosis.Citation1
Figure 2 MRI T1WI, T2WI & STIRWI (A–C): revealed bilateral multiple lesions with low signal intensity in T1WI, high signal intensity in T2WI & STIRWI. DCE-MRI (D): revealed non enhancement of the lesions. DW-MRI with post processing ADC maps at b-values 250 (E, F), 600 (G, H): revealed facilitated diffusion of the lesion with ADC value of region of interest 1.8 × 10−3 mm2/s confirming benignity.MRI scanning: BI-RADS category 2. The patient subjected to follow up after 6 months and no change occur.
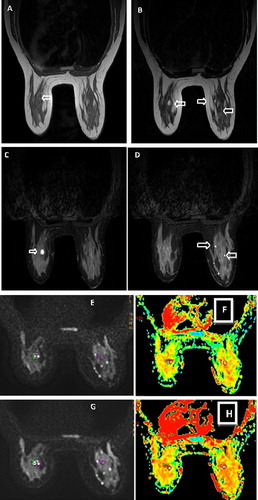
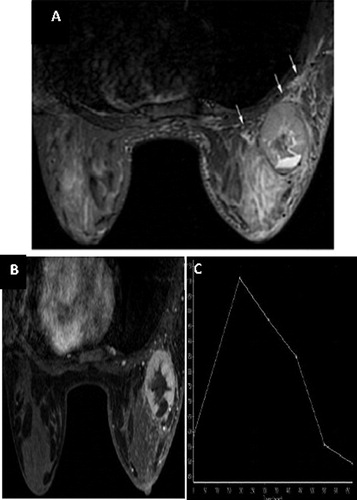
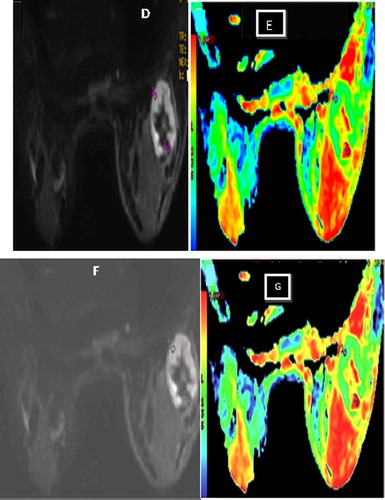
Figure 3 MRI STIRWI (A): of both breasts revealed LT breast isointense lesion with central hyperintensity with surrounding prepectoral oedema. DCE-MRI (B) & time/signal intensity curve (C): of the left breast lesion showed rim-enhanced mass with a thick wall and smooth margin, its time signal intensity curve of the lesion showed rapid slope up and rapid wash out (curve type III) DW-MRI with post processing ADC maps at b-values 600 (D, E) & 1000 (F, G): the mass showed peripheral hyperintensity on DWI. The corresponding ADC map shows the ADC value of the wall is 1.04 × 10−3 mm2/s, the central part, 2.70 × 10−3 mm2/s MRI scanning: BI-RADS category 5. The lesion was biobsied and the biobsy revealed invasive ductal carcinoma.
Nowadays MRI of the breast is frequently applied when other diagnostic modalities fail to find a primary source in the breast, remarkable advances in MRI technology have allowed sensitive detection and anatomic definition of cancer, and the introduction of MRI in several aspects of breast cancer diagnosis and management.Citation2
Dynamic contrast-enhanced MRI (DCE-MRI) and diffusion weighted MRI (DW-MRI) are currently used as an adjunct to mammography in women at high risk, or those with extremely dense breasts, selective “problem-solving” or adjunct diagnosis where standard clinical and imaging evaluation do not provide a clear diagnosis, imaging of breast silicone implants, monitoring response to neoadjuvant (primary), systemic therapy in locally advanced disease, irradiated breasts, and postsurgical breasts or highly invasive breast cancers.Citation3
In addition, using DWI & ADC values are reportedly useful in differentiating benign from malignant breast lesions and in the detection of breast cancer without administration of contrast medium. Hence, DWI could be a promising tool in screening for breast cancer without using contrast medium, especially for patients with renal dysfunction or previous reactions to contrast agents and will relieve the cost of examination.Citation4,Citation5
The aim of the study was to evaluate the role of the magnetic resonance imaging in differentiation of benign from malignant breast lesions using dynamic contrast enhanced MRI (DCE-MRI) and diffusion weighted MRI (DW-MRI).
2 Patients and methods
The current study included 33 female patients with clinically suspicious breast lesions detected by mammography and/or breast ultrasound; their age range was 30 & 65 years. The study was conducted in Tanta university hospital during the period from March 2013 to April 2015. Cases were referred from general surgery departments in Tanta university hospital. The patients underwent full history taking and clinical examination, full field digital mammography and US, for those patients cases diagnosed on sonomammography as BI-RADS 3 & 4 were selected for MRI examination.
Patients were excluded from the study in case of contraindications to perform MRI, (patients with metallic foreign body or cardiac pacemakers, claustrophobic and uncooperative patients, patients could not lie prone, patients who were allergic to contrast media, patients with disturbed renal functions and patients who refused the examination).
An informed consent was obtained from patients included in the study; an approval was obtained from the ethics committee.
Magnetic resonance imaging, dynamic contrast enhanced MRI was performed for the 33 patients included in the study with high field strength 1.5 T on high signa (general electric medical system) high speed using dedicated double breast coil.
Patient preparation: All metallic subjects were far from the patient body including zippers and clasps. Intravenous line was established for further gadolinium injection.
Patient positioning: The patient lied prone with breasts positioned onto the breast coil and checked to be as deep and as centered in the coil as possible, with the nipple faced straight down. The patient comfortability was checked and patients instructed not to move during the period of examination.
Coronal T1 weighted spin echo sequence was carried out for localization purpose and followed by plain sequences using T1weighted fast spin echo sequence (TR = 501 ms, TE = 10 ms, FOV = 24 × 24 cm),in addition to T2 weighted fast spin echo sequence (TR = 4131 ms, TE = 120 ms, FOV = 36 × 28 cm) & STIR weighted fast spin echo sequence (TR = 3660 ms, TE = 103 ms, FOV = 36 × 23.4 cm) in axial orientation and/or sagittal orientation.
A bolus of gadolinium dimeglumine (Gd-DTPA) was injected manually intravenous at a dose of (0.1 mmol/kg) followed by saline flush to ensure that contrast – enhanced images could be obtained immediately after contrast agent injection.
DWI was performed using a diffusion-weighted echo-planar imaging (EPI) sequence with parallel imaging (GE machine); reduction factor, 2; 7,000/71.5; number of excitations, 2; matrix, 240 × 240; field of view, 34 cm; slice thickness, 3 mm; and gap, 0. Diffusion gradients were applied in six directions with b value = 600 and 1000 s/mm2, and the scanning time was 4 min. Respiratory triggering was used for better resolution.
Image post processing on the work station: Diffusion maps were formed. A noise-level threshold of 200 was applied to mask the b = 0 s/mm2 images before forming diffusion maps.
An ROI was defined for each DCE-MRI–detected lesion at the corresponding location on the combined DWI (SDWI) series. The mean ADC of the voxels in the ROI was calculated for each lesion. Quantitative analysis was done by placing the ROI at the most enhanced part within the lesion result in automatically created time/ signal intensity curve.
2.1 Image analysis
The MRI images were evaluated as follow: T1 weighted images, T2 weighted images and STIR weighted images were first examined to detect presence of any abnormality, determination of MR appearance of the lesion(cystic, solid or mixed), location of the lesion, definition of the lesion (well or ill-defined), signal intensity of the lesion, the presence of lymph nodes.
Dynamic contrast enhanced images were examined to detect the presence or absence of lesion enhancement. Lesions interpretation took place as follow :Its shape (regular or irregular(,its border (well defined, ill defined, speculated, pattern of enhancement (homogenous, heterogeneous or ring enhancement(, dynamic behavior of the mass with evaluation of the percentage of enhancement as well as the shape of time/signal intensity curve (type I, type II or type III) was studied.
Diffusion – weighted images and ADC maps are then examined and the mean ADC of each lesion. The quantitative analysis of DWI, we generated the ADC maps from the DWI from b values (600 and 1000), then ADC values are automatically calculated on the work station.
MRI BIRADS classification was applied for each lesion based on the combination of morphologic and kinetic criteria, there were not any cases categorized as BI-RADS category I, Lesions that categorized as BI-RADS category 2 & 3 subjected to follow up after 6 months while lesions categorized as BI-RADS category 4 & 5 were correlated with histopathological result.
2.2 Statistical analysis
The role of MRI (DWI & DCE-MRI) in detection and characterization of breast focal lesions was evaluated and compared with histopathology (for fifteen cases) and multi-modality with clinical follow-up (for the remaining eighteen cases) which were considered the gold standard of reference were statistically described in terms of range, mean ± standard deviation (±SD), frequencies (number of cases) and percentages when appropriate. Data entry was done by SPSS version 16 and analyzed by the same software. The final diagnosis was confirmed by follow up after 6 months in 18 female patients whom classified as BI-RADS category 2 and 3 as the patients with BI-RADS category 2 had past history of breast cancer. The final diagnosis was confirmed by FNAC in 15 female patients whom classified as BI-RADS category 4 and 5.
3 Results
All the 33 patients included in the study which their ultrasound and/or mammography were suspicious besides their suspicious past history were referred for MRI examination. Description of MRI findings using BI-RADS included, the lesion type if mass or non- mass lesions. Regarding the mass lesions, the description including basic morphological criteria of solid mass lesions including shape, margin, mass enhancement and the kinetic curve assessment. The number of mass lesions in our study was 27 lesions (as shown in ).
Table 1 BIRADS descriptor criteria by MRI of studied 27 mass breast lesions.
There are 6 non- mass lesions in our study. The BI-RADS description applied for the non mass lesions included, distribution modifiers and the internal enhancement characteristics (as shown in ).
Table 2 BIRADS descriptor criteria by MRI of studied 6 non mass breast lesions.
Dynamic contrast enhanced MRI showed 33 mass and non mass breast lesions, 21 lesions showed homogenous enhancement, 12 of them were benign and the other 9 lesions were malignant. Six lesions showed heterogeneous enhancement all of them were malignant. Six lesions were not enhanced; all of them were benign (as shown in ).
Table 3 The MR enhancement characteristics of mass and non mass lesions.
In this study the 27 enhanced breast lesions, their time signal intensity curve were assessed, regarding their initial rise (slow, medium or rapid) and their delayed phase (persistent, plateau or washout). DCE-MRI revealed 3 lesions with progressive rising time/signal intensity curve (type I curve). Nine lesions showed slow wash in, slow wash out with plateau curve (type 2 curve). Nine lesions showed rapid slope up and rapid wash out (type 3 curve). There are 6 lesions showed more than one type of time/signal intensity curve, 3 lesions of those 6 lesions showed type 2 and type 3 curves, other 3 lesions showed the three types of curves (as shown in ).
Table 4 Shows the type of time/signal intensity curve of 27 enhanced breast lesions.
Diffusion weighted - MRI was done for the 33 breast lesions. They were classified according to their criteria on unenhanced MRI to benign and malignant lesions regarding to their signal intensity on DWI-MRI. There were 27 which displayed as hyper intensities on DWI-MRI, 12 of them were benign and 15 lesions were malignant. There were 6 lesions who displayed as hypo intensities on DWI-MRI, all of them were benign (as shown in ).
Table 5 classification of the examined 33 breast lesions according to their criteria on DW-MRI.
Quantitative analysis of DWI was done for the 33 breast lesions and their ADC values are recorded at 3 different b-values (250, 600, and 1000). Seventeen lesions showed facilitated diffusion, proved to be benign and 10 lesions showed restricted diffusion, 9 lesions of them proved to be malignant and one proved to be benign. There are 6 lesions showed mixed restricted and facilitated diffusion proved to be malignant (as shown in ).
Table 6 Classification of the examined 33 breast lesions according to their criteria on unenhanced breast MRI.
The decision of final assessment category was based on the criteria of the lesions on basic MRI sequences (T1 W, T2 W, STIRW), DCE-MRI, DWI and recorded ADC values on the ADC map (as shown in ) –.
Figure 1 MRI STIRWI (A): of the left breast revealed well defined abnormal signal intensity at the deep retroareolar region with heterogeneous signal intensity. DCE-MRI (B): revealed the retroareolar lesion not enhanced. DW-MRI with post processing ADC maps at b-values 600 (C& D) & 1000 (E & F) : revealed facilitated diffusion of the lesion with ADC value of region of interest 1.7 × 10−3 mm2/s confirming benignity.MRI scanning : BI-RADS category 2. Follow up of the patient after 6 months revealed no abnormality.
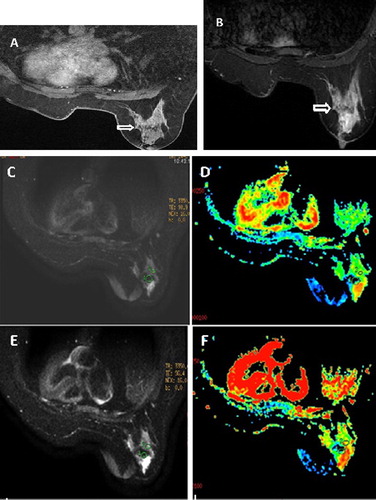
Figure 4 MRI STIRWI (A): of both breasts revealed RT breast hyperintense lesion with nipple retraction .DCE-MRI(B) & time/signal intensity curve (C): of the right breast lesion showed rim-enhanced mass with irregular margin with time signal intensity curve showed gradual slow slope up with gradual enhancement (curve type 1) indicating benignity. DW-MRI with post processing ADC maps at b-values 600 (D&E) & 1000 (F&G): the mass showed central hyperintensity on DWI. The corresponding ADC map shows the ADC value of the wall is 1.33 × 10−3 mm2/s, the central part, 0.861 × 10−3 mm2/s. MRI scanning: BI-RADS category 2.Pathology revealed lactating abscess.
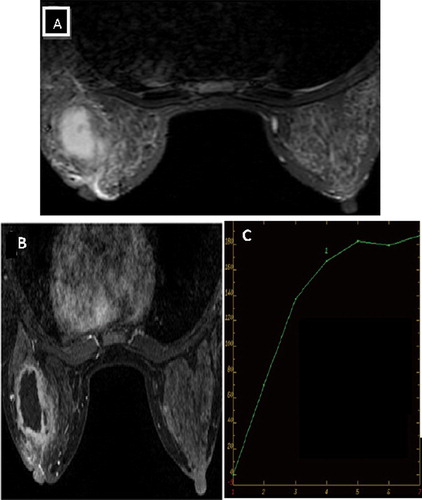
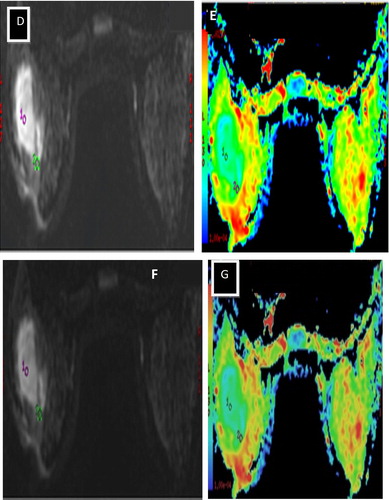
Table 7 Final assessment BI-RADS category of the 33 studied female patients with breast lesions.
4 Discussion
Dynamic contrast-enhanced MRI of the breast has high ability for breast lesions detection. DCE-MRI is also more accurate than mammography or ultrasound for the delineation of the extent of disease in patients with a recent diagnosis of cancer but limited ability for discrimination between benign and malignant lesions.Citation6
Diffusion weighted MR imaging (DWI) has recently been reported to demonstrate usefulness in differentiating benign from malignant breast lesions and for monitoring treatment response after chemotherapy or radiation, for differentiating post therapeutic changes from residual active tumor, and for detecting recurrent cancer.Citation7 Potential additional roles include predicting treatment outcomes (before and soon after starting therapy), for tumor staging, and perhaps also for detecting lymph node involvement by cancer.Citation8
DWI is quantified by ADC values, which is a calculated measure of water diffusion through the tissues. ADC values vary between malignant and benign breast lesions, whereby the ADC values of malignant breast lesions are usually lower than those of benign lesions, indicating restricted water diffusion and increased cellularity. The ADC values of benign lesions are higher, reflecting normal cellularity and no restriction of water movement. Nevertheless, there is overlap as benign breast changes can mimic malignancies.Citation9,Citation10
Our study included 33 patients with 33 breast lesions to evaluate the role of DWI as an adjunct to DCE-MRI in the probably benign and suspicious breast lesions after mammographic and/or ultrasonographic examinations. The patients included in this study were selected according to their clinical presentation, the patient past history, the appearance of lesion in the ultrasound or mammography (suspicious lesions were selected).
The final diagnosis was confirmed by follow up after 6 months in 18 female patients whom classified as BI-RADS category 2 and 3 as the patients with BI-RADS category 2 had past history of breast cancer. The final diagnosis was confirmed by FNAC in 15 female patients whom classified as BI-RADS category 4 and 5.
In this study it was found that the lesions with smooth margin (well defined) were 15 lesions and all were benign while the lesions with irregular and speculated margin were all malignant. This is comparable with Macura et al. Citation11 who reported that the margin description of a focal mass is the most predictive feature of the breast MR image interpretation and speculated margin are more suspicious for carcinoma.
In this study DCE-MRI of mass lesions was done which revealed 24 enhanced lesions and 3 non enhanced lesions. Twenty-one lesions with homogenous enhancement 12 of them were benign and the other 8 lesions were malignant. The lesions with heterogeneous enhancement were 3 lesions and all were malignant. In the non mass lesions in the present study, 3 lesions were with focal area of enhancement while 3 lesions were not enhanced. In the present study, in case of mass like enhancement it was found that the heterogeneous enhancement indicative for malignant lesions while homogenous enhancement is likely to occur in benign lesions While non mass lesions no specific criteria for the enhancement pattern, and this confirms the study conducted by Tozaki et al. Citation12 Who reported that the most frequent morphological finding among the malignant lesions was heterogeneous internal enhancement.
In the present study DCE-MRI time signal intensity curve revealed 3 lesions showed progressive raising curve (type I curve), by histopathology the 3 lesions were benign. 9 lesions showed plateau curve (type II curve), all the 9 lesions were benign. 15 lesions showed rapid wash out (type III curve) all proved by histopathology as malignant. This is comparable with many studies that reported the importance of the curve shape in differentiating between malignant and benign lesions. The use of time- signal intensity curves resulted in dramatically higher discrimination between benign and malignant lesions. Type III curve is more suspicious for malignancy, whereas persistent curves are associated with benign lesions. Plateau curves are indicative of either malignant or benign lesions. Schnall et al. Citation13
In this study there was one false positive case which was on unenhanced MRI T1WI,T2WI and STIRWI appeared well defined with homogenous enhancement on DCE-MRI with time/signal intensity curve of type 2 but on DWI showed restricted diffusion with ADC value 0.7 × 10−3 mm2/s, but by histopathology proved to be benign (fibroadenoma). So in our study the DWI technique had false positive result, this confirms the study conducted by Fornasa et al. Citation14 which during the study detect 2 false positive cases one of them was fibroadenoma.
In this study we calculated the ADC value with two different b- values (600 & 1000). In this study there was no any difference between the ADC values detected at different b-values. The results imply that to differentiate benign from malignant breast lesions. This confirmed the study conducted by Chen et al. Citation15 which reported that varying the b-values does not influence the conspicuity of breast lesions on DWI at 1.5 T.
In conclusion DWI improves the diagnostic ability of the DCE-MRI of the breast. It is a better method for detecting breast lesions than either T1- or T2-weighted imaging, but it is better to be performed in conjunction with contrast enhanced MRI.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 15 February 2017
References
- W.A.BergZ.ZhangD.LehrerDetection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer riskJama307201213941404
- M.ChenW.ZhanB.HanAccuracy of physical examination, ultrasonography, and magnetic resonance imaging in predicting response to neo-adjuvant chemotherapy for breast cancerChin Med J125201218621866
- C.KuhlThe current status of breast MR imaging part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practiceRadiology24420072
- S.G.OrelDifferentiating benign from malignant enhancing 5 lesions identified at MR imaging of the breast: are time intensity curves an accurate predictor?Radiology211199957
- M.D.SchnallJ.BlumeD.A.BluemkeDiagnostic architectural and dynamic features at breast MR imaging: multicenter studyRadiology23820064253
- N.HyltonOptimizing your breast MRI techniqueInternational Society for Magnetic Resonance in Medicine (SMRM)182200613401342
- C.ŞahinE.ArıbalThe role of apparent diffusion coefficient values in the differential diagnosis of breast lesions in diffusion-weighted MRIDiagn Interv Radiol192013457462
- M.TozakiE.Fukuma1H MR spectroscopy and diffusion-weighted imaging of the breast: are they useful tools for characterizing breast lesions before biopsy?AJR1932009840849
- Hayes DF.: Normal Anatomy and Development, In: Atlas of Breast Cancer, 2nd ed., Mosby, 2000; (3)3.2-3.
- Kaiser W A.: MR-Mammography, Graham A. Webb, Modern Magnetic Resonance, Part II, 2008; P: 1127–1141.
- K.J.MacuraR.OuwerkerkM.A.JacobsPattern of enhancement on breast MR images: interpretation and imaging pitfallsRadio Graph26200617191734
- M.TozakiK.FukudaHigh-spatial-resolution MRI of non-masslike breast lesions: interpretation model based on BI-RADS MRI descriptorsAJR1872006330337
- M.D.SchnallS.RostenS.EnglanderA combined architectural and kinetic interpretation model for breast MR imagesAcad Radiol82001591597
- F.FornasaL.PinaliA.GaspariniDiffusion-weighted magnetic resonance imaging in focal breast lesions: analysis of 78 cases with pathological correlationRadiol Med1162011264275
- X.ChenX.J.HeR.JinConspicuity of breast lesions at different b values on diffusion-weighted imagingBMC Cancer.22012334