
Abstract
Background
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy in the upper extremity. Nerve conduction studies (NCS) is the most valid way of diagnosing CTS in combination of these clinical symptoms together with positive signs by physical examination. Ultrasonography is a useful non-invasive diagnostic method for CTS and there is considerable correlation between the electrophysiological tests and the measurements of cross-sectional area (CSA) by ultrasonography. Many studies have shown that the carpal tunnel syndrome seems to occur more frequently in patients with diabetes mellitus and might be associated with the duration of diabetes mellitus, microvascular complications and degree of glycemic control. Although diabetes mellitus is a risk factor for CTS, reports about median nerve CSA measurements between CTS patients with and without DM are scant. This prospective study aimed to evaluate whether or not ultrasonographic findings of the median nerve is different between DM and non-DM-CTS patients. To correlate the diagnostic results in both DM and non-DM-CTS patients.
Patients and methods
Thirty six non-diabetic patients and twenty five diabetic patients with CTS were assessed. All patients were subjected to thorough history taking, full clinical examination, electrophysiological assessment of wrists and gray scale ultrasonography (US).
Results
High mean cross sectional area of median nerve (CSA) on ultrasonographical studies was detected with non-significant difference between both groups. Additionally, a non-significant difference for flattening ratio was found between two groups. Moreover, there was a highly significant positive correlation between electro diagnostic and ultrasonographic results in diabetic patients.
Conclusion
The CSA of median nerve is larger in CTS hands in both DM and non-DM patients. Mean electro-diagnostic parameters were not significant predictors of CTS in patients with diabetes. The combination of electrophysiological and ultrasonography provides diagnostic effective tools across the entire spectrum of CTS in diabetic and non-diabetic patients. Nevertheless, screening for DM in patients with CTS is not recommended.
1 Introduction
Carpal tunnel syndrome (CTS) is the most common form of entrapment neuropathies.Citation1 CTS is a combination of finger, hand, and arm distress with symptoms that reflect sensory or motor compromise.Citation2 Female gender, obesity, increase of age, hypothyroidism, pregnancy, rheumatoid arthritis, osteoarthritis and occupational factors like repetitive work are identified as the main risk factors for CTS.Citation3 In addition, previous studies stated that diabetes mellitus (DM) is also considered as a risk factorCitation4–Citation8 with a higher incidence of CTS in patients with pre-diabetes.Citation9 A relationship between HbA1c, duration of DM, micro vascular complications and CTS had been stated.Citation10 Entrapment disorders are highly prevalent in patients with diabetes, the most common neuropathy being carpal tunnel syndrome (CTS).Citation11 However, Hendriks et al.Citation3 reported that although type 2 diabetes was more frequently diagnosed among patients with carpal tunnel syndrome, it could not be identified as an independent risk factor. The high prevalence of CTS among patients with diabetes might be as a result of repeated undetected trauma, metabolic changes, accumulation of fluid or edema within the confined space of the carpal tunnel and /or diabetic cheiroarthropathy.Citation11
Fig. 2 Correlation between Flattening Ratio and CMAP.
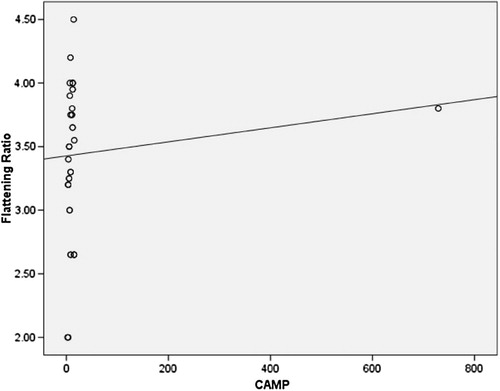
Fig. 3 Correlation between Flattening Ratio and MNCV.
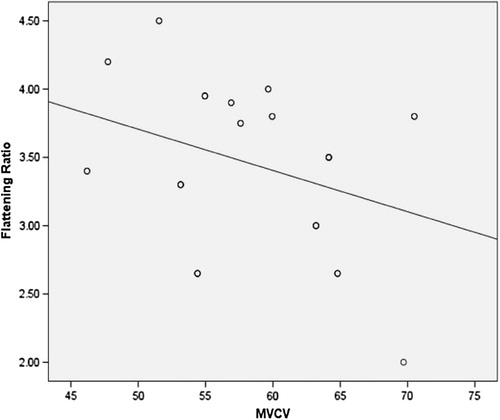
Fig. 4 Correlation between CSA and FW.
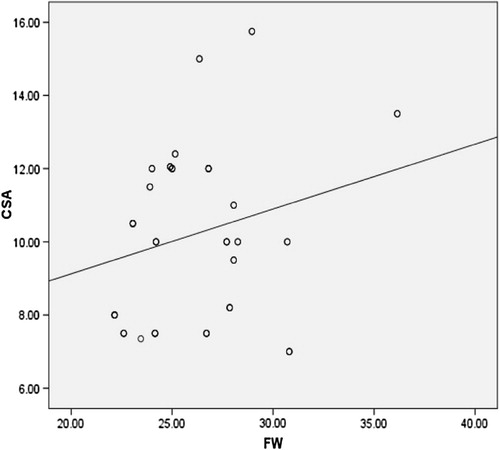
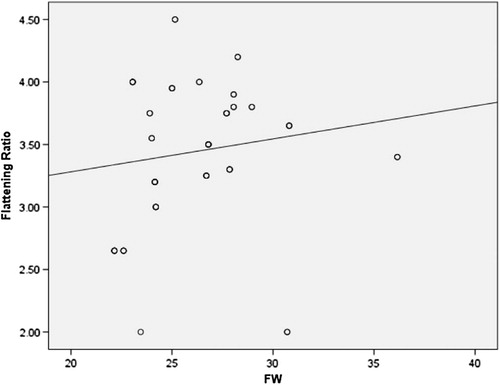
Fig. 5 Correlation between Flattening Ratio and FW.
Electrodiagnostic studies (nerve conduction studies and electromyography) are useful in diagnosis and in differentiation from cervical radiculopathy, diabetes or peripheral neuropathy.Citation2 Nerve conduction studies alone do not provide spatial information regarding the nerve or its attendant abnormalities.Citation12 Ultrasonography (US) has emerged as simple, low cost, rapid accurate and non-invasive imaging method for evaluating the median nerve in the carpal tunnel syndrome.Citation13 Many reports have appeared that agreed that US has high sensitivity and specificity in CTS diagnosis. It can detect the median nerve compression characteristics, provide anatomical images of the median nerve, neighboring structures and space occupying lesions as ganglia neural tumors.Citation2,Citation14 US has been used in clinical evaluation of CTS in diabetic neuropathy.Citation15
Diabetes mellitus is a chronic metabolic disorder, which is characterized by persistent hyperglycemia with resultant morbidity and mortality in relation to its micro- and macrovascular complications. “The diabetic hand” is a term used to describe pathological hand manifestations that are more commonly found in diabetes. It represents the following musculoskeletal disorders; limited joint mobility, Dupuytren’s contracture, flexor tenosynovitis and carpal tunnel syndrome. Combined occurrence of CTS and diabetes has been acknowledged for many years. Carpal tunnel syndrome (CTS) and diabetic polyneuropathy (DPN) are common conditions in patients with diabetes and therefore frequently occur concomitantly. Diagnosis of CTS in patients with DPN is important, as therapeutic interventions directed toward relief of CTS may be effective irrespective of diffuse neuropathy. The purpose of this study is to evaluate whether or not ultrasonographic findings of the median nerve is different between DM and non-DM-CTS patients. To correlate the diagnostic results in both DM and non-DM-CTS patients.
2 Patients and methods
This prospective study was conducted on sixty-one patients (122 wrists : 51 females and 10 males), their ages ranged 23–82 years old (mean ± SD 35.01 ± 3.17 years), referred from out-patients clinics of departments of Neurology, Orthopaedic, Internal Medicine and Rheumatology and Rehabilitation, Aswan and Assuit University Hospitals, Aswan, Assuit, Egypt. All patients clinically diagnosed with carpal tunnel syndrome lasting for at least one month (Forty patients had bilateral CTS and Twenty-one patients had unilateral CTS) in the period from January 2014 to December 2014 were included. The duration of illness ranged 6 ms-10 years old with mean ± SD 3.2 ± 2.1 years. For analysis purposes, The patients were classified into two groups according to Diabetes mellitus into thirty-six non diabetic patients (group I), their ages ranged 14.7–68 years old (mean age 35.7 ± 12.8 years) and twenty-five diabetic patients (group II), their ages ranged 14.7–68 years old (mean age 34.1 ± 13.9 years) . Exclusion criteria included pregnant women, those diabetic patients with clinical and electrophysiologic diagnosis of diabetic polyneuropathy, those with history of underlying disorders associated with CTS such as renal and hepatic diseases, patients with gout, rheumatoid arthritis or thyroid disease, patients with previous wrist surgery (including carpal tunnel injection), and those with clinical or electrophysiological evidence of accompanying condition that mimics CTS as cervical radiculopathy. Clinical CTS was defined according to the criteria of the American Academy of Neurology practice parameters. A written consent was obtained from all participants and approval from the local ethics committee of Faculty of Medicine, Aswan and Assuit Universities was obtained. All patients were subjected to full history taking, thorough clinical examination and neurological examination including (1) paresthesia, pain provoked or worsened by sleep, sustained hand or arm position or repetitive action of the hand or wrist that is mitigated by a change in posture or by shaking of the hand (2) sensory deficit in median nerve distribution, (3) motor deficit of median innervated thenar muscles and (4) positive provocative tests for CTS (Tinel sign, Phalen test and Reverse Phalen test). The clinical diagnosis of CTS was made when criterion 1 and one or more of criterion 2–4 were fulfilled.Citation16,Citation17 Electrophysiological assessment of wrists and gray scale ultrasonography were done for all patients.
Table 1a Socio-demographic characteristics of the studied sample.
Table 1b Baseline characteristics of the study participants.
3 Electrodiagnostic testing
Electrophysiological assessment of wrists was done according to the recommended AAEM protocol using Neuropack XI/EMG/EP measuring system, MEB-2300 in the Neurophysiological unit, Neuropsychiatry Department, Faculty of Medicine, Aswan University. The Median nerve sensory action potential amplitude, latency and sensory conduction velocity (CV) were measured. The Median nerve motor amplitude, distal motor latency (DML) and motor conduction velocity were measured by using standard techniques of supramaximal cutaneous stimulation and surface electrodes. F-response latency of median nerve was obtained to exclude proximal affection of the median nerve roots. Ulnar nerve sensory and motor conduction studies were performed. Needle EMG was done in abductor pollicis brevis muscle to determine the severity of CTS and additional muscles in the upper limb to exclude proximal median nerve neuropathy, brachial plexopathy or radiculopathy. Measurements performed and cut-off points or normal values used in our study were as follows: (1) median nerve distal sensory latency, upper limit of normal 3.6 ms (2) distal motor latency over the thenar, upper limit of normal 4.3 ms (3) median motor nerve conduction velocity, lower limit of normal 49 m/s (4) median sensory nerve conduction velocity, lower limit of normal 49 m/s according to Delisa et al.Citation18. The diagnostic criteria of electrodiagnostic tests for CTS were: Reduction in the median nerve sensory CV of less than 50 m/s, Prolongation of median nerve DML more than 4.3 ms, No abnormalities in the proximal median nerve. The severity of electrophysiological CTS impairment was assessed according to the modified scoring system of Padua et al.Citation19
4 The ultrasonographic imaging analysis
All patients underwent sonographic examination of the carpal tunnel. Both hands were examined. US examination was performed by using a 12 MHz linear array transducer (Phillips, HD 11 XE), at the Radio diagnosis department at Aswan University Hospital. The sonographic examination was done at the same day or within days of the electrophysiological study. The median nerve was examined in the transverse and longitudinal planes along the carpal tunnel by gray scale US to investigate the presence of median nerve compression criteria, including the measurement of cross sectional area (CSA) and flattening ratio of median nerve. The cut-off value of cross-sectional area at the tunnel inlet was 9.5 mm2 Kang et al.Citation20
4.1 Statistical analysis
The collected data were verified, coded by the researcher, then analyzed by the Statistical Package for Social Sciences (SPSS/PC/VER 21). Descriptive statistics: mean, standard deviation, median, range, frequencies, percentage were calculated. Test of significances: Chi square test was used to compare the difference in distribution of frequencies among different groups. Student t-test was calculated to test the mean differences in continuous variables between groups. Pearson’s correlation co-efficient was calculated for parametric variables and Spearman’s Ranked correlation co-efficient was calculated for non-parametric variables. Significant test results were considered when p value was ≤.05.
5 Results
The socio-demographic characteristics of the studied patients with carpal tunnel syndrome are presented in  and . Sixty-one patients were studied (83.3 % females and 16.7% males). Their ages ranged 23–82 years old (with mean ± SD, 35.01 ± 3.17 years). They were classified according to Diabetes Mellitus into two groups: group I were non- diabetic group (thirty-six patients (59%), with mean of age ± SD 35.7 ± 12.8 years) with the mean duration of disease was 3.21 ± 1.9 years, and group II were diabetic group (Twenty-five (41%) with mean age ± SD 34.1 ± 13.9 years) with the mean duration of disease was 3.12 ± 2.3 years. A considerable number of patients (40, 65.5%) with or without diabetes mellitus demonstrated bilateral carpal tunnel syndrome with more prevalence in group I (57.5%) of non-statistical importance. No statistically differences regarding the age, gender, increased duration of CTS or laterality between two groups.
Regarding electro diagnostic studies of the median, a statistically significant difference between two groups was found in the CMAP, MNCV, DSL and F-wave of median nerve (p < .001, .002, .03 and .04 respectively) (see ).
Table 2 Parameters of electrodiagnostic testing between Non –DM -CTS and DM-CTS groups.
CSA as well as FR of median nerve was larger in Non-DM-CTS-Hands and DM-CTS-Hands with no statistically difference between two studied groups (see ).
Table 3 Parameters of ultrasonography among the groups.
In diabetic patients with CTS, regarding the correlation between electrodiagnostic and sonographic results, there was statistically significant positive correlations between distal motor latency (DML) of median nerve and CSA (p-value = .003). Moreover, there was statistically negative correlation between amplitude (CMAP), motor conduction velocity (MNCV) and FR (p-value = .001 and .023 respectively). Furthermore F-wave had statistically significant positive correlation with both CSA and FR (p-value = .035 and 0.031 respectively). Interestingly, there was statistically positive correlation between the duration of DM and CSA but not with FR (see and –).
Fig. 1 Correlation between CSA and DML.
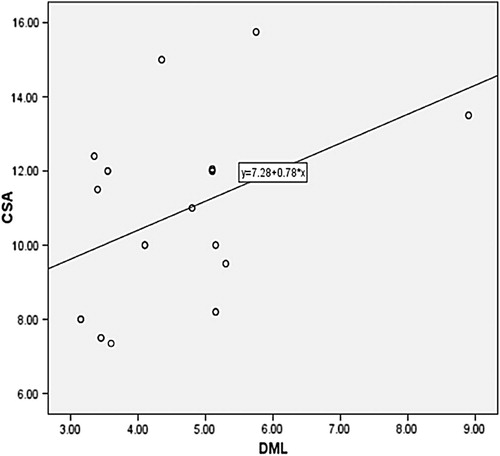
Fig. 6 Correlation between CSA and DM Disease Duration.
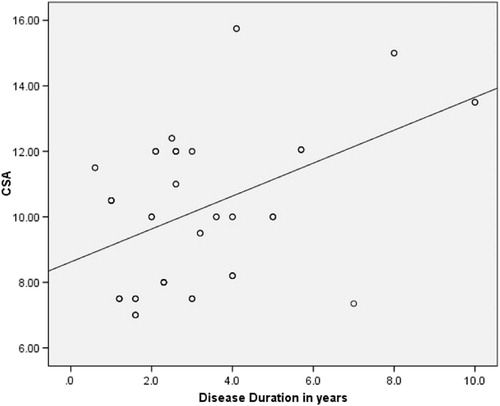
Table 4 Correlation among glycemic state of the patients, CSA, Flattening Ratio and electrodiagnostic testing of the median nerve.
6 Discussion
Carpal tunnel syndrome (CTS) is the commonest entrapment neuropathy and accounts for approximately 90% of all entrapment neuropathies with prevalence of approximately 3–6% of adults in the general population.Citation2 The reason as to why CTS is more common in diabetes is unknown and an early diagnosis is essential to prevent permanent nerve damage and functional squeals.Citation7
Confirmation of CTS is usually based on electrophysiological studies. However, many authors have proposed that conventional electrophysiological studies are not appropriate for detecting mild median nerve compression. Even when electrodiagnostic tests are applied, it is difficult to distinguish CTS from other neuropathic syndromes in diabetic patients.Citation21–Citation23 Ultrasonography (US) has been used in clinical studies on diabetic neuropathy, however its use in the clinical evaluation of CTS in diabetic patients has not been reported.Citation24 To date, rare studies evaluated the value of ultrasonography (US) between diabetic and non- diabetic patients with clinical and electro diagnostic- confirmed CTS. In the current study, our results are consistent with previous studies of ultrasound in CTS in showing enlargement of median nerve in CT hands.Citation25 We found a larger measurement of CSA and FR of median nerve in studied patients when examined on both sides. However, we found no significant difference between diabetic and non diabetic patients in measurement of CSAs. This findings could be explained by that the biological response to compression is the more important contributing factor rather than diabetic peripheral nerve injuries and the use of small sized sample of diabetic CTS patients in our study. Our finding was consistent withCitation26 who reported that the CSA of the median nerve was larger in both DM CTS and non-DM CTS groups compared to those without CTS. Agirman et al.Citation27 found more larger median nerve CSA in diabetic patients with carpal tunnel syndrome at wrist levels compared with those of the healthy controls. Watanabe et al.Citation15 and 2010Citation28 showed that the median nerve (at wrist) and tibial nerve (at the ankle) CSAs were increased in diabetic patients when compared with their control group. Moreover, we found increased FR in non diabetic and diabetic group CTS patients without significant difference between both groups. These findings were in agreement with Tsai et al.Citation26 who revealed significantly larger measurement of CSA of median nerve in both non diabetic and diabetic patients. However, in contrast to our observations, Chen et al.Citation24 stated that the measured CSAs in both diabetic and DPN groups were larger than those measured in the idiopathic, non diabetic and control groups. Moreover, our findings were in concordance with Boyaci et al.Citation29 who found statistically significantly greater FR in the DM –CTS groups than that of the control groups (see and )
Fig. 7 A 35 year female diabetic patient with severe bilateral carpal tunnel syndrome: (A & B) transverse image of the right and left median nerves at the inlet of the carpal tunnel showed increased cross sectional area, respectively measured 24.9 and 27.6 mm2, C) the estimated flattening ratio of right median nerve is 1:3.7.
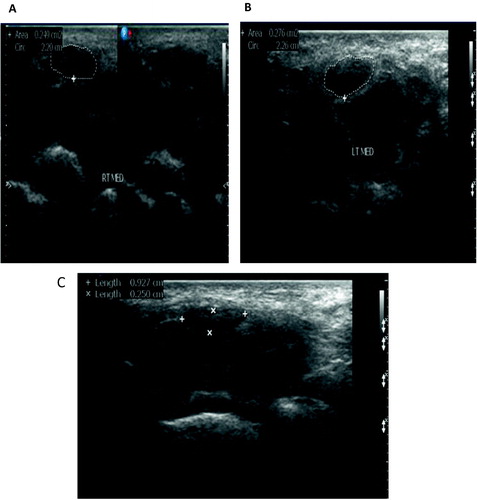
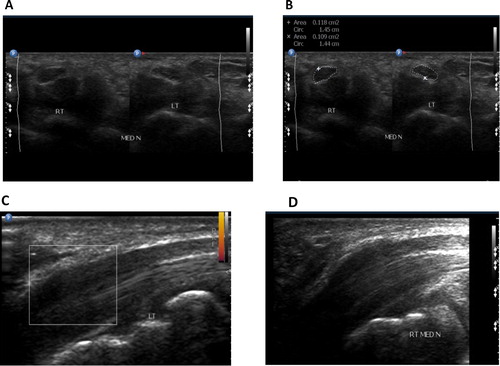
Fig. 8 A 28 year female non diabetic patient with bilateral mild carpal tunnel syndrome: (a, b) transverse image of the right and left median nerves at the inlet of the carpal tunnel; cross sectional area respectively measured 11.8 and 10.9 mm2. (c, d) Longitudinal image of the right and left median nerves showed focal swollen of the nerve at the inlet of carpal tunnel.
Among Diabetic patients with CTS, we showed highly statistically significant positive correlations of CSA with motor distal latency of median nerve. Moreover, both CSA and FR were significantly and positively correlated with F-wave latency of median nerve. These findings were in agreement with Watanabe et al.Citation15 who reported that the CSA in the carpal tunnel was correlated with delayed latency of median nerve. This arise the assumption that enlargement of the median nerve damages the myelin and results in the slowing of nerve conduction velocity. On the other hand, in agreement to our observation, Tsai et al.,Citation26 revealed that the CSA of the median nerve positively correlates to the distal motor latency of the median CMAP and F wave while he revealed negative correlation between the measurements of CSA of the median nerve and the amplitude of the median CMAP suggesting that median nerve swelling contributes to axonal degeneration of the median nerve in CTS, in contrast to our results that found no correlation between CSA measurement, amplitude of the median nerve CMAP and the distal sensory latency of the median nerve.
This current study needs further studies and challenges. Several limitations should be mentioned: First, cases were only enrolled in a secondary care setting and thereby mostly severe cases were included. Thus, less severe CTS patients treated with conservative treatment by general practitioners did not participate in the current study. Therefore, the generalizability of our results is limited to secondary care. Furthermore, differential misclassification bias could have occurred because patients with the diabetic patients with suspected polyneuropathy by clinical presentation and have CTS should be excluded and they need further studies and evaluation. Third is that the association between the duration of diabetes and the electrophysiological and ultrasonographic findings should be considered. Finally, our number of cases is small so, more studies are needed and included more larger number of cases.
7 Conclusion
The combination of electrophysiological and ultrasonography provides diagnostic effective tools across the entire spectrum of CTS in diabetic patients. Moderate to severe degrees of CTS and high mean CSA on ultrasonographical studies were characteristic patterns especially in diabetic patients. Moreover, there was a highly significant negative correlation between diabetic and non-diabetic patients evaluated by NCS and US. The prevalence of clinical CTS and the most efficient electro-diagnostic discriminators of CTS from diffuse neuropathy are uncertain. Nevertheless, screening for DM in patients with CTS is not recommended.
Conflicts of interest
There are no conflicts of interest.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 24 November 2017
References
- R.A.WernerM.AndaryCarpal tunnel syndrome: pathophysiology and clinical neurophysiologyClin Neurophysiol113200213731381
- R.E.MohamedM.A.AminA.A.AboelsafaS.E.ElsayedContribution of power Doppler and gray-scale ultrasound of median nerve in evaluation of carpal tunnel syndromeEgypt J Rad Nucl Med452014191201
- S.H.HendriksP.R.Van DijkK.H.GroenierP.HouptH.J.G.BiloN.KleefstraType 2 diabetes seems not to be a risk factor for the carpal tunnel syndrome: a case control studyBMC Musculoskelet Disord152014346
- M.A.J.Van DijkJ.B.ReitsmaJ.C.FischerG.T.B.SandersIndications for requesting laboratory tests for concurrent diseases in patients with carpal tunnel syndrome: a systematic reviewClin Chem49200314371444
- J.M.GeogheganD.I.ClarkL.C.BainbridgeC.SmithR.HubbardRisk factors in carpal tunnel syndromeJ Hand Surg Br292004315320
- J.BeckerD.B.NoraI.GomesAn evaluation of gender, obesity, age and diabetes mellitus as risk factors for carpal tunnel syndromeClin Neurophysiol113200214291434
- Y.karpitskayaC.B.NovakS.E.MackinnonPrevalence of smoking, obesity, diabetes mellitus and thyroid disease in patients with carpal tunnel syndromeAnn Plas Surg482002269273
- C.H.TsengC.C.LiaoC.M.KuoF.C.SungD.P.H.HsiehC.H.TsaiMedical and non-medical correlates of carpal tunnel syndrome in a Taiwan cohort of one millionEur J Neurol1920129197
- M.C.GullifordR.LatinovicJ.CharltonR.A.C.HughesIncreased incidence of carpal tunnel syndrome up to 10 years before diagnosis of diabetesDiabet Care29200619291930
- R.SinghG.GambleT.CundyLifetime risk of symptomatic carpal tunnel syndrome in Type 1 diabetesDiabet Med222005625630
- A.VinikA.MehrabyanL.ColenFocal entrapment neuropathies in diabetesDiabet Care27200417831788
- T.W.TaiC.Y.WuF.C.SuT.C.ChernI.M.JouUltrasonography for diagnosing carpal tunnel syndrome: a meta-analysis of diagnostic test accuracyUltrasound Med Biol387201211211128
- M.K.Abdel-GhaffarM.A.El-sinnawyH.FawzyS.E.IbraheemGray scale and colour Doppler sonography in the diagnosis of carpal tunnel syndromeEgypt J Rad Nucl Med432012581587
- K.U.KimH.J.JeonS.H.ParkD.S.ParkH.S.NamValue of ultrasonograhy in the diagnosis of carpal tunnel syndrome: correlation with electrophysiological abnormalities and clinical severityJ Korean Neurosurg Soc5520147882
- T.WatanabeH.ItoA.MoritaY.UnoT.NishimuraH.KawaseEvaluation of the median nerve in diabetic patients: comparison with nerve conduction studiesJ Ultrasound Med282009727734
- H.YouZ.SimmonsA.FreivaldsM.J.KothariS.H.NaiduRelationships between clinical symptom severity scales and nerve conduction measures in carpal tunnel syndromeMuscle Nerve221999497501
- C.K.JableckiM.T.AndaryR.G.FloeterPractice parameter; electrodiagnostic studies in carpal tunnel syndrome: report of the American association of electrodiagnostic medicine, American academy of neurology, and the American academy of physical medicine and rehabilitationNeurology58200215891592
- J.A.L.H.DelisaE.M.BaranK.S.LaiManual of nerve conduction velocity and clinical neurophysiology1994Lippincott Williams & WilkinsPhiladelphia
- L.PaduaM.LoMonacoB.GregoriE.M.ValenteR.PaduaP.TonaliNeurophysiological classification and sensitivity in 500 carpal tunnel syndrome handsActa Neurol Scand961997211217
- S.KangH.K.KwonK.H.KimHyung SeokYunUltrasonography of median nerve and electrophysiologic severity in carpal tunnel syndromeAnn Rehabi Med3620127279
- B.A.PerkinsD.OlaleyeV.BrilCarpal tunnel syndrome in patients with diabetic polyneuropathyDiabet Care25122002565569
- I.YagciO.H.GunduzS.SancakM.AgirmanE.MesciG.AkyuzComparative electrophysiological techniques in the diagnosis of carpal tunnel syndrome in patients with diabetic polyneuropathyDiabet Res Clin Pract882010157163
- S.GaziogluC.BozV.A.CakmakElectrodiagnosis of carpal tunnel syndrome in patients with diabetic polyneuropathyClin Neurophysiol122201114631469
- S.F.ChenC.R.HuangN.W.TsaiC.C.ChangW.N.ChanUltrasonographic assessment of carpal tunnel syndrome of mild and moderate severity in diabetic patients by using an 8-point measurement of median nerve cross-sectional areasBMC Med Imag1220121524
- G.BonderNerve compression syndromesS.PeerG.BonderHigh-resolution sonography in peripheral neurvous system2nded.2008Spring VerlagBerlin Heidelberg72122
- N.W.TsaiL.H.LeeC.R.HuangThe diagnostic value of ultrasonography in carpal tunnel syndrome: a comparison between diabetic and non-diabetic patientsBMC Neurol1320136572
- M.AgirmanI.YagciM.A.LeblebicierD.OzturkG.D.AkyuzIs ultrasonography useful in the diagnosis of the polyneuropathy in diabetic patients?J Phys Ther Sci28201426202624
- T.WatanabeH.ItoA.SekineSonographic evaluation of the peripheral nerve in diabetic patients: the relationship between nerve conduction studies, echo intensity, and cross-sectional areaJ Ultrasound Med2952010697708
- A.BoyaciA.TutogluN.BoyaciAn evaluation of radial and ulnar artery flow characteristics in diabetic patients with carpal tunnel syndrome and the diagnostic value of ultrasonography in these patientsJ Clin Exp Invest522014179185