
Abstract
Objectives: hepatic fibrosis occurs due to chronic liver injury. Early fibrosis can be reversed by treatment with specific antifibrotic therapy in addition to removal of the cause if possible, that is why, identification of the early liver fibrosis is important. MRI DWI is a non-invasive non-contrast imaging technique which help in diagnosis of different stages of hepatic fibrosis. Aim of the work: was to study the predictive value of diffusion weighted MRI for assessing liver fibrosis in comparison to liver biopsy in chronic hepatitis C virus patients. Methods: all the studied cases were subjected to the followings: (1) History and laboratory examination (PCR for HCV and liver function tests). (2) MRI DWI and post processing ADC map. (3) Percutaneous liver biopsy in cases with HCV for histopathological examination to assess the stage of fibrosis. Results: this study was carried out on 75 subjects, divided into two group, 50 cases and 25 controls, the mean age in the two studied groups was 36.5 ± 9.32 and 35.8 ± 6.75 respectively in patients and control. ADC of both liver and spleen showed a highly significant increase in the control than in the cases with mean liver ADC in the control group = 2.3 ± 0.25. There was a significant negative correlation between the mean ADC of the liver, spleen and the stage of liver fibrosis.
1 Introduction
Hepatic fibrosis occurs due to chronic liver injury that usually leads to collapse of hepatic lobules, formation of fibrous septae and hepatocyte regeneration with nodule formation.Citation1 Extracellular matrix components accumulate in the liver as a result of imbalances in their production, deposition and degradation.Citation2 At the end, this process will progress to cirrhosis, portal hypertension, hepatocellular failure and hepatocellular carcinoma in some patients.Citation3
There are multiple causes for chronic liver injury,Citation4,Citation5 in Egypt, hepatitis C virus (HCV) genotype 4 infection is the most common cause. Egypt has the highest prevalence of HCV in the world, estimated nationally at 14.7%.Citation6,Citation7
Early fibrosis can be reversed by treatment with specific antifibrotic therapy in addition to removal of the cause if possible, that is why, identification of the early liver fibrosis is important.Citation2,Citation8,Citation9
Liver biopsy (LB) is the gold standard and the reference method for determining histological grading (the extent of necroinflammatory activity) and staging (the extent of fibrosis) to assess the current status of the liver, to provide prognostic information for future disease progression and treatment decisions as it may reveal advanced fibrosis or cirrhosis that necessitates surveillance for HCC and screening for esophageal varices.Citation10,Citation11 However, liver biopsy is invasive, painful and limited by intra-and inter-observer variation and sampling errors, moreover, it can be complicated by hemorrhage, pneumothorax, peritonitis, penetration of abdominal organs and death.Citation12–Citation14 Therefore, reliable and noninvasive methods for assessment and quantification of hepatic fibrosis are needed. There are different noninvasive methods that have been developed for assessment of fibrosis as an alternative to the LB.Citation15 These methods are based on clinical, biochemical, and radiologic variables that can be used in combination.Citation16 If noninvasive methods provide a clear-cut assessment of hepatic fibrosis then further assessment with liver biopsy may not be needed, but questions remain regarding the cut-off values for the degree of fibrosis, cost, and validity of these tests, which should be answered through performing multiple studies.Citation16,Citation17
Noninvasive serum markers can be good clinical alternatives in patients who are not candidates for liver biopsy, they can predict presence or absence of significant fibrosis/cirrhosis, but are not useful in differentiating between intermediate stages of fibrosis. FibroSure, FibroTest-ActiTest and FIBROSpect are examples of these markers.Citation17–Citation19
Radiologic imaging has been used to estimate fibrosis. Ultrasound transient elastography is an example, which shows promising results in identifying stages of liver fibrosis, but its results are influenced by multiple factors such as obesity, hepatic inflammation and ascites. Thus, it is better to combine transient elastography results with other measures of hepatic fibrosis.Citation20,Citation21
Both CT and conventional MRI did not show high sensitivity for early stages of fibrosis, However, diffusion-weighted magnetic resonance imaging (DW-MRI) has been shown better results in diagnosing early fibrosis.Citation22
DWI-MRI is a technique in which water diffusion is quantified by the calculation of the apparent diffusion coefficient (ADC) because DWI-MRI is sensitive to the microscopic movement of water molecules.Citation22,Citation23
DWI-MRI has many advantages, it is rapid, non-invasive and non-contrast imaging technique, but MR diffusion quantifications can be affected by some factors such as permeability, perfusion and cellular structure. In patients with chronic liver disease, ADC values are lower which may be explained by the deposition of proteoglycan and glycosaminoglycan fibers in the liver with subsequent restriction of the diffusion of water molecules.Citation23–Citation25
2 Aim of the work
Was to study the predictive value of diffusion weighted MRI for assessing liver fibrosis in comparison to liver biopsy in chronic hepatitis C virus patients.
2.1 Subjects and methods
This study was conducted on 75 subjects, divided into two groups, 50 cases with chronic viral hepatitis C and 25 age and sex matched healthy subjects with no evidence of liver disease. These cases were referred from hepatobiliary and tropical medicine units to radiology department for DWI-MRI in the duration between June 2013 till June 2014.
The exclusion criteria were: hepatitis B virus (HBV) infection, alcohol consumption, obesity, concomitant schistosomiasis, bleeding diathesis, hepatic decompensation, chronic diseases such as diabetes mellitus or connective tissue diseases, malignancies, previous anti-viral or systemic anti-cancer therapy. Also absolute contraindication to MRI or refusing MRI imaging were considered.
The study protocol was approved by the Research Review Committee of the Alexandria Faculty of Medicine and was conformed to the 1975 Declaration of Helsinki. An informed consent was obtained from each subject included in the study.
All the studied cases were subjected to the followings:
| (1) | History and laboratory examination (PCR for HCV and liver function tests). | ||||
| (2) | MRI DWI and post processing ADC map. | ||||
| (3) | Percutaneous liver biopsy in cases with HCV for histopathological examination to assess the stage of fibrosis. | ||||
2.2 MRI examination
It was done for all patients one day before or at the same day of liver biopsy procedure but before it to avoid false results from bleeding that affects the DWI/ADC. The examination was done on 1.5T superconducting magnet MRI machines Philips Gyroscan Intera version 12.1.1.2 (Best, The Netherlands). The patient was placed in supine position; arms extended above head. A phased array surface coil was used.
DWI with b value 500 s/mm2 with TR 1000, TE 137, flip angle 90, FOV 370, slice thickness 7 mm and automatically computer-generated ADC map.
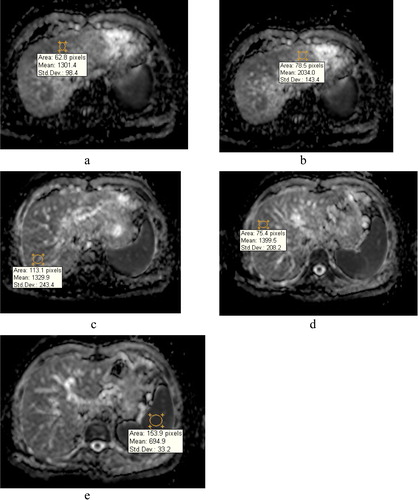
DWI was interpreted in correlation with ADC map and ADC value was calculated in ×10−3 mm2/s using dedicated workstation. Four ROIs for ADC values were measured for each case, two ROIs away from the blood vessels in each lobe of the liver with each ROI = 1–1.5 cm2. The final ADC value was the average of the four ROIs.
Normalized ADC was calculated as ratio between the mean ADC of the liver and that of the spleen .
Fig. 1 ADC map demonstrates measurements of ADC value of the liver and that of the spleen.
2.3 Liver biopsy
All patients were subjected to pretreatment liver biopsy as routine prerequisites for antiviral therapy to evaluate the degree of activity for chronic hepatitis (grading), and the presence or absence of fibrosis (staging) according to METAVIR scoring system.Citation26,Citation27 The histopathological findings were correlated with DW-MRI.
2.4 Procedure of the liver biopsyCitation28,Citation29
It was done as an inpatient procedure (only for 6 h of admission) in the ultrasound room in Hepatobiliary Unit, Department of internal medicine and Department of tropical medicine at Alexandria Main University Hospital.
| 1. | Examination of blood coagulation profile (platelet count, prothrombin activity). | ||||
| 2. | Informed consent was obtained in writing on the same day of the planned biopsy. | ||||
| 3. | Ultrasound-guided transcutaneous liver biopsy was done via an intercostal route using automatic Tru-Cut needle (“biopsy gun”) 16 gauge in diameter and 20 cm length with the patient positioned left lateral with the right arm elevated behind the head. | ||||
2.5 Sample size
Sample size was calculated based on a previous study by using Med Calc statistical software. Assuming area under ROC to be 0.80, an alpha of 0.05 and power of study 80.0%. A minimum sample size required was 50 patients and 25 control will be required for this study.
2.6 Statistical analysis
The Data was collected and entered into the personal computer. Statistical analysis was done using Statistical Package for Social Sciences (SPSS/version 20) software.
Arithmetic mean, standard deviation, for categorized parameters, chai square test was used, while for numerical data, t-test was used to compare two groups while for more than two groups ANOVA test was used. To find the association between two variables, Spearman correlation coefficient test was used and the level of significance was 0.05.
3 Results
This study was carried out on 75 subjects, divided into two group, 50 cases and 25 control, the mean age in the two studied groups was 36.5 ± 9.32 and 35.8 ± 6.75 respectively in patients and control, there was no significant difference between the two groups regarding age (p > 0.05), the male to female ratio in the two groups was matched, the BMI in patients was 24.59 ± 2.58 and in control was 23.55 ± 2.57, on comparing the two groups it was found that there was no significant difference regarding BMI ().
Table 1 Characteristic features of the studied groups.
Regarding the laboratory findings, it was found that there was a slightly significant increase in RBCs in patients more than the control, the Platelet count in patients was significantly lower than in the control group (P < 0.01), the Hb level and WBCs showed no significant difference between patients and control. Fasting blood glucose in the two groups was within normal without significant difference while there was a slightly increase in 2 h post prandial blood sugar in patients than in the control. Blood urea showed a significant increase in patients than in the control, while the creatinine showed insignificant difference between patients and control. Serum cholesterol and triglyceride showed a significant difference between patients and control. TSH, Free T3 showed a significant increase in patients than the control, but free T4 was matched in the two groups. Liver enzymes showed a significant increase in patients than the control. Serum bilirubin, Prothrombin activity (PA) and alfa fetoprotein (AFP) showed no significant difference in the two groups ().
Table 2 Comparison between the two studied groups regarding the laboratory and DWI findings.
The study included 9 patients with F0, 16 patients with F1, 7 patients with F2, 15 patients with F3 and 3 patients with F4 .
Table 3 Results of liver biopsy of the studied patients.
ADC of both liver and spleen showed a highly significant increase in the control than in the cases with mean liver ADC in the control group = 2.3 ± 0.25.
The relation between the stage of liver fibrosis and mean ADC of the liver and spleen was shown in ; there was a significant negative correlation between the mean ADC of the liver, spleen and the stage of liver fibrosis.
Table 4 Relation between mean ADC (liver) and ADC (spleen) and stage of liver fibrosis.
The ROC curve was done to calculate the cut off value of ADC of the liver and the mean normalized ADC to detect the stage of liver fibrosis. In the detection of stage 3 as a base line, mean ADC of the liver and cut off value was 1.15, the area under the curve was 0.89 with sensitivity of 86% and 85%, and specificity was 90% and 90% respectively. Regarding mean normalized ADC the area under the curve was 0.52 and the cut off value was 0.52 to detect the stage less or more than 2, the sensitivity was 61% and 60% and the specificity was 60.3% and 55% (, ).
Fig. 2 ROC curve and the cut off value of both mean ADC liver and normalized ADC in detecting the stage of liver fibrosis.
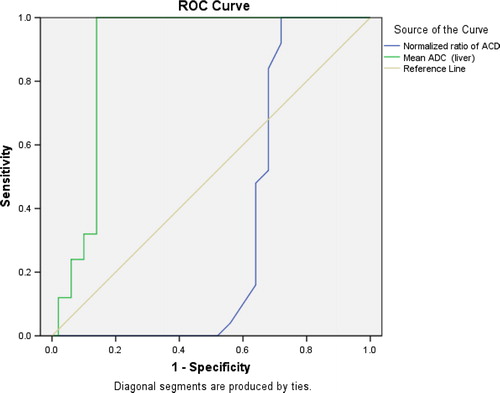
Table 5 The cut off value of both mean ADC liver and normalized ADC in detecting the stage of fibrosis.
The pearson correlation coefficient between different studied makers showed that there was a positive significant correlation between AFP and mean ADC of the liver, and there was a significant positive correlation between mean ADC of the liver and spleen ().
Table 6 Correlation between different parameters of the studied patients.
4 Discussion
Liver biopsy gives a snapshot and not an insight into the natural history of liver fibrosis and the dynamic changes during the process of fibrogenesis whether progression, static or regression as it needs repeated biopsies through the course of the disease which is not applicable in clinical field. At the same time, liver biopsy is an invasive procedure, carrying a risk of rare but potentially life-threatening complications Citation10,Citation12; however after recent development in MRI, there are different techniques that can be used to assess the fibrosis with more or less high accuracy, and one of these techniques is DWI/ADC which is non- invasive reliable method.Citation22
The decrease in ADC value among patients with liver fibrosis is attributed to accumulation of glycosaminoglycane, proteoglycane and collagen fibers within the liver and consequently restricted diffusion of water molecules.Citation30
Kumaresan et al., Richard et al., Hasan et al.Citation23,Citation31,Citation32 concluded that the ADC value in fibrotic liver is significantly lower than that of normal liver, in our cases, we confirmed that as we detected high ADC value of the liver among control group.
In our study we found that there is significant negative correlation between the stage of liver fibrosis and ADC value of the liver, this was also confirmed in different studies.Citation30,Citation32,Citation33
The cut off value, in the current study, of the liver ADC in stage 3 or less is 1.15 with sensitivity and specificity of 86% & 90% respectively. This was concluded in other studies as they found the best cut off value of hepatic ADC to detect higher stage of fibrosis at high b values is 1.3 with 89% sensitivity and 88% specificity.Citation22,Citation23
In other study, they found variable measurements of liver ADC with mean ADC in mild fibrosis = 0.97 while in advanced fibrosis = 0.78.Citation32
The variation in ADC values among fibrotic liver in different studies may be attributed to different machines that have been used together with variation in b values used in DWI/ADC.
We used the normalized ADC value which is the ADC of the liver/that of the spleen as another measurement method to confirm the relation between DWI/ADC and stage of liver fibrosis and this was in agreement with Mona El-Hariri, et al.Citation25
In the current study there was a significant relation between the normalized ADC of the liver and the stage of liver fibrosis with AUC = 0.52 and cut off value for stage 3 was 0.52 with a sensitivity and specificity = 61% & 60% respectively. Richard et al.Citation31 also confirmed this in their study as they found the normalized liver ADC distinguished between individual groups of fibrosis with significant differences between control subjects and intermediate stages of fibrosis (stages 2 and 3).
Although DWI-MRI proved to be useful in differentiating different stages of liver fibrosis, in our study, we found overlap between stages F0, F1 and F2 which is in agreement with Kumaresan et al.Citation23 and Hasan et al.Citation32 confirmed that in their study, and so DWI/ADC of the liver can divide the patients into two main groups <F3 and >F3, yet this overlap does not affect the treatment regimen.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 9 October 2017
References
- A.M.ElsharkawyF.OakleyD.A.MannThe role and regulation of hepatic stellate cell apoptosis in reversal of liver fibrosisApoptosis102005927939
- Wen-CeZhouQuan-BaoZhangLiangQiaoPathogenesis of liver cirrhosisWorld J Gastroenterol20201473127324
- L.FerrellLiver pathology: cirrhosis, hepatitis, and primary liver tumors. Update and diagnostic problemsMod Pathol132000679704
- S.NaveauG.PerlemuterA.BalianEpidemiology and natural history of cirrhosisRev Prat55200515271532
- A.M.Di BisceglieNatural history of hepatitis C: its impact on clinical managementHepatology31200010141018
- W.SievertI.AltraifH.A.RazaviA.AbdoE.A.AhmedA systematic review of hepatitis C virus epidemiology in Asia, Australia and EgyptLiver Int3120116180
- Y.A.MohamoudG.R.MumtazS.RiomeD.MillerL.J.Abu-RaddadThe epidemiology of hepatitis C virus in Egypt: a systematic review and data synthesisBMC Inf Dis132013288
- V.Hernandez-GeaS.L.FriedmanPathogenesis of liver fibrosisAnnu Rev Pathol: Mech Dis62011425456
- P.MarcellinT.AsselahN.BoyerFibrosis and disease progression in hepatitis CHepatology3620024756
- A.A.BravoS.G.ShethS.ChopraLiver biopsyN Engl J Med3442001495500
- L.JulesM.D.DienstagThe role of liver biopsy in chronic hepatitis CHepatology362002152160
- F.PiccininoE.SagnelliG.PasqualeComplications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsiesJ Hepatol21986165173
- A.RegevM.BerhoL.J.JeffersSampling error and intraobserver variation in liver biopsy in patients with chronic HCV infectionAm J Gastroenterol97200226142618
- C.H.JanesK.D.LindorOutcome of patients hospitalized for complications after outpatient liver biopsyAnn Intern Med11819939698
- L.CastéraJ.VergniolJ.FoucherB.Le BailE.ChanteloupProspective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis CGastroenterology1282005343350
- L.CasteraM.PinzaniNon-invasive assessment of liver fibrosis: are we ready?The Lancet375201014191420
- M.StellaGonzalloCrespoMiquelNaversaXavierFornsNoninvasive assessment of liver fibrosisHepatology532011325335
- T.P.EmailF.Imbert-BismutM.MunteanuOverview of the diagnostic value of biochemical markers of liver fibrosis (FibroTest, HCV FibroSure) and necrosis (ActiTest) in patients with chronic hepatitis CComp Hepatol320048
- P.CalesF.ObertiS.MichalakA novel panel of blood markers to assess the degree of liver fibrosisHepatology42200513731381
- L.CasteraX.FornsA.AlbertiNon-invasive evaluation of liver fibrosis using transient elastographyJ Hepatol482008835847
- M.Friedrich-RustK.WunderS.KrienerLiver fibrosis in viral hepatitis: noninvasive assessment with acoustic radiation force impulse imaging versus transient elastographyRadiology2522009
- H.R.IbrahimA.A.EL-HamidA.TohamyM.R.HabbDiagnostic value of apparent diffusion coefficient calculated with diffusion-weighted MRI for quantification of liver fibrosisEgypt J Radiol Nucl Med422011119131
- K.SandrasegaranF.AkisikC.LinValue of diffusion-weighted MRI for assessing liver fibrosis and cirrhosisAJR193200915561560
- AliyeSoyluÖzgürKılıçkesmezŞulePoturoğluUtility of diffusion-weighted MRI for assessing liver fibrosis in patients with chronic active hepatitisDiagn Interv Radiol162010204208
- M.El-HaririT.F.TahaH.I.HussienApparent diffusion coefficient (ADC) in liver fibrosis: usefulness of normalized ADC using the spleen as reference organEgypt J Radiol Nucl Med442013441451
- R.MacSweenV.DesmitT.RoskamsDevelopmental anatomy and normal structureR.MacSweenA.BurtB.PortmanK.IshakP.ScheuerP.AnthonyPathology of the liver4th ed.2002ChurchillLivingston166
- O.OkaforS.OjoA comparative analysis of six current histological classification schemes and scoring systems used in chronic hepatitis reportingRev Esp Pathol372004269277
- Patch D, Dhillon AP. Biopsy of the Liver. In: Dooley JS, LOK AS, Burroughs AK, Heathcote EJ, eds. Sherlock's Diseases of the Liver, 12th ed. UK: Blackwell Inc.; 2011:36–47.
- Kuntz E, Kuntz HD. Hepatology, Principles and Practice, 2nd ed. Germany: Springer Medizin Verlag; 2006: 142–149.
- B.TaouliM.ChouliA.MartinA.QayyumF.CoakleyV.VilgrainChronic hepatitis: role of diffusion-weighted imaging and diffusion tensor imaging for the diagnosis of liver fibrosis and inflammationJ Magn Reson Imag2820088995
- K.RichardC.HershF.ElyDiagnosis of liver Fibrosis and cirrhosis with diffusion weighted imaging: value of normalized apparent diffusion coefficient using the spleen as reference organAJR1952010671676
- C.HasanE.AbdulbasitY.SemaThe use of DWI to assess spleen and liver quantitative ADC changes in the detection of liver fibrosis stages in chronic viral hepatitisEur J Radiol822013307312
- T.BachirM.Tolia1S.JamesA.MichaelT.HillelDiffusion-weighted MRI for quantification of liver fibrosis: preliminary experienceAJR1892007799806