
Abstract
Objective:
To determine the incidence, mechanism of injury, wounding pattern and surgical management of urethral and penile injuries sustained in civil violence during the Iraq war.
Patients and methods:
In all, 2800 casualties with penetrating trauma to the abdomen and pelvis were received at the Al-Yarmouk Hospital, Baghdad, from January 2004 to June 2008. Of these casualties 504 (18%) had genitourinary trauma, including 45 (8.9%) with urethral and/or penile injuries.
Results:
Of 45 patients, 29 (64%) were civilians and 16 (36%) were Iraqi military personnel. The injury was caused by an improvised explosive device (IED) in 25 (56%) patients and by individual firearms in 20 (44%). Of the patients, 24 had penile injuries, 15 had an injury to the bulbar urethra and six had an injury to the posterior urethra. Anterior urethral injuries were managed by primary repair, while posterior urethral injuries were managed by primary realignment in five patients and by a suprapubic cystostomy alone in one. An associated injury to major blood vessels was the cause of death in eight of nine patients who died soon after surgery (P < 0.001).
Conclusion:
Urethral and penile injuries were caused by IEDs and individual firearms with a similar frequency. Most of the casualties were civilians and a minority were military personnel. Injuries to the anterior urethra can be managed by primary repair, while injuries to the posterior urethra can be managed by primary realignment. An associated trauma to major blood vessels was the leading cause of death in these casualties.
Abbreviations:
Introduction
Trauma to the urethra in war situations is much less common and seldom fatal compared to chest or abdominal wounds. In fact, associated non-urological injuries are usually the more obvious, and often the most life-threatening, dictating priority treatment [Citation1–Citation3]. However, urethral injury can disable injured survivors for the rest of their lives, as it has a tremendous potential for creating serious urological ‘cripples’, including the well-known triad of stricture, incontinence and impotence [Citation4]. Reports on genitourinary (GU) trauma during the Iraqi conflict have been limited to combat injuries amongst Coalition troops [Citation5–Citation7]. However, urban civil violence has been raging throughout the country since the beginning of the war in March 2003, and became a living hell for most of its population. Civil violence in Iraq reached an endemic level during the 4 years from 2004 to 2008, and civilians were daily exposed to violent acts in the streets and markets, or even in their houses. We sought to characterise the incidence, mechanism of injury, wounding pattern and surgical management of urethral and penile injuries sustained in civil violence during the Iraqi war. To our knowledge, this study is the first comprehensive report of urethral and penile trauma sustained in civil violence during the Iraq conflict.
Patients and methods
In all, 2800 casualties with penetrating trauma to the abdomen and pelvis were received at Al-Yarmouk Hospital (the teaching hospital of Al-Mustansiriya College of Medicine, Baghdad) from January 2004 to June 2008. On arrival at the hospital, the new casualty underwent prompt resuscitation, with control of shock and an evaluation of the injuries. Most of the cases had immediate surgical exploration by the hospital surgical team and, in the presence of GU injury, the management was at the discretion of the attending urologist. Of the 2800 casualties 504 (18%) had GU trauma, including 45 (8.9%) with urethral and/or penile injuries who were the subjects of this study.
Patient data were collected prospectively and analysed retrospectively. We examined patient records for age, whether they were civilians or military, the cause of injury (explosive device or individual firearm), the site of injury or injuries, associated injured organs, the type of surgical treatment and the outcome. Also, penile injuries were scored according to the organ injury severity scales of the American Association for the Surgery of Trauma [Citation8]. In most of the patients a thorough preoperative evaluation was precluded by the urgent intervention of concomitant injuries to other organs. A postoperative follow-up for a sufficient time was not possible in many patients because of the difficult and dangerous situation in Iraq during the study period. The results were analysed statistically using the Pearson chi-squared test, with significance considered at P < 0.05.
Results
The results are summarised in . All patients were male with a median (range) age of 29 (14–55) years. Young adults, 20–39 years old, were the most common victims (35 patients, 78%). Of 45 patients with urethral and/or penile injuries 29 (64%) were civilians and 16 (36%) were Iraqi military personnel. Data on the number of military personnel who were wearing body armour at the time of injury were not available. The injury was caused by improvised explosive devices (IEDs) in 25 (56%) patients and by individual firearms in 20 (44%). The IEDs included car bombs and road-side bombs (14 and 11 cases, respectively), while individual firearms included US M16 A2 and Russian AK-47 automatic rifles and pistols.
Table 1 Causes, type of patients, associated injuries and outcome in 45 patients with urethral and/or penile injuries during civil violence in Baghdad, 2004–2008.
Of the patients, 24 had penile injuries, 15 had injury to the bulbar urethra and six had injury to the posterior urethra (). Most of the penile injuries were not associated with urethral rupture, which was found in only seven cases. Of the 24 penile injuries, 19 (79%) were of grade 3 according to the severity scale, two (8%) were grade 4 and three (13%) were grade 5. Injury to the bulbar urethra was in the form of a complete rupture in 11 cases and partial rupture in four, while injury to the posterior urethra was in the form of complete rupture in all six cases.
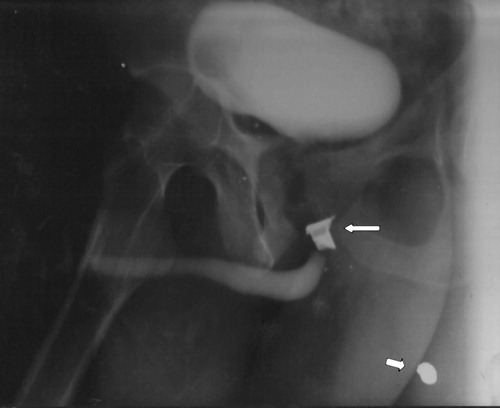
Figure 1 An ‘up-and-down’ urethrogram showing a bullet fragment (arrow) retained in the region of posterior urethral disruption. The proximal urethral segment was not filled by contrast medium in this film.
Penile wounds were repaired, after debridement of obviously necrotic tissue, by suturing the tunica albuginea and approximation of Buck’s fascia. After closing the penile skin, a Foley catheter was fixed, an elastic pressure dressing was applied and the penis was then taped to the lower abdomen. Total penectomy was resorted to in three cases with grade 5 penile injury. Injury to the penile and bulbar urethra was repaired by direct suturing or resection and anastomosis, with urethral catheter drainage for 2–3 weeks. Injury to the posterior urethra was managed by primary realignment in five patients and by a suprapubic cystostomy alone in one. Of the 21 patients with bulboprostatic urethral injury five (24%) died as a result of associated injury, seven (33%) had successful outcomes (no urinary symptoms and free urethral passage, as shown by urethrography) and nine (43%) developed urethral strictures or distraction defects. Of the patients with urethral strictures/distraction defects two were corrected by perineal repair at the Al-Yarmouk hospital and seven were referred to a high volume surgeon (M.M.K.) for a delayed repair.
The most commonly associated injury involved the scrotum and scrotal contents (27 patients, 60%); this association was more marked (92%) in penile injuries. Of the 27 patients, 19 had different grades of testicular injury and eight had only scrotal wounds. The injured testicles could be salvaged in 17 patients while the other two had a unilateral orchidectomy. Other associated injuries in this series included injuries to the bladder in 18 (40%) patients, the rectum in 20 (44%), other abdominal organs in 30 (67%), major blood vessels in eight (18%) and fractures of the pelvic bones in 21 (47%). Of the 45 casualties, nine (20%) died soon after surgery, most commonly (eight) as a result of associated major vascular injury (P < 0.001).
Discussion
Incidence
The findings of the present study show that the proportion of casualties with a GU injury was 18% of all those with abdominal and pelvic injury. This rate is almost similar to that of 22% during the American Civil War [Citation9]. Reports from other wars have compared GU injuries to all trauma admissions rather than to abdominal and pelvic cases, and thus comparison with our series is not applicable. Our findings also show that injury to the urethra accounted for 5.6% of all GU injuries. This rate is comparable to that reported from the wars in Vietnam (5.6%) [Citation1], and Croatia/Bosnia (3.5–5.3%) [Citation2,Citation10], relatively less than that of the American Civil War (7%) [Citation11], and much less than that for World War 2 (15%) [Citation2]. The present rate of penile injury (4%) is similarly less than that reported from the Croatia/Bosnia conflict (9.2–9.5%) [Citation2,Citation10], and World War 2 (18.7%) [Citation12]. These differences might be related to the different theatres of war, different types of weapons used, as well as the methods used to obtain the data.
Wounded population
The two striking differences between the Iraqi conflict and all previous wars are the high percentage of the civilian population amongst the wounded, and the high incidence of IEDs as a mechanism of injury. Owens et al. [Citation5] reported that of 3102 casualties receiving treatment for wounds sustained in the conflicts in Iraq and Afghanistan, about a third (31%) were classified as non-battle injuries. As expected, non-battle street-related violence would involve a higher proportion of civilians, reaching about two-thirds (64%) in the current series. Notably, 69% of casualties with penile and anterior urethral injuries were civilians and 31% were military personnel, while 67% of casualties with posterior urethral injury were military and 33% were civilians.
Mechanism of injury
The cause of injury can be categorised as by individual firearms (high velocity US M16 and Russian AK-47 automatic rifles, and low velocity handgun/pistol) or an IED. Wounding is a complex situation with variables of bullet size, velocity, shape, spin, distance from muzzle to target, and nature of the tissue affected. For example, a bullet striking bone might cause fragmentation of the bone and/or bullet, forming numerous secondary missiles, each producing additional injury (). Also, the distance of the target from the muzzle plays a large role in wounding capacity, for most bullets fired from handguns loose significant kinetic energy at 100 m, while high-velocity military rifles deliver bullets that still have considerable kinetic energy even at 500 m.
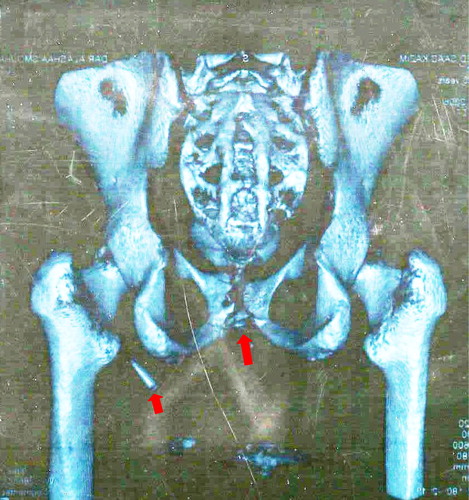
Figure 2 A cystogram after filling the bladder from a suprapubic catheter showing multiple bullet fragments inside the pelvis and perineum. The patient had been shot by a high velocity US M16 automatic rifle from a distance of ≈3 m. The bullet fragments resulted in testicular injury, disruption of the posterior urethra, injury to the rectum and fracture of the coccyx.
IEDs can be classified as roadside explosives and blast mines, explosive-formed projectiles devices, car bombs and suicide bombings [Citation13]. These devices range from rudimentary home-made explosives to sophisticated weapon systems containing high-grade explosives. Injuries from IEDs follow an ‘all or none’ pattern; casualties either die from catastrophic polytrauma resulting from direct impact, or sustain relatively minor injuries as a result of the associated indirect energy dissipation [Citation14]. Bala et al. [Citation15] found that the median injury severity score in casualties from an IED was significantly higher than from gunshot wounds (34 and 18, respectively, P < 0.001) and that injury to multiple body regions (three or more) occurred in 86% and 29% of IED and gunshot victims, respectively (P < 0.001). Briefly, IEDs generate more severe injuries to more body regions than individual firearms.
The mechanism of injury is a key difference amongst various conflicts during the past 150 years. In the American Civil War, urethral injuries were primarily (94%) caused by bullets [Citation9]. This high rate of injuries by bullets gradually decreased in subsequent conflicts to reach 58% in Vietnam, 47% in Bosnia, 30% in Croatia and 18–35% in combat injuries in Iraq [Citation1,Citation2,Citation6,Citation7,Citation10]. In the present series, urethral and penile injuries were inflicted by individual firearms in 44% of cases and by IEDs in 56%. In the largest report of GU injuries during any military conflict, Serkin et al. [Citation7] found that 65% of 819 casualties (90% were sustained in Iraq) were because of explosions. Also, Belmont et al. [Citation16] found that explosive injury mechanisms accounted for 75% of all combat casualties from 2005 to 2009. Indeed, the IED has become synonymous with the conflict in Iraq, as it was widely used by the insurgents and was the leading cause of injury and death amongst civilians and coalition troops.
Associated injuries
Reports from previous wars show that associated injuries occurred in 70–93% of the urogenitally wounded combatants, with the abdomen, chest and extremities being the most common sites [Citation2,Citation10,Citation17]. Associated non-urological injuries are usually the most life-threatening, dictating priority treatment, even before a full investigation of the GU injury. The current study shows that the most commonly associated injury involved the scrotum and scrotal contents. This association was particularly prevalent in penile injuries (). Also, the present study shows that although trauma to major blood vessels was not a common associated injury, it was the leading cause of death in these casualties (eight of the nine cases). It has been noted that in injuries to the posterior urethra, the projectile usually follows a path through the gluteal muscles and pelvis, while in injuries to the anterior urethra a perineal genital path is usually found [Citation18]. This might explain the frequency of associated vascular and colorectal lesions in pelvic wounds and genital injuries in perineal wounds.
Anatomical pattern of wounding
The anatomical pattern of wounding has changed over several conflicts during the past 100 years. This would be expected considering the development of weapons and the different types of warfare, i.e., from the trench battlefields of World War l to the mobile battle fields of World War 2, to the jungles of Vietnam and to the urban-type warfare of Iraq. For example, the shift of trench battlefields to mobile battlefields resulted in a greater percentage of injuries to the lower extremities and external genitalia in World War 2 [Citation19]. Also, the wounding pattern in the Iraqi conflict had notable differences from the patterns in previous conflicts. There was a greater proportion of head and neck wounds than in World War 2, and the Korea and Vietnam wars (30% vs. 16–21%, P < 0.001), and a lower proportion of thoracic wounds than in World War 2 and Vietnam (6% vs. 13%, P < 0.001) [Citation5]. Notably, this study shows that penile injuries were caused by IEDs in 67% of patients and by individual arms in 33%, while injuries to the posterior urethra were caused by IEDs in only 17% and by individual firearms in 83% (). It seems that injury to the posterior urethra, given its protected position inside the pelvis, requires a high-velocity firearm rather than an IED, which tends to produce more superficial injuries [Citation20], such as those of the penis and anterior urethra.
The value of body armour, which has led to changes away from abdominal injuries, has been reported by several investigators. Paquette [Citation6] noted a significant reduction in overall GU injuries and specifically kidney injuries in those casualties wearing body armour. Also, Patel et al. [Citation18] noted a significantly greater percentage of abdominal wounds in Iraqi prisoners of war than in USA combatants (21% vs. 3%, respectively, P < 0.05); none of the Iraqi wounded were wearing body armour. Also, new developments in body armour technology, with the addition of a groin protector, should decrease the incidence of genital wounds [Citation3].
Surgical treatment
In a combat setting, urethral and penile injuries are usually associated with more serious injuries to other organs, dictating priority treatment. The best approach to wound care is conservative. With simple punctures and no apparent tissue disruption, just irrigation and application of a dressing might suffice. Treatment guidelines include debridement of devitalised tissues when greater tissue disruption is apparent. In some wounds, it can be difficult to determine the extent of disruption and the amount of nonviable tissue. In such cases, the use of duplex Doppler ultrasonography can aid in determining the extent of vascular injury; otherwise, the injury can be reassessed after 48 h [Citation21]. In short ‘treat the wound, not the weapon’. Bullets are not sterile and might have encountered intermediate targets such as clothing before entering the body [Citation22]. Also, skin particles serve as a transport vehicle for pathogens [Citation23]. In addition, the pressure difference from atmospheric pressure to a bullet track might allow air to sweep debris inward, causing contamination of the wound [Citation24]. Thus, antibiotic prophylaxis is recommended in gunshot injuries.
The most common surgical procedure adopted in this series was debridement and the repair of injuries to the external genitalia. For injuries of the penile and bulbar urethra, primary repair can be suggested for most cases. Injuries to the posterior urethra can be managed by primary realignment for haemodynamically stable patients. A suprapubic cystostomy alone and delayed repair might be the best option for unstable patients, or when an experienced urologist is unavailable.
In conclusion, urethral and penile injuries sustained in civil violence during the Iraqi conflict constituted 8.9% of GU trauma. About two-thirds of casualties were civilians and a third were military personnel. The injury was caused by IEDs in 56% of the cases and by individual firearms in 46%. The most commonly associated injury involved the scrotum and scrotal contents. Injury to the anterior urethra can be managed by primary repair, and injuries to the posterior urethra can be managed by primary realignment in stable patients and by a suprapubic cystostomy alone in critically unstable patients. Trauma to major blood vessels, regardless of its rare incidence as an associated injury, was the leading cause of death in these casualties.
Conflict of interest
None.
Funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- O.SalvatierraJrW.O.RigdonD.M.NorrisT.W.BradyVietnam experience with 252 urological war injuriesJ Urol1011969615620
- A.TucakT.LukacevikH.KuvezdicZ.PetekR.NovakUrogenital wounds during the war in Croatia in 1991/1992J Urol1531995121122
- S.J.HudakA.F.MoreyT.A.RozanskiC.W.FoxJr.Battlefield urogenital injuries: changing patterns during the past centuryUrology65200510411046
- M.M.KoraitimPelvic fracture urethral injuries: the unresolved controversyJ Urol161199914331440
- B.D.OwensJ.F.KraghJrJ.C.WenkeJ.MacaitisC.E.WadeJ.B.HolcombCombat wounds in operation Iraqi Freedom and operation Enduring FreedomJ Trauma642008295299
- E.L.PaquetteGenitourinary trauma at a combat support hospital during operation Iraqi Freedom. The impact of body armorJ Urol177200721962199
- F.B.SerkinD.W.SoderdahlJ.HernandezM.PattersonL.BlackbourneC.E.WadeCombat urologic trauma in US military overseas contingency operationsJ Trauma69Suppl. 12010175178
- A.M.MohrA.M.PhamR.F.LaveryZ.SifriV.BargmanD.H.LivingstonManagement of trauma to the male external genitalia: the usefulness of American Association for the surgery of trauma organ injury scalesJ Urol170200323112315
- H.W.HerrUrological injuries in the Civil WarJ Urol172200418001804
- T.HudolinI.HudolinSurgical management of urogenital injuries at a war hospital in Bosnia-Herzegovina in 1992–95J Urol169200313571359
- H.W.HerrJ.W.McAninchUrethral injuries in the Civil WarJ Urol173200510901093
- D.F.MarshallUrogenital wounds in an evacuation hospitalJ Urol551946119132
- A.RamasamyS.HarrissonI.LasradoM.P.StewartA review of casualties during the Iraqi insurgency in 2006 — a British field hospital experienceInjury402009493497
- A.RamasamyS.HarrissonJ.C.ClasperM.P.StewartInjuries from roadside improvised explosive devicesJ Trauma652008910914
- M.BalaA.I.RivkindG.ZamirT.HadarI.GertsenshteinY.Mintzet alAbdominal trauma after terrorist bombing attacks exhibit a unique pattern of injuryAnn Surg2482008303309
- P.J.BelmontJr.B.J.McCriskinR.N.SiegR.BurksA.J.SchoenfeldCombat wounds in Iraq and Afghanistan from 2005 to 2009J Trauma Acute Care Surg732012312
- T.G.OchsnerF.M.BuschB.G.ClarkeUrogenital wounds in VietnamJ Urol1011969224225
- T.H.PatelK.A.WennerS.A.PriceM.A.WeberA.LeveridgeS.J.McAteeA US Army Forward Surgical Team’s experience in operation Iraqi FreedomJ Trauma572004201207
- J.C.KimbroughWar wounds of the urogenital tractJ Urol551946179189
- B.A.GeorgiM.MassadM.ObeidBallistic trauma to the abdomen: shell fragments versus bulletsJ Trauma311991711716
- M.L.FacklerCivilian gunshot wounds and ballistics: dispelling the mythsEmerg Med Clin North Am1619981728
- R.A.SantucciY.-J.ChangBallistics for physicians: myths about wound ballistics and gunshot injuriesJ Urol171200414081414
- M.G.PerdekampB.P.KneubuehlA.SerrB.VennemannS.PollakGunshot-related transport of micro-organisms from the skin of the entrance region into the bullet pathInt J Legal Med1202006257264
- R.JandialB.ReichwageM.LevyV.DuenasL.SturdivanBallistics for the neurosurgeonNeurosurgery622008472480