
Abstract
Background
Candidaemia is an emerging problem and one of the most important nosocomial infections in many hospitals. The aim of this study was to characterize the epidemiology and patient outcomes of candidemia after cardiac surgery at two medical centers in Iran over a nine-year period.
Methods
A retrospective analysis was conducted reviewing the medical records of all patients who underwent surgical treatment of cardiac disease at two medical centers. Demographic data, comorbidities, surgical procedure, length of hospital stay, odds ratio and annual trend for candidemia in cardiosurgical cases were collected and analyzed.
Results
Candidemia was responsible for 1.78% cases of total cardiac surgeries (23,849) in two hospitals. Data showed an overall declining trend for the incidence of candidemia during the study period, so that decreased from 3.81% in 2003–2004 to 0.52% in 2011–2012 (P < .01). The odds ratio was significantly downward (from 1 to 0.14, P < .01). Candidemia had a direct relationship with patiant age, and the mean age was 64.2 years. A remarkable gender difference skewed towards males was observed, and the male/female ratio among candidemia cases <60 and ≥65 years old was 0.82 and 1.79, respectively. Housewives had the highest rate of infection (34.91%). Coronary Artery Bypass Graft was the most common type of surgical intervention. Majority of candidemia patients (89.2%) had risk factor and the most common comorbidities were diabetes. Mean total hospital stay was 17.34 ± 4.69 days.
Conclusions
This study expands the knowledge of the epidemiology and trend of incidence of candidemia in cardiosurgical cases. The survey provides preliminary baseline data for the future monitoring of candidemia, and effective programs for controlling and preventive strategies against the disease in hospitals.
1 Introduction
Candidemia are important nosocomial infection and is associated with high morbidity and mortality resulting in significant increase in the duration of hospitalizations and healthcare costs.Citation1,Citation2 The incidence of nosocomial bloodstream infections caused by Candida spp. has risen in the past 20 years.Citation1,Citation3,Citation4 The second agents of infective endocarditis are the fungi,Citation5,Citation6 and two-thirds of cases of fungal endocarditis are caused by Candida spp.Citation6,Citation7 Among the causative agents of nosocomial bloodstream infections, Candida spp. ranks fourth in the United States and seventh in Europe.Citation1,Citation4,Citation8 Mortality rates have been reported to range from 29% to 76%, with an attributable mortality as high as 49%.Citation1–Citation3
The epidemiology of candidemia varies between regions and countries, For example, an increasing incidence of candidemia in Iceland was reportedCitation9 but the same was not observed in Switzerland, where that the incidence of candidemia had remained unchanged.Citation10 Risk factors such as prolonged use of intravenous catheters, increased use of intracardiac prosthetic devices, long term use of antibiotics, intravenous drug use or narcotic addiction, diabetes mellitus, immunosuppressive therapies as well as open-heart surgery, abdominal surgery, and suffering from haematological malignancies are recognized, however data on the intra-hospital epidemiology of candidemia is scarce.Citation5,Citation11,Citation12 Therefore, it is justifiable to find reliable data for monitoring epidemiologic aspects of disease and prepare a baseline data for future comparison. Although retrospective hospital surveys have limitations, but careful study of them are a useful tool and an economical way of gathering information on human disease.Citation13,Citation14
Without information about the prevalence of nosocomial infections, the control hospital-acquired infections and effective programming for nosocomial infections is almost impossible.Citation15,Citation16 There were limited studies about nosocomial infections in Iran, which supposed 8–10% prevalence rate,Citation17,Citation18 however additional information is needed to determine the country-wide presence of nosocomial infections, including candidemia.
Considering the lack of data on the status of Candida infection after heart surgery in Iran, the present study was conducted to determine: (i) the prevalence, odds ratios (ORs) and trend of candidemia from 2003 to 2012; (ii) the associations of demographic features (such as age, sex and the occupation) with candidemia in operated cases; and (iii) relationship of the comorbidities or predisposing factors on infections and on the in-hospital epidemiology of candidemia at two medical centers in Iran.
2 Patients and methods
A retrospective analysis was conducted reviewing the medical records of all patients who underwent surgical treatment of cardiac disease, between 2003 and 2012 at Lavasani hospital and between 2007 and 2012 at Milad hospital in Tehran, capital of Iran. People from different parts of the country are referred to these hospitals for heart surgery. Patients were included if they had at least one positive blood culture for Candida spp. and signs or symptoms of infection. No informed consent was obtained because of the retrospective nature of this study.
Demographic data, comorbidities or predisposing factors (if any), surgical procedure, and length of hospital stay were collected for each confirmed case of candidemia and then analyzed. Patient information was anonymized and de-identified prior to analysis. The ratios between male and female cases were calculated. Data was collected on an annually basis for indicating any annual trend of candidemia after heart surgery. Odds ratios (odds of candidemia in patient with cardiac surgery during successive years) were calculated.
The mean and standard deviation (SD) were used to describe quantitative data. Frequency was used to describe categorical data. The statistical significance of each difference seen between hospital stay, and between two proportions was evaluated in χ2 tests, and by calculating the Z statistic, respectively. Frequency of surgical procedures was statistically evaluated in Student’s t-tests. The level of significance for all statistical tests was 2-sided, with P-value of <.05. All statistical analyses were done with SPSS software (version 16).
3 Results
The total number of cardiac surgeries recorded in two large medical centers registries in the study period were 23,849 cases (15,964 cases belonged to Lavasani hospital and 7885 to Milad hospital). Among these medical records, 424 (1.78%) patients with confirmed candidemia infection were identified after heart surgery over a 9-year period (). The mean prevalence of the disease in Lavasani and Milad hospitals was 1.87% (298 cases) and 1.60% (126), respectively ().
Table 1 Annual incidence and odds ratios of candidemia among patients with cardiac surgeries at two hospitals in Tehran, Iran.
The odds ratios (ORs) were calculated, assuming the first year’s OR equal to 1.00 as the basis for comparison, and the results are shown in . As it is seen, the overall declining trend was still observed (from 1 to 0.14), and was statistically significant (P < .01).
Data showed an overall downward trend for candidemia in all cases operated during the study period (from 3.81% to 0.52%, P < .01). Thus, the incidence of post-cardiac surgery candidemia decreased from 3.81% in 2003–2004 to 0.51% in 2011–2012 for Lavasani hospital; and also the disease declined from 3.72% in 2007–2008 (first year study) to 0.53% in 2011–2012 for Milad hospital ().
Age and gender distribution pertaining to 424 confirmed cases of candidemia after cardiac surgery and the male/female ratio by age groups are shown in . In the current survey, majority of the candidemia cases were old age. Age group ≥65 was the most affected and represented 40.10% of the total number of candidemia cases. An overall analysis of gender and age of the candidemia cases revealed that the number of males infected was higher than that of females (57.08% vs. 42.92%) with a 1.33 male to female ratio (), while the gender ratio in the general population is about 1.00. The variation in the male: female ratio with age group was not, however, statistically significant. The males/females rate of postoperative candidemia cases showed a direct relationship with patient age.
Table 2 Age and gender distributions of the 424 confirmed cases of post-cardiac surgery candidemia at two medical centers in Tehran, Iran.
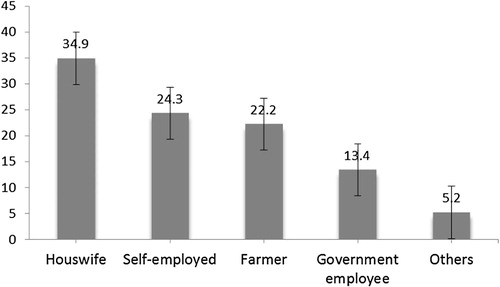
As depicted in , a significantly (P < .05) higher post-cardiac surgery candidemia was recorded in the housewife occupation (34.91%) than each other occupations groups.
Fig. 1 The prevalence of candidemia after cardiac surgery in different occupations at two hospitals in Tehran, Iran.
Coronary Artery Bypass Graft (CABG) was the most common type of surgical intervention and was performed in 381 (89.86%) out of candidemic patients (p < .001). Mitral Valve Repair (MVR) was performed in thirty-seven patients (8.73%), and only 1.41% of cases underwent Atrial Septal Defect (ASD) closure. There was no statistical difference in the mean hospital stays for type of the surgical procedures (p > .35), as shown in .
Table 3 Surgical procedures and hospitalization in confirmed cases of post-cardiac surgery candidemia at two hospitals in Tehran, Iran.
Mean total hospital stay of cases with candidemia after cardiac surgery was 17.34 ± 4.69 days. Most (65.6%) of the candidemic patients required that stay in hospitals from 10 to 19 days following surgery (p < .05). In contrast, only 5.2% of them estimated hospitalization of 25 or more days of hospital stay. The postoperative hospital stay for candidemia patients according to sex is given in .
Table 4 Distribution of candidemia in cardiac surgery cases according to hospital stay categories and gender at two hospitals in Tehran, Iran.
Underlying diseases or predisposing factors of the candidemia in cardiac surgery patients have listed in . The most common predisposing factor included underlying diabetes (38.2% alone, 11.3% diabetes + addiction, 4.5% diabetes + hypertension), and followed by hypertension (18.9% alone and/or with concomitant hyperlipidemia 6.4%). Other underlying diseases or predisposing factors were less frequently seen, and 97 (22.88) patients had more than one underlying diseases. Forty-six patients (10.8%) had no underlying diseases or predisposing factor identified. Postoperative hospital stay among candidemic cases according to predisposing conditions had fluctuations, but there was no statistical difference ().
Table 5 Predisposing factors and hospital stays in post-cardiac surgery candidemia at two hospitals in Tehran, Iran.
4 Discussion
Several studies have shown incidence rates of candidemia have increased significantly in recent years, resulting in a growing number of patients at risk for this disease.Citation19–Citation21 A better understanding of the epidemiology, associated risk factors or underlying diseases for candidemia after cardiac surgery, and postoperative hospital stay is needed but difficult to obtain because of the rarity and lack of large prospective cohorts. Hence, we studied after cardiac surgery patients in order to highlight differences in epidemiology and mentioned outcomes.
In the present study, candidemia was responsible for 424 (1.78%) of total cases (23,849) after cardiac surgeries in two medical centers, and the highest prevalence (3.81%) was recorded in 2003–2004 and lowest the (0.52%) in 2011–2012. Our results were close to some previous reports, for instance, Baddley et al.Citation20 in 2008 and Pasero et al.Citation22 in 2011 reported 1.2% and 1.3% developed candidemia respectively. Previous studies indicated that contamination of operating room especially during reconstruction procedures might play a role. In addition, blood stream infections and candidemia varies with the type of population studied, the type of ward and its location, and the length of the patient’s stay in the hospital.Citation1,Citation2,Citation23
The incidence was collected on an annually basis. This time interval was chosen as being likely to indicate any annual trends. The overall trend was a significant decline in the incidence of Candidemia after cardiac surgery over the study period (P < .01) in both medical centers. The incidence of candidemia decreased from 3.81 and 3.72% per years at the beginning of the study period to 0.51 and 0.53% at the end of the period for Lavasani and Milad hospitals, respectively, (). This may partly be attributed to greater awareness among medical teams, possibly as a result of improvements in surgical technique, prevention of contamination of operating room especially during reconstruction procedures. Another explanation is the implementation of a program which undertook in recent years in order to control infections in operating room, such as the improvement of the clean-air operating theater environment.Citation24,Citation25
In contrast with our findings, a number of previous studies have reported that rate of Candida blood stream infections increased in US,Citation1 EuropeCitation10,Citation26,Citation27 and some other regionCitation28,Citation29 during the last years. Of course, the epidemiology of candidemia remained stable in some parts of the world.Citation10,Citation12,Citation23 In this study, odds ratios (odds of candidemia in patient with cardiac surgery during successive years) showed the overall declining trend was still observed, which was decreased from 1 in the first year (2003–2004) to 0.14 at the end of the study period (P < .01).
Several studies have reported a variation within the rate of candidemia obtained from patients with blood stream infections related to patient age that are in concordance with our observations.Citation12,Citation21,Citation30,Citation31 In the current survey, majority of candidemia cases were old age, and the mean age of patients was about 64.2 years. Age group ≥65 was the most affected and represented 40.10% of the total number of after cardiac surgery patients developed candidemia. These findings are important since it may be inferred that in elderly patients at risk for candidaemia.
An overall analysis of gender and age of candidemia cases after cardiac surgery revealed that the number of males infected was higher than that of females with a 1.33 male to female ratio (), while the gender ratio in the general population is about 1.00. The variation in the male/female ratio among cases generally increasing with age (from 0.82 for the cases aged <60 years to 1.79 among the cases aged ≥65 years), so that a remarkable gender difference skewed towards males was observed. A similar shift towards more candidemia has been reported from many parts of the world, including the review by Ericsson et al. (male-to-female ratio was 206/179 = 1.15),Citation30 Bassetti et al. (male-to-female ratio was = 1.30),Citation21 Ellis et al. (male-to-female ratio was 184/83 = 2.22),Citation24 and Pasero et al. (male-to-female ratio was 1.6).Citation22
Sex predilection as a risk factor for the development of infective Candida is important because past studies have historically demonstrated a prevailing male predominance for the disease. This observation has been due in part to the associated male sex predilection with postoperative candidemia. Increasing age is a well-recognized risk factor associated with the development of the disease, and as populations in developing countries continue to age, an anticipated growth in the number of cases is expected.Citation32,Citation33 We think that an aging effect has been operative in the studied regions and is reflected in the trend of increasing age among infected cases.
A comparison of the proportion of patients represented by each occupation indicated that in the study, rate of candidemia after cardiac surgery in housewives was the highest. Housewives are, of course, commonly gender-specific occupations, and housewives are presumably at increased risk. The reasons why candidemia is so frequent in housewives are not known, but could be presumably related to low rate of physical activity in women. In addition, women was probably due to the cultural habits of the area, whereby are obliged to be home more than men, and their act of moving are less or very less.
Coronary Artery Bypass Graft (CABG) was the most common type of surgical intervention among candidemic patients and was performed in 381 (89.86%) patients (p < .001). Mitral Valve Repair (MVR) was performed in thirty-seven patients (8.73%), and only 1.41%% of cases underwent Atrial Septal Defect (ASD) closure. As in the present study, Baddley et al.Citation20 also reported that CABG and prosthetic valve were significantly more common in Candida patients. An increase in previous CABG among Candida patients could be explained by CABG being performed in association with prosthetic valve surgery.Citation20 There were few differences in hospitalization among candidemia cases who had a heart surgery procedure, since the mean hospital stays for type of the surgical procedures were no statistical difference.
The increase in hospital-acquired candidemia cases in general is consistent with recent data describing Candida spp. as an emerging nosocomial bloodstream pathogen over the past decade.Citation20 In our study, the mean total hospital stay among candidemia cases after cardiac surgery was 17.34 ± 4.69 days. Most (65.6%) of the candidemic patients required that stay in hospitals from 10 to 19 days following cardiac surgery (p < .05) and only 5.2% of them estimated hospitalization of 25 or more days of hospital stay, whereas was no statistical difference between male and female in hospital stay. Moreover, the length of hospital stay was shown to play a major role in colonization of fungi in critical care settings.Citation34
Important predisposing conditions or risk factors for candidemia have been reported in recent, extensive reviews, and the most frequently reported are previous surgery, antibiotic use, underlying heart disease, prosthetic valves, and immunocompromising conditions.Citation5,Citation11,Citation12 We found some similar comorbidities or underlying diseases and noted several distinct differences among candidemia cases.Citation21,Citation23,Citation24 In the present study, there was a significant increase in incidence of postoperative candidemia cases among patients with underlying diseases (89.2%) as compared to cases without predisposing conditions (10.8%) at the time of candidemia diagnosis. Among patients who had cardiac surgery, diabetes alone and/or with concomitant underlying diseases were the most common comorbidities among patients with candidemia (), and 94 patients (22.17%) had >1 risk factor or underlying diseases. Bassetti et al. reported 93.1% of candidemia cases had one or more predisposing conditions, 46% had undergone a surgical intervention, 30% had a solid tumor, 28.8% had cardiovascular diseases, 25.3% were diabetic, 6.3% had hematological malignancies, 3.4% received a solid organ transplantation, and 2% had human immunodeficiency virus (HIV) infection.Citation21 Ellis et al. (2001) in one review of fungal endocarditis found that fifty-six (21%) of 270 patients had 1 risk factor; 77 (29%) had 2 risk factors; 75 (28%) had 3; and 56 (21%) had 4–7.Citation24 The present data showed that confirmed candidemia cases with cardiac surgery in the region had hospital stay fluctuations due to comorbidities or underlying diseases, but there was no statistical difference between various comorbidities for mean hospital stay.
In conclusion, these data represent a significant decline trend for candidemia and Odds ratios in all cases cardiac-operated during the study period. Majority of candidemia cases were old ages, and a remarkable gender difference skewed towards males was observed. CABG was the most common type of surgical intervention in the candidemic patients, and diabetes were more common comorbidities or underlying diseases among candidemia cases after cardiac surgery. The survey provides preliminary baseline data for the future monitoring of the disease, and highlighting potentially important nosocomial candidemia for the development of fungal endocarditis. It is demonstrating possible trends of the disease, and also, effective programs for controlling and preventive strategies against the disease in hospitals.
Conflict of interest
None declared.
Acknowledgments
The authors thank all their colleagues who cooperated in this investigation, particularly the hospital staff who had assisted us in this study. Proteomics Research Center, Shahid Beheshti University of Medical Sciences
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 6 December 2017
References
- H.WisplinghoffT.BischoffS.M.TallentH.SeifertR.P.WenzelM.B.EdmondNosocomial bloodstream infections in US hospitals: analysis of 24179 cases from a prospective nationwide surveillance studyClin Infect Dis392004309317
- J.MorganM.I.MeltzerB.D.PlikaytisA.N.SofairS.Huie-WhiteS.WilcoxExcess mortality, hospital stay, and cost due to candidemia: a case–control study using data from population-based candidemia surveillanceInfect Control Hosp Epidemiol262005540547
- D.DiekemaS.ArbefevilleL.BoykenJ.KroegerM.PfallerThe changing epidemiology of healthcare-associated candidemia over three decadesDiagn Microbiol Infect Dis7320124548
- H.WisplinghoffJ.EbbersL.GeurtzNosocomial bloodstream infections due to Candida spp. in the USA: species distribution, clinical features and antifungal susceptibilitiesInt J Antimicrob Agents4320147881
- L.C.PierrottiL.M.BaddourFungal endocarditis, 1995–2000Chest1222002302310
- B.ParisaPost-cardiac surgery fungal endocarditisCuneytNarinSpecial Topics in Cardiac Surgery2012InTech ISBN: 978-953-51-0148-2. Available from:http://www.intechopen.com/books/special-topics-in-cardiac-surgery/post-cardiac-surgery-fungal-endocarditis
- A.KaloterakisI.RizosG.GoumasIsolated native tricuspid valve Candida endocarditis in a Non-drug-addicted patient: case report and review of the literatureJ Heart Valve Dis122003652658
- D.L.HornJ.A.FishmanW.J.SteinbachPresentation of the PATH Alliance registry for prospective data collection and analysis of the epidemiology, therapy, and outcomes of invasive fungal infectionsDiagn Microbiol Infect Dis592007407414
- L.R.AsmundsdóttirH.ErlendsdóttirM.GottfredssonIncreasing incidence of candidemia: results from a 20-year nationwide study in IcelandJ Clin Microbiol4200234893492
- O.MarchettiJ.BilleU.FluckigerEpidemiology of candidaemia in Swiss tertiary care hospitals: secular trends, 1991–2000Clin Infect Dis382004311320
- A.ShorrY.TabakR.JohannesCandidemia on presentation to the hospital: development and validation of a risk scoreCritical Care132009R156
- J.-E.BerdalR.HaagensenT.RanheimJ.V.BjørnholtNosocomial Candidemia; Risk factors and prognosis revisited; 11 years experience from a Norwegian Secondary HospitalPLoS ONE972014e103916
- N.A.AhmadiM.HamidiA retrospective analysis of human cystic echinococcosis in Hamedan province, an endemic region of IranAnn Trop Med Parasitol1022008603609
- N.A.AhmadiF.BadiDiagnostic, surgical and medicinal approaches of human cystic echinococcosis: a review of 203 cases in Tehran, IranInfect Dis Clin Pract202012390393
- WHO, world alliance for patient safety. WHO Guidelines on Hand Hygiene in Health Care WHO/EIP/SPO/QPS/05.2; 2005.
- O.LyytikäinenM.KanervaN.AgtheT.MöttönenP.RuutuHealthcare-associated infections in Finnish acute care hospitals: a national prevalence survey, 2005J Hosp Infect692008288294
- M.AskarianR.S.HosseiniP.KheirandishZ.A.MemishIncidence of urinary tract and bloodstream infections in Ghotbeddin Burn Center, Shiraz 2000–2001Burns292003455459
- S.LahsaeizadehH.JafariM.AskarianHealthcare-associated infection in Shiraz, Iran 2004–2005J Hosp Infect692008283287
- G.S.MartinD.M.ManninoS.EatonM.MossThe epidemiology of sepsis in the United States from 1979 through 2000N Engl J Med348200315461554
- J.W.BaddleyD.K.BenjaminM.PatelCandida infective endocarditisEur J Clin Microbiol Infect Dis272008519529
- M.BassettiM.MerelliE.RighiEpidemiology, species distribution, antifungal susceptibility, and outcome of candidemia across five sites in Italy and SpainJ Clin Microbiol5112201341674172
- D.PaseroF.G.De RosabN.K.RanaaCandidemia after cardiac surgery in the intensive care unit: an observational studyInteract Cardiovasc Thorac Surg122011374378
- E.GirãoA.S.LevinM.BassoSeven-year trend analysis of nosocomial candidemia and antifungal (fluconazole and caspofungin) use in Intensive Care Units at a Brazilian University HospitalMed Mycol4662008581588
- M.E.EllisH.Al-AbdelyA.SandridgeW.GreerW.VenturaFungal endocarditis: evidence in the world literature, 1965–1995Clin Infect Dis3220015062
- J.NormandA.BozioJ.EtienneF.SassolasH.Le BrisChanging patterns and prognosis of infective endocarditis in childhoodEur Heart J16Suppl B19952831
- A.VossJ.A.J.W.KluytmansJ.G.M.KoelemanOccurrence of yeast bloodstream infections between 1987 and 1995 in five Dutch university hospitalsEur J Clin Microbiol Infect Dis151996909912
- A.M.TortoranoA.PrigitanoC.LazzariniA 1-year prospective survey of candidemia in Italy and changing epidemiology over one decadeInfection412013655662
- A.S.OmraniE.A.MakkawyK.BaigTen-year review of invasive Candida infections in a tertiary care center in Saudi ArabiaSaudi Med J3582014821826
- I.M.HiiH.L.ChangL.C.LinChanging epidemiology of candidemia in a medical center in middle TaiwanJ Microbiol Immunol Infect482015306315
- J.EricssonE.ChryssanthouL.KlingsporCandidaemia in Sweden: a nationwide prospective observational surveyClin Microbiol Infect192013E218E221
- M.BassettiM.MerelliF.AnsaldiClinical and therapeutic aspects of candidemia: a five year single centre studyPLoS ONE1052015e0127534
- E.Durante-MangoniS.BradleyC.Selton-SutyCurrent features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort StudyArch Intern Med168200820952103
- D.D.Correa de SaI.M.TleyjehN.S.AnavekarEpidemiological trends of infective endocarditis: a population-based study in Olmsted County, MinnesotaMayo Clin Proc8552010422426
- P.KordbachehF.ZainiF.KamaliK.AnsariM.SafaraStudy on the sources of nosocomial fungal infections at intensive care unit and transplant wards at a teaching hospital in TehranIranian J Publ Health34200518