
Highlights
| • | All antiretroviral therapies (ARTs) are potentially toxic to the liver. The rising incidence of ART induced adverse events has led to guideline revision. | ||||
| • | The rising incidence of ART induced adverse events has led to guideline revision. Limited studies to date evaluating ART induced liver injury in these countries. This need to be addressed to guide future clinical practice. | ||||
| • | Majority of patients developed significant ALT elevation within 3 months of ART initiation. No significant difference between mean ALT levels at baseline and month 6. | ||||
| • | Patients with high risk of hepatocellular damage, female sex, and > grade 2 ALT elevations, and patients who test positive for HBV/HCV, should be monitored for at least 6 months after initiation of NVP and EFV based ART. | ||||
Abstract
Introduction
All antiretroviral therapies (ARTs) are potentially toxic to the liver. In sub-Saharan Africa, the rising incidence of ART induced adverse events has complicated treatment leading to recent revisions of Namibian ART guidelines. Unfortunately there have been limited studies to date evaluating ART induced liver injury in Namibia to guide further revisions if needed.
Objective
Determine the current patterns and grades of ALT elevation in Namibia’s HIV/AIDS.
Methods
Retrospective cohort analysis. Patterns of alanine amino transferase (ALT) liver enzyme elevation were determined in a cohort of ART naïve HIV patients on firstline ART regimen in a referral hospital in Namibia over a 1 year treatment period. Patterns of ALT changes at baseline, 3 months and 6 months were analyzed using ANOVA and Bonferroni test for pairwise comparisons.
Results
Of 79 eligible patients, 72 developed significant ALT elevation within 3 months of ART initiation (F (3, 76) = 6.4, p = 0.002, η2 = 0.193). Four 4 (5.6%) and 1 (1.38%) patient respectively developed grade 2 and grade 3 ALT elevation by month 3. There was no significant difference between mean ALT levels at baseline and month 6. A CD4 count of <350 cells/mm3; female gender and age over 40 years were the main factors associated with moderate or severe ALT elevation.
Conclusions
First line ART commonly induces mild self-limiting liver enzyme elevation in Namibian HIV patients especially in the first 3 months. Consequently, there is a need to monitor ALT levels for at least 3 months after initiation mainly in high risk patients to reduce side-effect concerns. This is already happening.
1 Introduction
HIV/AIDS has devastated public health in sub-Saharan Africa. This is a concern since this region despite being resource constrained hosts over 80% of the world’s HIV patients.Citation1 Within Africa, UNAIDS ranks Namibia among countries with the highest prevalence of HIV/AIDS among adults aged 15–49 years (14.3%), with currently over 250,000 people out of a population of 2.3 million in Namibia living with the infection.Citation2,Citation3 Since the rollout of antiretroviral therapy (ART) in Namibia in 2003, over 104, 531 (80%) HIV/AIDS patients have been initiated on treatment.Citation3,Citation4 Recently the test and treat policy has led to a considerable scale up of patients on first-line ART regimens. Unfortunately scale-up of ART exposes some patients to adverse drug reactions (ADRs)Citation5–Citation10 with liver damage characterized by an elevation of alanine aminotransferase (ALT) being the most common.Citation11–Citation14 Pharmacovigilance reports in Namibia have shown an increasing incidence in adverse effects that parallel the scale-up of ART,Citation15 particularly with stratification by CD4 count,Citation15–Citation20 female sexCitation12,Citation20 and the use of non-nucleoside reverse transcriptase inhibitors (NNRTIs).Citation19-Citation25

The high number of female patients initiating ARTCitation15,Citation26 is an important risk factor for ART induced adverse effects including renal impairment - with hormonal differences playing a part.Citation15,Citation21 Despite these risk factors, ART initiation policies in Namibia has evolved based on increasing CD4 thresholds: 250 cells/mm3 (2003); 350 cells/mm3 (2010); 500 cells/mm3 (2014) and currently to test and treat.Citation27–Citation29 Unfortunately to date, there have been only a limited number of studies evaluating the grades and risk factors for ART induced hepatotoxicity among the Namibian HIV/AIDS population. This is particularly important as the risk for ART induced hepatotoxicity among HIV patients in Namibia may be heightened by the high rates of tuberculosis (TB),Citation30 high alcohol consumption per capita (12.28 L per person per year)Citation31 and the use of efavirenz and/or nevirapine based therapies as first line ART treatment in line with recommendations.Citation20,Citation22–Citation25,Citation27–Citation29 TB coinfection and co-medication is an important risk factor for hepatotoxicity.Citation32,Citation33 Liver damage characterized by elevation in liver transaminases through alanine amino transferase (ALT) is the most reliable marker for hepatocellular toxicityCitation11,Citation20,Citation34–Citation36; however, it’s measurement among patients on firstline ART in Namibia is currently unknown. The routine monitoring of ALT in Namibia is complicated by limited human resource capacity, which may negatively impact on treatment outcomes in some patients.
Consequently, the aim of this paper was to determine the current patterns and grades of ALT elevation in Namibia’s HIV/AIDS population to provide future guidance to the authorities in Namibia and other African countries with similar profiles of patients with HIV. This is because ADRs negatively impact on treatment adherence,Citation16 health related costs, and the social-psychological wellbeing of patientsCitation37 as well as patient outcomes including their quality of life.Citation8,Citation38–Citation42 Increased morbidity and mortality related to ADRs is the main reason for revision and switching ART treatment as seen in the HIV guidelines in the Namibia.Citation8,Citation9,Citation27–Citation29,Citation43 The use of AZT based regimens from 2003 to 20,010 was associated with anemia, and stavudine (d4T) based regimens from 2010 to 2015 was associated with peripheral neuropathy.Citation27–Citation29 The currently preferred Tenofovir-based regimensCitation15 have been associated with renal insufficiency and bone dimineralization.Citation15,Citation20,Citation43 Despite these risk factors for liver damage among the Namibian population, evidence on patterns and prevalence of liver toxicity remains limited.
2 Methods
2.1 Study subjects
The study adopted a retrospective cohort analysis of grades and risk factors for ALT elevation among patients on firstline ART regimens. The study population consisted of clinical and laboratory records of patients initiated on first-line ART at Katutura Intermediate Hospital (KIH). This is a teaching referral hospital in Windhoek; the capital city of Namibia, and cares for over 5800 patients on active ART from across the Khomas region and Namibia.
Retrospective data was collected over a 12 month period between 1st January 2013 and 1st January 2014. The study included records of all adult HIV/AIDS patients (≥18 years) who completed at least 12 months of treatment of first line ART regimen.
The first line regimens in this study included tenofovir/lamivudine/nevirapine (TDF/3TC/NVP) or tenofovir/lamivudine/efavirenz (TDF/3TC/EFV) combinations. For consistency and reliability, only records on ALT levels that had been provided by the National Institute of Pathology (NIP) laboratory at KIH were included. All the serum levels of ALT of records included in this study were determined by Architect ci8200 Dxc analyzer (Abbot Diagnostics) as per the International Federation Clinical Chemistry protocol (IFCC). Patients with severe ALT elevation at baseline and/or with missing laboratory records on ALT levels at 3 months and or 6 months were excluded from the study.
Out of the 123 patients who had the first line ART at KIH between January 2013 and 31 January 2014, 44 patients were excluded as their records did not have ALT measurements at month 3 or month 6. Consequently, a total of 79 patient records that met the eligibility criteria were included in the study.
2.2 Procedure
Laboratory data on the liver enzyme (AST) and (AST) profiles of ART naïve patients were collected using quantitative methods over a 12 month period and five time points - baseline and months 3, 6, 9 and 12 of treatment. Data from the patients’ records were abstracted by the principal researcher (PAM) from patient ART treatment records over a 3 months study period - May 2014 to August 2014 using a pre-tested abstraction tool (Appendix A). Data abstracted includes demographic, clinical and laboratory data at baseline, 3 and 6 months. Data collection tools were designed to exclude patient identifiable data including patient names.
The main outcome variable was the grades and risk factors for ALT elevation at 3 months and 6 months of ART treatment. Data was double entered into Epidata® (version 3.1) entry software for management and exported to SPSS® (version 21) software for quantitative analysis. The grades of ALT elevation were determined using descriptive statistics such as frequencies (%), mean(X) and standard deviation (SD). The risk factors and patterns of ALT elevation were determined using a chi-square test (χ2) for categorical variables and student t-test and/or ANOVA test for continuous variables. The Bonferroni pair-wise Post-hock test was used to compare the mean ALT levels at baseline with months 3 and month 6 post ART initiation. The significance level for a 95% confidence interval was set at a p value < 0.05. Missing data were excluded in the analysis.
2.3 Criteria for grading ALT elevation
The grades of ALT elevations were determined using the WHO toxicity scale based on the upper limits of normal (ULN) ALT levels,Citation35 that is normal or grade 1 (<2.5 × ULN); mild - moderate elevation or grade 2 (2.5–5 × ULN); severe elevation or grade 3 (>5 × ULN) or grade 4 (>10 × ULN). The normal limits of ALT levels were considered to be 0–40 IU/L.Citation34,Citation44,Citation45
2.4 Ethics
The study was approved by the University of Namibia (UNAM), the Ministry of Health and Social Services (MoHSS) and Namibia Institute of Pathology (NIP) research and ethics committees. The need for informed consent was waved by the research committee as the study was based on patient records with no direct contact with patients. Patient codes or serial numbers were used instead of patient identifiers such as names to delink the patients from the data collected. All collected data was safely stored.
3 Results
A total of 79 patient records that met the eligibility criteria were included in the study. 44 patients were excluded as their records did not have ALT measurements at month 3 or month 6.
3.1 Baseline demographic and clinical characteristics
The majority of the study subjects were female (n = 51 (65%), p = 0.01) aged between 30 and 40 years (n = 41 (52%), p = 0.000); were not married (76%), (p = 0.000) and did not consume alcohol (n = 61(78%); p = 0.149). The majority of the subjects were initiated on a NVP based regimen (n = 53 (82%), p = 0.000); were WHO clinical state 1 or 2 (n = 59 (85%), p = 0.000) with a CD4 count of <350 cells/mm3 (n = 69 (89.6%), p = 0.000); did not have TB co-infection (n = 72 (98%), p = 0.000) and had an ART adherence level of >90% (n = 64(92%), p = 0.000) ().
Table 1 Baseline demographic and clinical characteristics of the study subjects (n = 79).
3.2 Patterns of alanine amino transaminase (ALT) elevation among study subjects
The analysis of variance (ANOVA) of the mean ALT levels among study subjects at baseline, month 3 and month 6 after the initiation of first line, ART was statistically significant (F (3, 76) = 6.4, p = 0.002, η2 = 0.193) ().
Table 2 Patterns of biomarkers for HAART efficacy and toxicity among the subjects.
This suggests evidence to conclude there is a difference between the ALT levels by initiation and duration of ART treatment with an appreciable effect size (η2 > 0.14). A post hoc comparison to evaluate pair wise difference between the mean ALT levels at baseline, month 3 and month 6, using the Bonferroni test to control for type I error, showed a significant increase in the mean ALT levels between baseline and month three (p = 0.001) as well as baseline and month six after the initiation of ART (p = 0.02). The ALT levels were higher at month three and month 6 compared to baseline ().
Table 3 Pair wise comparison of ALT levels at base line, month 3 and month 6.
3.3 Prevalence of grades of ALT elevation among the study subjects
Out of the 79 patients at baseline, 77 (97.5%) and 2 (2.5%) had grade 1 and grade 2 ALT elevation respectively. At 3 months post ART initiation, out of the 72 (91.1%) patients who had their ALT results recorded; 67 (93.1%) had grade 1, 4 (5.6%) had grade 2 and 1 (1.34%) had grade 3 ALT elevation. At 6 months post ART initiation, out of the 66 (83.5%) patients who had their ALT determined; 62 (93.9%) had grade 1 and 4 (6.1%) had grade 2 ALT elevation. Out of the five 5 (6.9%) patients that developed grade 2 or 3 ALT elevation by month 3 post ART initiation, the majority were taking a NVP based regimen, had a baseline CD4 count <350 cells/mm3, were of the female gender, were aged more than 40 years and were classified by WHO HIV clinical stage I (). The study also found that the initiation of ART significantly increased mean CD4 counts, level of haemoglobin and the patient’s body weight. The first ART regimen was associated with an increase in the mean serum creatinine levels also increased after the initiation of ART (; ).
Fig. 3 Grades of ALT elevations by CD4 counts after 3 months of ART initiation.
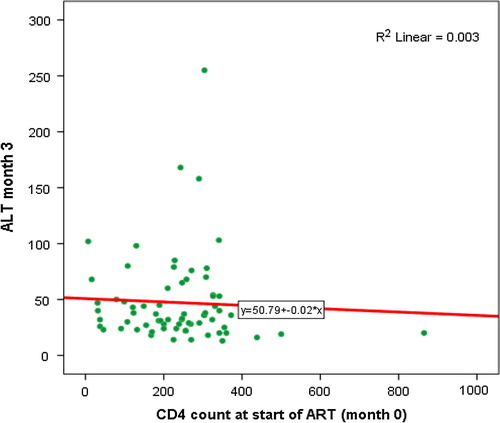
Table 4 Factors associated with elevation of ALT at month 3 (n = 5).
There were a higher number of female patients with normal – grade 1 and 2 - as well as with severe liver enzyme elevation (). The elevation in ALT at 3 months was associated with the baseline ALT levels () and CD4 count. The elevation in ALT was negatively correlated with the baseline CD4 counts ().
Fig. 1 Grades of ALT elevations by sex of patient after 3 months of ART initiation.
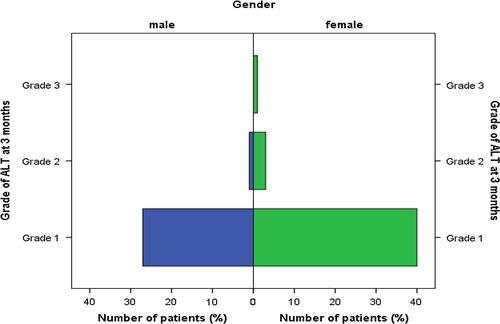
Fig. 2 Grades of ALT elevations by sex of patient after 3 months of ART initiation.

4 Discussion
We found that first line ART regimens were associated with significant elevation of ALT from baseline to 3 months, with ALT levels normalized by the months 6 of therapy. These findings concur with studies by Lucien et al., Uberti-Foppa, Teklay et al. and De Maat et al. who found an increased ALT elevation following ART with in the first month of treatment.Citation7,Citation11,Citation22,Citation35 Studies have associated NNRTI based regimens with early onset of ALT elevations.Citation16,Citation39,Citation45 However our findings differ from studies by Lucien et al., Splenger et al., and Bossi et al., regarding the patterns of the ALT elevation, which showed long term elevation of ALT with duration of treatment.Citation6,Citation11,Citation17 These studies, unlike our study, evaluated regimens with thymidine analogues (AZT or d4T) that have been associated with long term mitochondrial toxicity related liver damage.Citation39 This is unlike this study where adenosine analogue (TDF) based regimens were used, and have been referred to as safe to the liver.Citation8 TDF regimens were used as currently the recommended first line ART regimen in Namibia is TDF/lamivudine (3TC)/Nevirapine (NVP) or Efavirenz (EFV).Citation29
We also found a low incidence of moderate or grade 2 ALT elevation in 4 patients (5.6%) and severe or grade 3 elevation in only 1 patient (1.39%) who had ALT elevation at 3 months of ART initiation. Studies in Ethiopia, Zambia, and Palmon et al. also showed mild liver enzyme elevation in patients initiated on TDF based regimens.Citation7,Citation9,Citation23 However these findings differ from those of Martinez et al., Sulkowsky, Verucchi et al., Tetrault et al. and Manfredi et al., whose incidence of severe ALT elevation were 8% and 17.5% for EFV and NVP respectively.Citation18,Citation24,Citation25,Citation46,Citation47 A study in Cameroon by Lucien et al. found 22.67% (34/150) presented with transaminitis with respect to ALT,Citation11, with a study undertaken in the US among 352 subjects found 81 subjects developed elevated liver enzymes over the 96 week follow up period.Citation19 In this US study, the cumulative incidence of liver enzyme elevation was 5.7% at month 1, 9.2% at month 2, 11.5% at month 3, 17.3% at month 6 and 19% at month 9.Citation19 A slightly higher rate of efavirenz associated hepatotoxicity (12.5%) was observed in a prospective cohort study by Maggiolo et al. and Shubber et al.Citation12,Citation14 Whilst not statistically significant, our study found that grade 2 (moderate) and or grade 3 (severe) ALT enzyme elevations were associated with the use of NVP based regimens, initiation of ART in patients in the WHO Clinical Stage I, and older than 40 years. This was similar to the findings of Lucien et al., Spengler et al., and Hawkins et al., where ALT elevations were greater in patients >40 years, females and having a CD4 count of less than 350 cells.Citation6,Citation11,Citation48 Previous studies have associated liver damage with the NVP based regimensCitation20,Citation22–Citation25 and the female sex.Citation16 The higher incidence may parallel the higher enrollment of female patients on ART programmes in African countries.Citation15,Citation26–Citation29 Contrary to findings of this study (), liver toxicity of NVP base ART regimens has been associated with higher CD4 counts of >250 in female patients and >400 cell m3 in male patients.Citation45 This may be because these studies have traditionally been undertaken among Western countries with different patient populations and pharmacogenomics.Citation26
We accept that the main limitation of this study is the retrospective design – with a number of patients missing complete records on their ALT measurements; consequently, they were excluded. A prospective randomized clinical trial is ideal but may not be realistic in settings with limited resources. This is consistent with the fact that most studies in the African setting on ART induced liver damage have used retrospective data.Citation5,Citation11 However, we controlled for bias with paired samples in our study design. In addition, we were also aware that this study was undertaken in only one center in Namibia. Never-the-less we believe in view of the fact that we had 79 patients with paired ALT measurements (3 × 79 tests) for 3 months, and ANOVA analysis indicated significant differences at different treatment time points, that our findings are robust and would not have been different if we had included additional patients or additional centers in Namibia.
5 Conclusion
First line ART regimens commonly induce mild self-limiting liver enzyme elevation in Namibian HIV patients especially in the first 3 months of therapy. However, the incidence of moderate to severe first line ART induced liver toxicity is low. Patients of the female gender, aged over 40 years with a CD4 count of <350 and the use of NVP based regimens may be at greater risk of developing moderate to severe liver damage. Consequently, there is a need to monitor ALT levels for at least the first three months after initiation of therapy mainly in female patients, patients with grade >2 ALT elevations at baseline and patients with low CD4 counts, as well as patients on co-medication for tuberculosis.
In view of this, a different approach to monitoring liver toxicity may be warranted and should be incorporated in guidelines to monitor ART toxicity. This approach should be based on clinical signs and symptoms for hepatocellular injury such as jaundice as well as asymptomatic elevations in ALT at baseline and three months for all patients initiated on ART. We believe based on our findings that patients with high risk of hepatocellular damage such as low baseline CD4 count, of female sex, and >grade 2 ALT elevations, and patients who test positive for HBV/HCV, should be monitored for at least 6 months after initiation of NVP and EFV based antiretroviral therapy. The Ministry of Health in Namibia has started to implement these practices, and we will be monitoring the results in future research projects. These findings may also be of interest to other African countries.
Conflict of interest and funding
The authors hereby declare that they have no conflicts of interest to disclose. There was no external funding for this project.
Acknowledgements
The authors would like to acknowledge the contribution from the National Institute of Pathology of Namibia for the permission to use their data to conduct this study and the staff of the MoHSS ART clinic of Katutura State Hospital and the MoHSS for allowing us to undertake this research.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 13 April 2017
References
- UNAIDS. Report on the Global AIDS Epidemics. Ps 16-29. <http://www.unaids.org/documents/20101123_globalreport_em.pdf>; 2010.
- UNAIDS. Namibia Report on AIDS Epidemics update. <http://www.unaids.org/en/resources/documents/2014/20140716_UNAIDS_epidermiologydata>; 2013.
- Republic of Namibia, Ministry of Health and Social Services. Directorate of special programmes Surveillance report of the 2014 national HIV sentinel survey. <http://www.mhss.gov.na/files/downloads/12f_2014%20National%20HIV%20Sentinel%20Survey.pdf>; 2014.
- Global HIV/AIDS response progress report 2014. UNICEF, UNAIDS. <http://www.unaids.org/sites/default/files/media_asset/GARPR_2014_guidelines_en_0.pdf>.
- Mwamakimbula NWR, Prevalence and severity of adverse drug reactions among adult patients using default first line and modified antiretroviral combinations in Mbeya region, Tanzania. <http://ihi.eprints.org/1627/1/William_Ndimbumi_Mwamakimbula_Reuben.pdf>; 2012.
- U.SpenglerM.LichterfeldJ.K.RockstrohAntiretroviral drug toxicity – a challenge for the hepatologist?J Hepatol3622002283294
- G.TeklayB.LegesseM.LegesseAdverse effects and regimen switch among patients on antiretroviral treatment in a resource limited setting in EthiopiaJ Pharmacovigilance120134
- I.CassettiJ.V.MadrugaJ.M.SuleimanThe safety and efficacy of Tenofovir DF in combination with lamivudine and Efavirenz through 6 years in antiretroviral-naive HIV-1-infected patientsHIV Clin Trials82007164172
- B.H.ChiA.MwangoM.GigantiEarly clinical and programmatic outcomes with Tenofovir-based antiretroviral therapy in ZambiaJ Acquired Immune Deficiency Syndrome5420106370
- B.WoldemedhinN.T.WabeThe reason for regimen change among HIV/AIDS patients initiated on first line highly active antiretroviral therapy in southern EthiopiaN Am J Med Sci420121923
- K.F.H.LucienA.N.J.ClementN.P.FonP.WeledjiC.P.NdikvuThe effects of antiretroviral treatment on liver function enzymes among HIV-Infected out-patients attending the central hospital of Yaounde, CameroonAfr J Clin Exp Microbiol113201015951689
- Z.ShubberAdverse events associated with Nevirapine and Efavirenz-based first-line antiretroviral therapy: a systematic review and meta-analysisAIDS27201314031412
- N.KontorinosD.DieterichHepatotoxicity of antiretroviral therapyAIDS Rev5120033643
- F.MaggioloC.AriciM.AiroldiReasons for discontinuation of Nevirapine containing HAARTJ Antimicrob Chemother592007569572
- F.KalemeeraC.MbangoM.MubitaE.NaikakuR.GaidaB.GodmanEffect of changing from first- to second-line antiretroviral therapy on renal function: a retrospective study based on data from a single health facility in NamibiaExp Rev Anti-infective Ther1482016777783
- S.WakibiZ.Ng'ang'aG.MbuguaFactors associated with non-adherence to highly active antiretroviral therapy in Nairobi, KenyaAIDS Res Ther58201143
- P.BossiD.ColinF.BricaireE.CaumesHypersensitivity syndrome associated with efavirenz therapyClin Infectious Diseases302000227228
- E.MartinezJ.L.BlancoA.ArnaizHepatotoxicity in HIV-1–infected patients receiving Nevirapine-containing antiretroviral therapyAcquired Immune Deficiency Syndrome15200112611268
- I.OfotokunS.E.SmithsonC.LuK.A.EasleyJ.L.LennoxLiver enzymes elevation and immune reconstitution among treatment-naïve HIV-infected patients instituting antiretroviral therapyAm J Med Sci33452007334341
- I.SabolicA.R.AsifW.E.BudachC.WankeA.BahnG.BurckhardtGender differences in kidney functionPflugers Archiv45532007397429
- Barlett J. Severe liver toxicity in patients receiving two nucleoside analogues and a non-nucleoside reverse transcriptase inhibitor. 8th Conference on Retroviruses & Opportunistic Infections. Chicago, IL. 2001; Abstract 19.
- M.M.De MaatR.ter HeineE.C.Van GorpCase series of acute hepatitis in a non-selected group of HIV-infected patients on nevirapine-containing antiretroviral treatmentAIDS1715200322092214
- R.PalmonB.C.KooD.A.ShoulzLack of hepatotoxicity associated with non-nucleoside reverse transcriptase inhibitorsJ Acquired Immune Deficiency Syndrome292002340345
- M.S.SulkowskyD.L.ThomasS.H.MehtaHepatotoxicity associated with nevirapine- or efavirenz-containing antiretroviral therapy: role of hepatitis C and B infectionsJ Hepatol352002182189
- G.VerucchiIncidence of liver toxicity in HIV infected patients receiving isolated dual nucleoside analogue antiretroviral therapyJ Acquired Immune Deficiency Syndrome332003546548
- R.GaidaI.TruterC.GroblerT.KotzeB.GodmanA review of trials investigating efavirenz-induced neuropsychiatric side effects and the implicationsExp Rev Anti-infective Ther1442016377388
- Republic of Namibia, Ministry of Health and Social Services Directorate of Special Programmes. National Guidelines for Antiretroviral Therapy First Edition; 2003.
- Republic of Namibia, Ministry of Health and Social Services Directorate of Special Programmes. National Guidelines for Antiretroviral Therapy second Edition; 2010.
- Republic of Namibia, Ministry of Health and Social Services Directorate of Special Programmes. National Guidelines for Antiretroviral Therapy Fourth Edition; 2014.
- Ministry of health and Social Services (MoHSS), National Tuberculosis and leprosy Control Program 2009/2010 Annual Report, Windhoek MoSS.
- World Health Organization. Global Status Report on Alcohol. <http://www.who.int/substance_abuse/publications/global_status_report_2004_overview.pdf>; 2004.
- Veira DEO, Gomes M. Adverse effects of tuberculosis treatment: experience at an outpatient clinic of a teaching hospital in the city of São Paulo, Brazil. J Bras Pneumol 2008; 34. <http://www.scielo.br/pdf/jbpneu/v34n12/en_v34n12a10.pdf>.
- M.JavariG.ShalviriGholamiJ.SalamzadehG.MaghooliMirsaeediAdverse reactions of anti-tuberculosis drugs in hospitalized patientsPDS1610200711041110
- WHO Toxicity Grading Scale for Determining. The Severity of Adverse Events. <http://www.icssc.org/Documents/Resources/AEManual2003Appendices>; 2003.
- C.Uberti-FoppaA.De BonaL.GaliLiver fibrosis in HIV-positive patients with hepatitis C virus: role of persistently normal alanine aminotransferase levelsJ Acquired Immune Deficiency Syndrome4120066367
- Carter M. ALT levels may not give true picture of liver disease in HIV/HCV co-infected, suggests study. <http://www.aidsmap.com/ALT-levels-may-not-give-true-picture-of-liver-disease-in-HIVHCV-coinfected-suggests-study/page/1422831/>; 2006.
- S.BoseA.VaranasiG.MoDemographic, socio-economic and psychological determinants of HIV treatment: a community out-patient experienceBJMP2220094245
- M.J.NunezMartin-CarboneroV.MorenoE.ValenciaJ.Garcia-SamaniegoJ.Gonzalez-CastilloImpact of antiretroviralAIDS222006825829
- J.H.LewisThe rational use of potentially hepatotoxic medications in patients with underlying liver diseaseInforma Healthcare12002159172
- Aronson JK, Torpey K, Lartey M. Side effects of drugs annual 2011; 33: 577–88. <http://https://www.elsevier.com/books/book-series/side-effects-of-drugs-annual_>.
- A.BonjochHigh rate of reversibility of renal damage in a cohort of HIV-infected patients receiving Tenofovir-containing antiretroviral therapyAntiviral Res9620126569
- R.D.MooreAnaemia and human immunodeficiency virus disease in the era of highly active antiretroviral therapySemin Hematol720001823
- C.NjugunaC.OrrellR.KaplanL.G.BekkerR.WoodS.D.LawnRates of switching antiretroviral drugs in a primary care service in South Africa before and after introduction of tenofovirPLOS One852013e63596
- Bimenya GS. International system of units in clinical sciences: reference values for analytes in clinical chemistry, vol. 44, 1st ed., Kampala; 2000.
- G.N.LoanouE.J.BoykoS.P.LeeThe prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999–2002Am J Gastroenterol10120067682
- J.M.TetraultJ.P.TateK.A.McGinnisVeterans Aging Cohort Study Team. Hepatic safety and antiretroviral effectiveness in HIV-infected patients receiving naltrexoneAlcohol Clin Exp Res3622012318324
- R.ManfrediL.CalzaRecent availability of two novel, fixed formulations of antiretroviral nucleoside analogues: a 12-month prospective, open-label survey of their practical use and therapeutic perspectives in antiretroviral-naive and -experienced patientsAIDS Patient Care STDs222008279290
- C.HawkinsC.AchenbachW.FrydaD.NgareR.MurphyAntiretroviral durability and tolerability in HIV-infected adults living in urban KenyaJAIDS4532007304310
Appendix A Data abstraction tool
A.1 Data entry tool
First-line antiretroviral therapy induced liver enzyme elevation in a cohort of HIV/AIDS patients in Namibia: findings and implications