
Abstract
Nodular hidradenoma is a rare benign skin adnexial lesion of the breast. It is often located in the nipple areolar region and presents as a slow growing painless lesion.
We report a case in a 62 yr old male who had a slowly growing left breast lesion of 10 yrs duration. Physical examination revealed an 8 cm superficial, spherical, mobile non tender lump in the nipple areolar region. Excision biopsy with clear margins was performed and histologic examination was nodular hidradenoma after wide consultations.
Nodular hidradenoma of the breast is a differential diagnosis of sub areolar masses that must be considered by both pathologist and surgeons to avoid misdiagnosis and overtreatment.
1 Introduction
Nodular hidradenoma is an established entity as a skin adnexial tumour arising from the eccrine sweat glands.Citation1 It is still a very rare benign skin adnexial lesion.Citation2 Literature review as at 2011, reported only 25 cases of the tumour.Citation1 Nodular hidradenoma is also known as clear cell hidradenoma, eccrine acrospiroma and solid cystic hidradenoma. The common locations include face, upper extremities, axilla, trunk, thigh, scalp and pubic region.Citation3 Rarely, it has been reported in the breast at the nipple areolar region and is slightly more common in women than men.Citation3 It often presents as a slow growing painless breast lump although, there are reported cases of pain, nipple discharge and ulceration of the overlying skin.Citation4
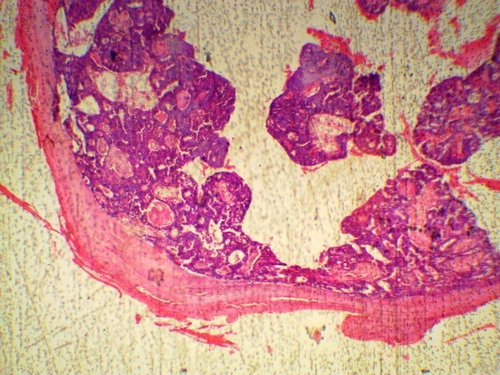
Fig. 2 X40. Showing thickened wall of the cyst, pseudopapillae and ducts containing eosinophilic decapitation secretion.
2 Case report
The patient is a 62-year-old male who lived in Ghana for several years. He was seen in the surgical outpatient clinic with a 10-year history of unilateral painless left breast enlargement which was not preceded by trauma and is without breast discharge. No history of night sweat, cough or fever. No features suggestive of malignancy. He requested for the surgical removal of the enlarged left breast mass for cultural and aesthetic reasons.
Physical examination revealed a spherical, mobile, non-tender lump of 8 cm diameter in the left breast. The right breast was normal. There is no nipple discharge and no axillary lymph node enlargement. His pulse rate was 80 beats per minute and blood pressure 130/80 mmHg. His thyroid gland was not clinically enlarged and no ophthalmopathy. He had normal androgenic hair distribution with normal genitalia and no evidence of chronic liver disease or hypogonadism. His body mass index (BMI) was 28.45.
He was counseled on the nature of the surgical operation, consent for the procedure was obtained and routine pre op tests carried out were within normal limits. Intra-operative finding was that of a spherical cystic mass which was located superficially around the nipple areolar complex, it was easily and completely excised by blunt dissection. The patient was discharged the next day. Post-operative course was unremarkable. He has remained healthy on his clinic visits within the last one and half year (see –).
Fig. 1 Dissected gross specimen of cystic mass and content from right breast.

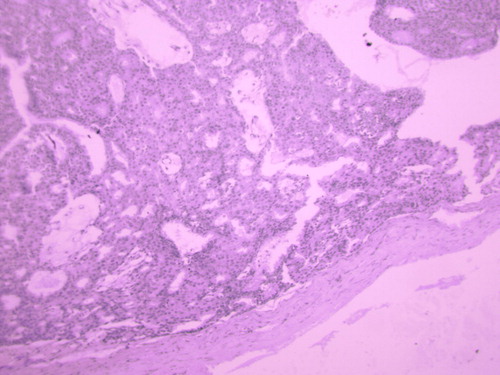
Fig. 3 X100 Periodic Acid Schiff Stain (PAS), showing decapitation secretions and lining epithelial cells containing glycogen.
At gross pathologic examination, a cystic oval shaped formalin fixed specimen was received. It measures 6 cm in diameter, weighing 16 g, cut surface revealed a unilocular cystic cavity containing grayish semisolid substance. No papillary in growth or definite solid area was seen.
Microscopically, the sections consist of mainly cystic areas lined by cuboidal to columnar epithelium some containing eosinophilic decapitation secretion. The solid areas are very scanty with pseudopapillary growth in places, there are round to oval cells with round nuclei few having clear pink cytoplasm. Other cells aggregate to form squamous spherules; there are no atypical cells. Periodic acid Schiff (PAS) stain carried out reveal presence of glycogen in the decapitation secretion and clear cells lining the cystic cavities.
3 Discussion
Nodular hidradenoma situated in the breast is very rare and it usually occurs in the nipple areolar area as one of the differentials diagnosis of breast neoplasms.Citation1 When fine needle aspiration cytology (FNAC) is performed, cytological features are often inconclusive and as such it is rarely encountered in literature review of case reports.Citation1,Citation5 Nodular hidradenoma can be either superficial or deep within the breast. When it is deep, it is often located close to mammary ducts with extensions that mimic breast cancer.Citation2 It has been reported that nodular hidradenoma can mimic conventional type renal cell carcinoma.Citation6 This is not surprising as part of the consultation leading to the diagnosis of this tumour was diagnosis of papillary carcinoma by four pathologists. The patient on follow up has remained symptoms free in the last 2 yrs and as the time of writing this article. It is possible that the complete excision of the tumour with clear margins could have accounted for lack of recurrence of the tumour. Eventhough, Orsaria and Mariuzzi have reported a case of recurrent eccrine hidradenoma in a male breast.Citation7
Immunohistochemical studies can aid in distinguishing this tumour; for example PAS diastase resistance can be demonstrated in the materials within the clear cells and eosinophilic secretions in the lumen of the cyst. Other techniques used in making a diagnosis in difficult cases include lack of reaction for estrogen and progesterone receptors, negativity for smooth muscle actin (SMA) and endoplasmic reticulum. Both epithelial membrane antigen and S-100 protein are strongly positive, while gross cystic disease fluid protein-15 is weakly positive.Citation1,Citation2 Detailed clinical history, physical findings, and ancillary studies are essential for correct diagnosis and categorization of these tumours.Citation6
4 Conclusion
Skin adnexal tumour located in the breast is unusual and is one of the differential diagnoses for subareolar breast nodules. It must be considered by surgeons and pathologist to avoid misdiagnosis and over treatment.
Conflict of interest
Authors have declared that there is no conflict of interests.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 4 May 2018
References
- V.U.GrampurohitU.DineshR.RaoNodular hidradenoma of male breast: cytohistological correlationJ Cytol2842011235237
- H.DomotoS.TerahataK.SatoS.TamaiNodular hidradenoma of the breast: report of two cases with literature reviewPathol Int48111998907911
- S.SehgalP.GoyalS.GhoshD.MittalA.KumarS.SinghClear cell hidradenoma of breast mimicking atypical breast lesion: a diagnostic pitfall in breast cytologyRare Tumours6220145343 doi: 104081/rt2014.5343
- D.G.MoteT.RamamurtiBabu B.NaveemNodular hidradenoma of the breastIndian J Surg7120094345
- Y.OhiY.UmekitaY.RaiClear cell hidradenoma of the breast: a case report with review of literatureBreast Cancer1432007307311
- K.E.VolmarT.J.CummingsW.H.WangA.J.CreagerD.S.TylerH.B.XieClear cell hidradenoma: a mimic of metastatic clear cell tumorsArch Pathol Lab Med12952005113116
- M.OrsariaL.MariuzziRecurrent eccrine hidradenoma of the breast in a male patient: problems in differential diagnosisOur Dermatol422013215