
Abstract
Introduction
The popliteus musclotendinous complex is considered to be one of the main stabilizers of the posterolateral corner of the knee having different attachments and variable sites of injuries, the use of MRI helps the radiologists to depict such injuries consistently.
Purpose of the study
To study the role of MRI in evaluating the popliteus musclotendinous injuries as a part of the PLCof the knee.
Patients and methods
Our study included 15 patients with trauma to the knee undergoing MRI using 1.5 T magnet using the following sequence: Axial, Coronal, sagittal proton density fat sat, T1, T2 and T2 gradient and conventional X-ray/CT [All patients did conventional X-ray Knee (AP and Lateral views), two patients did CT study of the knee].
Results
Out of 15 studied patients with PLC injuries, eight (53.33%) patients had popliteus complex injuries, 7 (87.5%) patients showed combined injuries with other posterolateral structures while one (12.5) patient had isolated popliteus musclotendinous complex injury.
Conclusion
MRI imaging is crucial in the evaluation of the different sites and patterns of injuries of the popliteus musclotendinous complex when suspecting PLC injury.
1 Introduction
1.1 Anatomy
As described in a three-layer approach, the popliteus musclotendinous complex is considered to be a layer three structure forming one of the main deep posterolateral stabilizers.Citation1
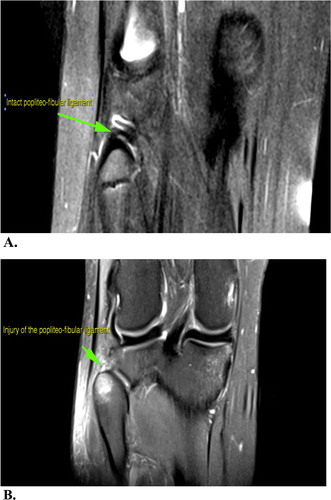
Fig. 5 Coronal PDFS (B) shows injury of the popliteofibular ligament at site of its insertion at the apex of the fibular head with associated marrow contusion at the fibular head in our case. Coronal PDFS (A) shows an intact popliteofibular in a normal individual for comparison.
The popliteus muscle forms part of the floor of the popliteal fossa. It is triangular in shape, thin and flat in dimensions and is broadly attached to the posterior aspect of the medial surface of the tibia just above the soleal line.Citation2
It then continues upwards and to the lateral, forming a tough and long tendon that enters through the popliteal opening into the knee joint.
The popliteus tendon passes below two structures, which are the lateral collateral ligament (LCL) and the tendon of the biceps femoris muscle. The tendon is then inserted at the outer side of the lateral condyle of the femur in a bony depression. This tendinous attachment is located anterior and inferior to the attachment of the lateral collateral ligament, which lies more proximally on the lateral femoral epicondyle ( and ).Citation3–Citation5
Fig. 1 Anatomic drawing of the popliteus musclotendinous unit origin and insertion. (a) Drawing of the posterior view of the knee shows the site of origin (blue) and site of tendon insertion (red) of the popliteus muscle. (b) Drawing of the lateral aspect of the lateral femoral condyle shows the relation of the lateral collateral ligament (white) as well as the lateral head of the gastrocnemius muscle (orange) to the tendinous attachments of the popliteus (red). (c) Drawing of the posterior aspect of the knee shows the lateral collateral ligament (arrowhead) and biceps femoris in relation to the popliteus muscle and tendon.Citation3–Citation5
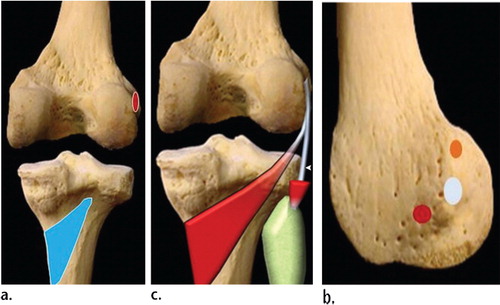
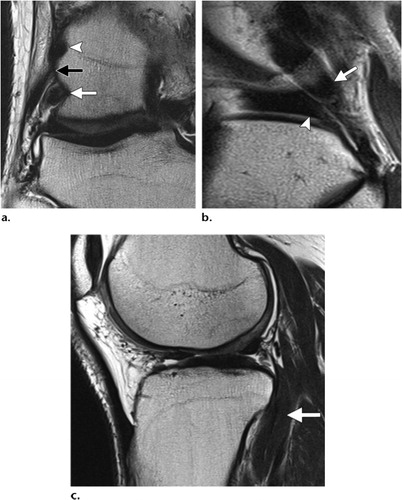
Fig. 2 MRI images of the appearance of popliteus muscle and course of its tendon: (a) Coronal T2-weighted image depicts popliteus tendon insertion (white arrow), the lateral collateral ligament at its femoral attachment (black arrow) as well as the lateral head of the gastrocnemius origin (arrowhead). (b) Sagittal T2-weighted image shows the popliteus tendon passing through the popliteal opening where the popliteus tendon (arrow) seen adjacent to the posterior horn of the lateral meniscus (arrowhead) with intervening synovial fluid. (c) Sagittal T2-weighted image shows the popliteus muscle passing underneath the arcuate ligament where the bulk of the popliteus muscle lies extra-articular (arrow).Citation11
Just behind the articular cartilage surface of the lateral femoral condyle, the tendinous attachment lies on a wide area relatively about (59 mm2) located at the anterior fifth of the popliteus sulcus. The site of insertion shows a consistent location about 18.5 mm anterior to the FCL insertion site.Citation6
It is obvious that the popliteus tendon has an intracapsular location, yet extra-articular and extrasynovial in character. As described by most authors, there are variations regarding the deep and superficial layers of the muscle, being more evident at the deep layers. It is found that the superficial fibers blend with the knee joint capsule.Citation4,Citation5,Citation7–Citation10
The popliteofibular ligament is seen consistently extending from the popliteus tendon close to the myotendinous junction of the popliteus musclotendinous complex reaching to the apex of the styloid process of the fibular head at its posterior aspect, such attachment lies exactly posterior and medial to the site of insertion of the biceps femoris tendon.Citation12,Citation13
This ligament is one of the toughest lateral stabilizing structures of the knee, unfortunately it isn’t easily recognized but variably visualized at MR imaging as a subtle structure in different sequencesCitation14,Citation15 as demonstrated in .Citation12,Citation13
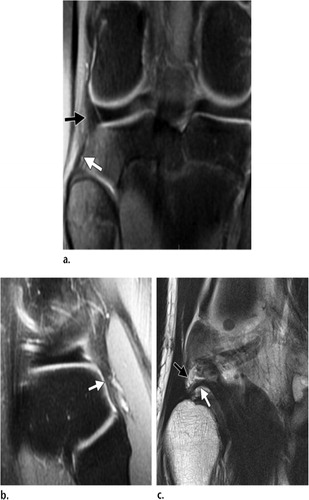
Fig. 3 MRI images of the popliteofibular ligament: (a) Coronal PD-weighted images with fat saturation show the extension of the popliteofibular ligament (white arrow) from the apex of the head of fibula upwards towards the popliteus muscle (black arrow). (b) Sagittal PD-weighted images with fat saturation shows the attachment of the popliteofibular ligament to the apex of the fibular head posteriorly. (c) Coronal T2-weighted image shows the lateral geniculate vessels (black arrow) and the popliteofibular ligament (white arrow) depicted beneath them.
1.2 Mechanism of injury
The mechanism of posterolateral injury is either 1. External rotation of the tibia or abrupt hyperextension of the knee, with concomitant direct varus force or 2. A hit to the anterior aspect of the medial surface of the tibia in an extended knee.Citation16–Citation18
1.3 MRI pattern of injuries
Ligamentous injuries
The ligamentous injuries are graded on MRI into three groupsCitation19:
GRADE 1 sprain: (minor sprain) high signal is seen superficial to an otherwise normal ligament.
GRADE 2 sprain: (severe sprain or partial tear) high signal is seen superficial to the ligament, with partial discontinuation of the ligament fibers.
GRADE 3 sprain: complete discontinuity and loss of integrity of the ligament.
Musclotendinous injuries
Myotendinous strains can be graded at MR imaging into three groupsCitation20:
GRADE 1/First-degree strain manifested as high signal with a feathery appearance on MR images indicating a minor degree of disruption of the injured fibers.Citation20,Citation21
GRADE 2/Second-degree strain manifested as partial tear with evident fibers discontinuity in a non-retracted muscle.Citation20,Citation21
GRADE 3 /Third-degree strain involves a complete rupture of the myotendinous structure with subsequent retraction and clamping of the involved muscle.Citation20,Citation21
A forceful, unbalanced and rather eccentric muscle contraction can result in an acute avulsive injury noticed at the tendon insertion site.Citation22 And it becomes manifested as periosteal stripping and hematoma on MR images noticed at the tendon attachment site.Citation23 A fragment of bone or cartilage hanging from the wavy retracted torn tendon end may also be noted.Citation24
2 Subjects and methods
2.1 Patients
This is a prospective study conducted among patients subjected to knee trauma and suspected clinically to have PLC injuries, referred to the Radio-diagnosis Department of Alexandria Main Hospital selected with the following inclusion criteria: sport injuries, fall from height, twisting injury and road traffic accident.
The study excluded those with any history of knee operative interference, non-traumatic painful knee, claustrophobic patients and anomalous ossifications of the lateral femoral condyle.
2.2 Methods
Patients were subjected to full history taking and thorough clinical examination, CT whenever possible as well as MRI using a 1.5 T Philips Gyroscan Achieva (Best, The Netherlands) closed configuration scanner using a dedicated 8 channels extremity coil as well as using a 1.5 T whole body scanner (Magnetom, Avanto by Siemens, Erlangen, Germany) using a dedicated 8 channels extremity coil.
All patients were subjected to the following MRI protocols: 1. Rapid localizer sequence including axial, coronal and sagittal sequences. 2. Sagittal T1 weighted image utilizing the following parameters: A repetition time (TR) of 500msec, an echo time (TE) of 20msec, a slice thickness of 4 mm, a gap of 0.3 mm, FOV = 200 mm and NSA = 1. 3. Sagittal T2 weighted image utilizing the following parameters: A repetition time (TR) of 3000 msec, an echo time (TE) of 100 msec, a slice thickness of 4 mm, a gap of 0.3 mm, FOV = 200 mm and NSA = 2. 4. Sagittal PDW fat suppressed images utilizing the following parameters: A repetition time (TR) of 2500 msec, an echo time (TE) of 30 msec, a slice thickness of 4 mm, a gap of 0.4 mm, FOV = 180 mm and NSA = 2. 5. Sagittal gradient images utilizing the following parameters:A repetition time (TR) of 400 msec, an echo time (TE) of 14 msec, flip angle 30°, a slice thickness of 3 mm, a gap of 0.4 mm, FOV = 180 mm and NSA = 2. 6. Axial T2weighted image utilizing the following parameters: A repetition time (TR) of 3000 msec, an echo time (TE) of 100 msec, a slice thickness of 4 mm, a gap of 0.5 mm, FOV = 180 mm and NSA = 1. 7. Coronal PDW fat suppressed images utilizing the following parameters: A repetition time (TR) of 2500 msec, an echo time (TE) of 30 msec, a slice thickness of 4 mm, a gap of 0.4 mm, FOV = 180 mm and NSA = 2 (see –).
Fig. 4 Showing different grades of injury of the popliteus musclotendinous complex in our study. Sagittal PDFS (A) showing grade I strain of the myotendinous fibers. Sagittal PDFS (B) showing grade II strain (partial tear) of the muscle fibers. Coronal T2 gradient sequential images (C) showing grade III strain (complete tear) of the popliteus tendon near its femoral insertion associated with also complete tear of the lateral collateral ligament as well as the illiotibial tract.
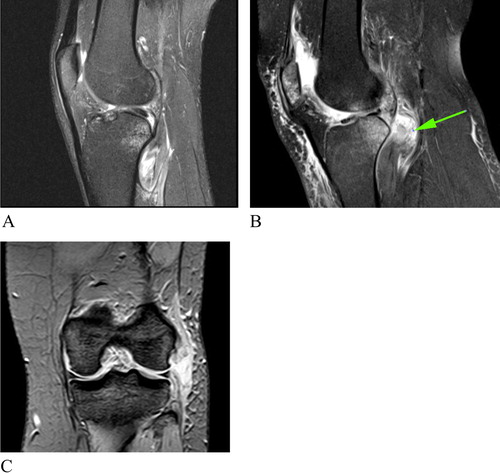
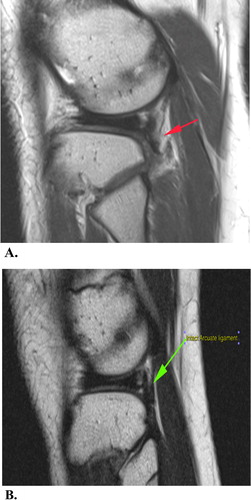
Fig. 6 Sagittal T2 TSE (A) shows ill definition of the arcuate ligament just posterior to the popliteus tendon suggestive of its tear in our case. Sagittal T2 TSE (B) shows intact arcuate ligament in a normal individual for comparison.
2.3 Image analysis
The MR images were carefully examined for evaluation of 1. The presence of injury of the different PLC structures including the lateral collateral ligament, popliteus muscle complex, conjoined tendon, biceps femoris tendon, lateral head of gastrocnemius, popliteofibular ligament and ilio-tibial band, 2. Grading of the injury of the popliteus muscle complex.
3 Results
Regarding the suggested mechanism of action of the PLC injury, nine (60.00%) patients had a non-contact external rotation injury while six (40.00%) patients were suffering from a direct blow to the antero-medial tibia with hyperextension to the knee.
Regarding the incidence of injury of the popliteus musclotendinous complex among our studied 15 patients with posterolateral corner injuries, eight (53.33%) patients had popliteus complex injuries while five (33%) patients showed injury of the popliteofibular ligament
Regarding the incidence of combined injuries of the popliteus musclotendinous with other posterolateral corner structures, 7 (87.5%) patients showed combined popliteus muscle injuries with other posterolateral structures while one (12.5) patient had isolated popliteus musclotendinous injury. All (100%) patients with popliteofibular ligament injury showed associated injuries of one or more structures of the posterolateral corner.
Regarding the different incidences of the other posterolateral structures affected in the total number of posterolateral corner injured patients, 10 (67.00%) patients had lateral collateral ligament injury, six (40.00%) patients had injury of their conjoined tendon, five (33%) patients showed ill definition of the arcuate ligament suggesting its tear, and similar number (percentage) showed biceps femoris tendon injury while only one (7%) injury of the lateral head of gastrocnemius and illiotibial band were encountered for each in our study.
Regarding the different sites and patterns of injury of the popliteus musclotendinous complex seen in eight of our patients, four (50%) patients showed intra-substance MRI signal denoting grade I strain, three (38%) patient showed MRI signal with partial discontinuation of the musclotendinous fibers denoting grade II strain, and one patient (12.5%) showed grade III strain. Four (50%) patients had myotendinous junction and muscle belly injuries, two (25%) patients had popliteus tendon injury, while two (25%) patients had combined popliteus tendon and popliteus muscle belly injuries.
4 Discussion
Radiologists should be familiar with the precise anatomy and attachments of the popliteus musclotendinous complex being one of the main stabilizers of the posterolateral corner of the knee, leading to improvements in treatment and functional outcomes for patients in whom the injury was not clinically suspected.
Regarding the suggested mechanism of action in our study, it was found that there are two main mechanisms of action suggested in patients with posterolateral lateral corner injury; these include a non-contact external rotation twisting injury and a direct blow to the antero-medial tibia with hyperextension to the knee constituting 60% and 40% of our patients respectively. Our results agreed with BakerCitation25 who suggested that such injuries occur due to blows to the antero-medial aspect of the proximal tibia with the knee hyperextended or to noncontact hyperextension with external rotation. On the other hand our results disagreed with the findings of Brown et al.Citation26 who could not find any clear mechanism of injury in their study of 24 patients.
Eight (53.33%) of the patients had popliteus complex injuries, 7 (87.5%) of them showed combined popliteus muscle injuries with other posterolateral structures while one (12.5%) had isolated popliteus musclotendinous injury. Five (33%) patients showed injury of the popliteofibular ligament, all of which showed associated injuries of one or more structures of the posterolateral corner. Similar findings were reported by LaPrade et al.Citation18 stating that 72–87% of PLC injuries were combined ligamentous and tendinous injuries. Also it’s clear in our study that isolated popliteus musclotendinous complex were uncommon and encountered in only one (12.5)% of our cases with popliteus injury, and that was similar to the findings of WestrichCitation27 which showed that less than 10% of the popliteus tears were isolated. Similarly Mirkopulos et al.Citation28 reported that isolated injuries of the popliteus muscle are unusual found in four patients only in their study.
Our study depicted that the popliteus musclotendinous unit as well as lateral collateral ligament, conjoined and biceps femoris tendons constitutes the mainstay for posterolateral corner integrity of the knee; being the most commonly injured structures constituting about 53.33%, 67%, 40% and 33.33% respectively. These results were a little different from those of Theodorous et al.Citation15 who stated that injury of the lateral collateral ligament was found in 100% of their patients, followed by the biceps femoris tendon (79%) and popliteus complex (36%). Collins et al.Citation29 found injury of the LCL in 100% of their patients, popliteus muscle injury in 95% and biceps femoris injury in 77.3%.
Regarding the site of injury of the popliteus muscle, our study found that injuries of the popliteus muscle most commonly involve the muscle belly and myotendinous junction constituting about 50%, while 25% of our cases showed injury of the popliteus tendon and 25% had combined popliteus tendon and popliteus muscle belly injuries. These findings were matching with Brown et al.Citation26 who stated that 23 of 24 patients (96%) in their study had a tear of the popliteus that involved the muscular portion and similarly MirkopulosCitation28 reported that avulsion injuries at the femoral insertion of the popliteus tendon have been reported; however injuries of the muscle belly and myotendinous junction of the popliteus are far more common.
On the other hand the popliteofibular ligament was described by Wadia et al.Citation13 as a constant structure, yet in our study it was difficult to be visualized on axial images, but it was more reliably depicted in coronal images just deep to the lateral geniculate vessels which agreed with the findings of Theodorou et al.Citation15 and Helms et al.Citation30 and thus injury to the ligament was suggested in 33% of our patients based on its ill definition at the previously described anatomical location compared to normal templates as well as the bony and soft tissue ligamentous disruption noted at the posterior aspect of the apex of the fibular head, just medial to the arcuate ligament attachment. Collins et al.Citation29 found the popliteofibular ligament to be disrupted in 82.6% of their patients. In one study done by Yu et al.Citation31 use of a coronal oblique plane compared with a standard coronal plane improved visualization of this ligament from 8% of knees to 53%. However, this oblique plane unfortunately wasn’t done in our study to avoid patient discomfort due to prolonged examination time.
5 Conclusion
We concluded that among the different PLC structures, the most common structures injured are the fibular collateral ligament, biceps femoris tendon, conjoined tendon and popliteus musclotendinous complex. The anatomy and different attachments of the popliteus musclotendinous complex should be thoroughly examined by the radiologist specially when a clinical suspicion of posterolateral instability is encountered. The most common site of injury was found to be the muscle belly and myotendinous junction while the most common type of injury was found to be grade I strain.
Conflict of interest
The authors declared that there is no conflict of interest.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 30 September 2017
References
- M.E.RuizS.J.EricksonMedial and lateral supporting structures of the knee: normal MR imaging anatomy and pathologic findingsMagn Reson Imaging Clin N Am21994381399
- D.B.JenkinsHollinshead’s functional anatomy of the limbs and back1991SaundersPhiladelphia, PA233305
- T.T.MillerP.GladdenR.B.StaronJ.H.HenryF.FeldmanPosterolateral stabilizers of the knee: anatomy and injuries assessed with MR imagingAJR Am J Roentgenol169199716411647
- M.De MaeseneerM.ShahabpourK.VanderdoodF.De RidderF.Van RoyM.OsteauxPosterolateral supporting structures of the knee: findings on anatomic dissection, anatomic slices and MR imagesEur Radiol11200121702177
- H.U.StäubliS.BirrerThe popliteus tendon and its fascicles at the popliteal hiatus: gross anatomy and functional arthroscopic evaluation with and without anterior cruciate ligament deficiencyArthroscopy61990209220
- R.F.LaPradeT.V.LyF.A.WentorfL.EngebretsenTheposterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendonAm J Sports Med312003854860
- F.P.ReisC.A.de CarvalhoAnatomical study on the proximal attachments of the human popliteus muscleRev Bras Pesqui Med Biol81975373380
- Y.WatanabeH.MoriyaK.TakahashiFunctional anatomy of the posterolateral structures of the kneeArthroscopy919935762
- J.F.LovejoyJrT.P.HardenPopliteus muscle in manAnat Rec1691971727730
- K.UllrichW.K.KrudwigU.WitzelPosterolateral aspect and stability of the knee joint. I. Anatomy and function of the popliteus muscle-tendon unit: an anatomical and biomechanical studyKnee Surg Sports Traumatol Arthrosc1020028690
- S.JadhavS.MoreR.RiascosD.LemosL.SwischukComprehensive review of the anatomy, function and imaging of the popliteus and associated pathologic conditionsRadiographics342014496513
- C.T.Moorman3rdR.F.LaPradeAnatomy and biomechanics of the posterolateral corner of the kneeJ Knee Surg182005137145
- F.D.WadiaM.PimpleS.M.GajjarA.D.NarvekarAn anatomic study of the popliteofibular ligamentInt Orthop272003172174
- M.MunshiM.L.PretterklieberS.KwakG.E.AntonioD.J.TrudellD.ResnickMR imaging, MR arthrography, and specimen correlation of the posterolateral corner of the knee: an anatomic studyAJR Am J Roentgenol180200310951101
- D.J.TheodorouS.J.TheodorouD.C.FithianL.PaxtonD.H.GarelickD.ResnickPosterolateral complex knee injuries: magnetic resonance imaging with surgical correlationActa Radiol462005297305
- D.M.SwensonC.L.CollinsT.M.BestEpidemiology of knee injuries among U.S. high school athletes, 2005/2006-2010/2011Med Sci Sports Exercise452013462
- A.RanawatC.L.Baker3rdS.HenryC.D.HarnerPosterolateral corner injury of the knee: evaluation and managementJ Am Acad Orthop Surg162008506
- R.F.LaPradeF.A.WentorfH.FrittsA prospective magnetic resonance imaging study of the incidence of posterolateral and multiple ligament injuries in acute knee injuries presenting with a hemarthrosisArthroscopy23200713411347
- Davis KW, Sanin A. Knee: ligamentous pathology. In: Blankenbaker DG, Davis KW, editors. Diagnostic imaging trauma, 2nd ed.; 2016. p. 740.
- W.E.PalmerS.J.KuongH.M.ElmadbouhMR imaging of myotendinous strainAJR Am J Roentgenol1731999703709
- L.S.SteinbachJ.L.FleckensteinJ.MinkMagnetic resonance imaging of muscle injuriesOrthopedics171994991999
- M.A.StevensG.Y.El-KhouryM.H.KatholE.A.BrandserS.ChowImaging features of avulsion injuriesRadioGraphics191999655672
- D.A.ConnelH.G.PotterM.F.ShermanT.L.WickiewiczInjuries of the pectoralis major muscle: evaluation with MR imagingRadiology2101999785791
- G.D.BatesM.T.HreskoD.JaramilloPatellar sleeve fracture: demonstration with MR imagingRadiology1931994825827
- C.L.BakerL.A.NorwoodJ.C.HughstonAcute posterolateral rotatory instability of the kneeJ Bone Joint Surg Am651983614618
- T.R.BrownS.F.QuinnJ.P.WenselJ.H.KimT.DemlowDiagnosis of popliteus injuries with MR imagingSkeletal Radiol241995511514
- G.H.WestrichJ.A.HannafinH.G.PotterIsolated rupture and repair of the popliteus tendonArthroscopy111995628632
- N.MirkopulosT.MyerIsolated avulsion of the popliteus tendonAm J Sports Med191991417419
- Mark S.CollinsMRI injury patterns in surgically confirmed and reconstructed posterolateral corner knee injuriesKnee Surg Sports Traumatol Arthrosc201529432949
- C.A.HelmsN.M.MajorM.W.AndersonP.A.KaplanR.DussaultKneeMusculoskeletal MRI2nd ed.2009Saunders ElsevierPhiladelphia, PA353383
- J.S.YuD.C.SalonenJ.HodlerP.HaghighiD.TrudellD.ResnickPosterolateral aspect of the knee: improved MR imaging with a coronal oblique techniqueRadiology1981996199204