
Abstract
Objective:
To assess the benefit of a new technique of a Plastibell circumcision supported by a ventral calcium-alginate fibre dressing, to reduce bleeding from the frenular vessels, the commonest complication of Plastibell circumcision.
Patients and methods:
This was a retrospective study of 200 neonates circumcised in the Royal Bahrain Hospital over a 2-year period from 2012 to 2014. They had a standard Plastibell circumcision, but a calcium-alginate fibre dressing (Hypo-sorb, Plastod, Italy) was placed over the glans and under the foreskin, to help control bleeding from the frenular vessels.
Results:
Circumcision using the calcium-alginate fibre dressing reduced the bleeding complication rate to zero. The delayed separation of the bell was 2.9% when using the new technique and 2.5% from our previous data. There were no cases of urinary retention reported, compared to two in the previous results.
Conclusion:
A Plastibell circumcision supported by the calcium-alginate fibre dressing was a safe technique to reduce bleeding.
Introduction
World-wide, circumcision is one of the commonest surgical procedures in the neonatal period. The vast majority of neonatal circumcisions are done for religious or cultural reasons. The advantages and disadvantages of neonatal circumcision remain a matter of debate [Citation1]. The main medical benefit of circumcision is considered to be the reduction in relative risk of UTI during infancy. Six UTIs can be prevented for every complication endured, and almost two complications can be expected for every case of penile cancer prevented [Citation2]. Currently, the Plastibell method is frequently used for neonatal circumcision, as it is quicker and has fewer late complications [Citation3–Citation5]. The common complications reported with Plastibell circumcision are problems with the ring (3.6%), and bleeding (3%). Here we analyse a new technique which can reduce bleeding-related complications and give the best cosmetic results.
Patients and methods
After obtaining approval from the local ethics committee, we retrospectively analysed the results of 200 neonatal circumcisions at the Royal Bahrain Hospital between 2013 and 2014, for which we used a new technique in which the Plastibell circumcision was supported by a ventral calcium-alginate fibre dressing. The mean (SD, range) age of the patients was 5.85 (1–30) days.
Procedure
The neonates were not fed for 2 h before circumcision. After placing an infant on a circumcision-restraint board, the skin was prepared with a povidone–iodine (10%) solution. A dorsal nerve block was administered using 0.2 mL/kg of 2% lidocaine, with a 27-G needle, and a delay of 3 min allowed before starting the procedure (). The first step was to hold the prepuce between two haemostatic forceps to either side of the midline, and make a compressed skin line by crushing with another haemostatic forceps. A dorsal slit was then made through the compressed skin line (). The prepuce was pulled back and cleaned using the povidone–iodine solution. The entire prepuce, sulcus and frenular attachment was examined (). Retraction of the prepuce will rupture the frenulum, causing bleeding, if the frenular attachment is closer to the urethral meatus. Bleeding over the frenular area was assessed and a small compression applied for some time. A Plastibell with a calcium-alginate fibre dressing on the ventral aspect (Hypo-sorb, Plastod, Italy) was placed over the glans and under the foreskin (). This helps to control the bleeding from the frenular vessels. The prepuce is then returned to its anatomical position. The bell is held in position between the haemostat forceps by an assistant. A silk suture is tied around the entire foreskin, which will fall off (after necrosis) within several days (). The excess skin over the bell is excised using scissors (). The parents of the patients were informed to return if the interval before bell separation was >10 days. However, there was no further intervention unless the bell remained for >15 days.
Figure 1 (A) A dorsal nerve block dorsal is applied. (B) A slit is made through a compressed skin line. (C) The prepuce is retracted and the frenular area examined. (D) The alginate dressing is placed inside the ventral aspect of the bell. (E) The silk suture is positioned and tied. (F) The excess skin over the bell is removed.
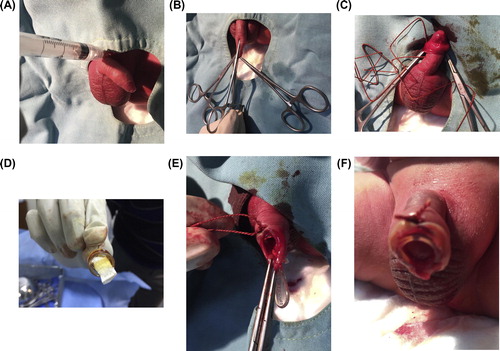
The ventral dressing is a sterile non-adhesive advanced wound dressing formed by a soft and conformable net of pure calcium-alginate microfibres. The highly hydrophilic fibres swell during the absorption of exudate, forming a firm gel which fills the wound without adhesion to it.
The patient is advised to apply mupirocin cream to the wound two to three times daily until the bell falls off. The bell, along with dressing, usually falls within 4–10 days.
Results
This method of circumcision was associated with no bleeding complications, whereas previously in our department the commonest complication associated with Plastibell circumcision was bleeding from the frenular vessels, occurring in 5% of circumcisions during 2011–2012. The rate of delayed separation or migration of the bell was 2.9% in the present study, compared to 2.5% in our previous data. There were no cases of urinary retention, compared to two previously.
Discussion
Routine circumcision is becoming more acceptable world-wide, and according to numerous studies the Plastibell technique is considered to be the safest procedure for neonatal circumcision, with overall complications being very rare. Many of the studies show that the Plastibell method is an acceptable option for circumcision even up to middle childhood. The common reported complications include haemorrhage, infection, sepsis, meatal ulceration, a retained bell, and poor cosmetic results. During a Plastibell circumcision the complete release of adhesion of the prepuce to the glans, including the frenular area, is very important for obtaining a good cosmetic result and avoiding the complication of the bell compressing the urethral meatus. The choice of a correctly sized Plastibell is also important to avoid compression of the glands and any oedema, thus leading to difficulty in urination. The main problem that the surgeon faces is that when the prepuce is retracted properly, the risk of bleeding from the frenular vessels can be unpredictable, and if incorrectly retracted the bell can compress the urethral meatus, leading to a poor cosmetic result. If the bell is too large or too small there might be a proximal or distal dislocation.
Bleeding was a significant complication in many previous studies, with rates of 18–44% [Citation6,Citation7], and these studies showed that there was no difference in the infection rate in a Plastibell group compared to standard circumcision, with rates of 4–14% [Citation7–Citation11]. In the present study there were no reported infections requiring a hospital visit. The mean (range) time required for bell separation was 6 (4–15) days. The rate of delayed separation (>10 days) of the retained bell was 2.9%, compared to a previous rate of 2.5%, but no bell was retained for >15 days.
In conclusion, a Plastibell circumcision supported by the calcium-alginate fibre dressing is a safe modification to standard Plastibell circumcision to reduce bleeding-related complications.
Conflict of interest
None.
Source of funding
None.
Notes
Peer review under responsibility of Arab Association of Urology.
References
- V.PalitD.K.MenebhiI.TaylorM.YoungY.ElmasryT.ShahA unique service in UK delivering Plastibell circumcision. Review of 9 year resultsPediatr Surg Int2320074548
- D.A.ChristakisE.HarveyD.M.ZerrC.FeudtnerJ.A.WrightF.A.ConnellA trade-off analysis of routine newborn circumcisionPediatrics1052000246249
- I.A.FraserM.J.AllenP.F.BagshawM.JohnstoneA randomized trial to assess childhood circumcision with the Plastibell device compared to a conventional dissection techniqueBr J Surg681981593595
- Y.L.MakS.C.ChoM.W.FaiChildhood circumcision: conventional dissection or Plastibell device—a prospective randomized trialThe Hong Kong Practitioner171995101105
- J.M.Bastos NettoJ.G.de AraújoJr.M.F.de Almeida NoronhaB.R.PassosJ.de BessaJr.A.A.FigueiredoProspective randomized trial comparing dissection withJ Pediatr Urol62010572577
- S.A.MousaviE.SalehifarCircumcision complications associated with the Plastibell device and conventional dissection surgery: a trial of 586 infants of ages up to 12 monthsAdv Urol6061232008
- J.LazarusA.AlexanderH.RodeCircumcision complications associated with the Plastibell deviceSouth Afr Med J972007192193
- S.M.SörensenM.R.SörensenCircumcision with the Plastibell device. A long-term follow-upInt Urol Nephrol201988159166
- T.ShahJ.RaistrickI.TaylorM.YoungD.MenebhiR.StevensA circumcision service for religious reasonsBJU Int831999807809
- K.P.ManjiCircumcision of the young infant in a developing country using the PlastibellAnn Trop Paediatr202000101104
- J.R.HolmanE.L.LewisR.L.RinglerNeonatal circumcision techniquesAm Fam Physician521995519520