Abstract
Background
This study was designed to evaluate the preemptive analgesic efficacy of ketorolac tromethamine versus tramadol in providing postoperative pain relief and improving discharge criteria in children undergoing inguinal herniotomy.
Methods
Eighty children, aged between 2 and 12 years, undergoing inguinal herniotomy were randomly allocated to receive intravenous 1 mg/kg tramadol (group T; n = 40) or 1 mg/kg ketorolac (group K; n = 40), immediately after induction of general anesthesia.
Heart rate, arterial pressure and oxygen saturation were monitored. Postoperative pain was assessed at regular intervals until discharge. Postoperative rescue analgesic (15 paracetamol mg/kg rectally) was supplemented when pain score was >4. Time to first analgesia, requirement for additional analgesics, sedation level, bleeding time and side effects were noted.
Results
Time to first analgesia was significantly longer and total consumption of rescue analgesic was significantly lower in tramadol group compared with ketorolac group .There were no significant changes in intraoperative heart rate, and arterial pressure between groups. Intraoperative bleeding time was within normal in both groups, but it was significantly higher in the ketorolac. Adverse effects were not observed.
Conclusions
Tramadol provided longer duration of postoperative analgesia and reduced requirement for rescue analgesic compared with ketorolac in children undergoing inguinal herniotomy.
1 Introduction
Preemptive pain control remains controversial. Numerous studies have suggested a benefit from the administration of analgesic medications before surgical incision [Citation1]. Research on ideal technique, ideal drug and ideal time of application is still going on for better results in postoperative pain management [Citation2]. Adequate analgesia after inguinal hernia repair in children is essential and may be obtained through various techniques. These methods include administration of opioids, administration of non steroidal anti-inflammatory drugs and use of regional techniques [Citation3].
Tramadol, synthetic 4-phenylpiperidine analog of codeine, has an analgesic effect due to activation of mu opioid receptors and inhibition of monoamine reuptake, specifically serotonin and norepinephrine [Citation4,Citation5]. A metabolite formed following first-pass metabolism, O-desmethyltramadol (M1), possesses a higher affinity for mu opioid receptors compared to tramadol and likely contributes to its analgesic effects [Citation6]. Tramadol may be used as analgesic for day-case surgery compared with other opioids because of its side-effect profile [Citation7]. Ketorolac tromethamine is a non-steroidal anti-inflammatory drug (NSAID) that has an analgesic efficacy similar to commonly used opioids, and that recently has found wide acceptance in the treatment of postoperative pain in a variety of surgical procedures [Citation8,Citation9]. The aim of this randomized, double-blind study is to compare ketorolac versus tramadol in providing analgesia for children undergoing inguinal herniotomy.
2 Methods
After gaining institutional ethical committee approval and written informed parental consent, 80 children, ASA I or II, aged between 2 and 12 yr, who were subjected to day-case inguinal herniotomy were enrolled in a randomized, double-blind study. Exclusion criteria include known renal dysfunction, coagulopathy, or a family history of a bleeding diathesis. Patients were fasted for 6 h before the procedure with exemption of clear fluids (allowed up to 3 h before the procedure). No premedication was given.
Anesthesia was induced with thiopental 4–6 mg/kg and cisatracurium 0.09 mg/kg. After induction, patients were randomly allocated by closed envelope method to receive either tramadol (1 mg/kg i.v.) in group T or ketorolac (1 mg/kg i.v.) in group K. Both drug solutions looked identical, 3 ml volume and prepared by personnel unaware of group assignment. Anesthesia was maintained with 2% sevoflurane, in combination with 50% air in oxygen. The ventilation is adjusted to maintain an end tidal carbon dioxide (EtCO2) of 4–4.6 kPa. Sevoflurane was discontinued at the start of skin closure. Monitoring included electrocardiography, noninvasive blood pressure, pulse oximetry, and EtCO2 concentrations. An increase in blood pressure or heart rate by more than 15% from preoperative value was defined as insufficient analgesia and was treated with fentanyl 1 μ/kg.
Saline dextrose 5% (1:1) solution was infused in a dose of 12 ml/kg/h. Bleeding time was measured with the standard Ivy method. At the end of surgery, residual neuromuscular block was antagonized with neostigmine 50 μg/kg and atropine 20 μg/kg, and the trachea was extubated. No sedatives or opioids were administered during operation. After the operation, time from discontinuation of anesthesia to spontaneous eye opening and the duration of surgery were noted. Pain in the postanesthetic care unit (PACU) and day-surgery unit was assessed every hour by the trained nurse blinded to group assignment, using FLACC Scale. FLACC scale uses five criteria: Face, Legs, Activity, Cry, and Consolability. Each criterion scores from 0 to 2 to give a possible total score of 0–10. Assessments were done every hour until hospital discharge. Children were transferred from PACU to day-surgery unit (DSU) if they achieved Modified Aldrete Score [Citation10] of 10. Patients received rectal paracetamol 15 mg/kg as rescue analgesic when FLACC scale was >3which could be repeated every 4 h if Pain scale >3. Fentanyl 1 μg/kg is second rescue analgesic if FLACC scale was >3 in spite of rectal paracetamol or until next dose of paracetamol. Time for first analgesic and the total opioid consumption of analgesic in the postoperative period were recorded. Sedation level was evaluated every hour with a four-point sedation scale, 0 = eyes open spontaneously, 1 = eyes open to speech, 2 = eyes open when shaken, 3 = unrousable [Citation11]. Side effects, including vomiting, bleeding from surgical point, were reported.
The statistical analysis of data was done by using excel program and SPSS program (statistical package for social science) version 11 (SPSS Inc., Chicago, IL, USA). K–S (Kolmogorov–Smirnov) test was done to test the normality of quantitative data. The analysis of the data was done using Student's unpaired t-test. Scores for pain and sedation were analyzed using the Mann–Whitney U-test. Data were expressed as mean ± standard deviation or frequency (%), or medians (ranges). P is significant if <0.05 at confidence interval 95%.
3 Results
The two groups of children were comparable with respect to age, weight, sex and duration of surgery (). No statistically significant differences were observed between the two groups in the heart rate and mean arterial blood pressure intraoperatively ( and ).
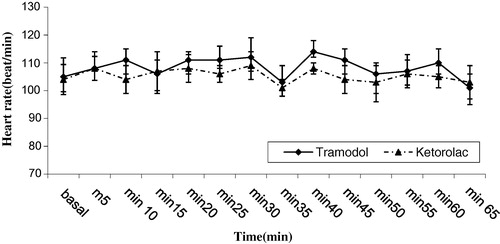
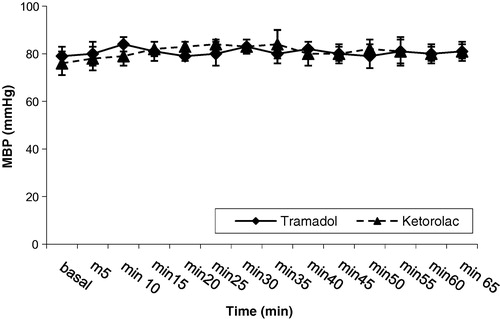
Table 1 Demographic data of patients and duration of surgery.
The time to first administration of rescue analgesia was significant earlier and total opioid consumption was significantly higher in the ketorolac group compared to the tramadol group. Also, significantly more children in the ketorolac group required postoperative analgesics compared to the tramadol group ( and ). Patients in group T had significantly less postoperative pain (). Intraoperative bleeding time was significant higher in the ketorolac group compared to the tramadol group but still within the normal limits (). Ten patients in group K required postoperative paracetamol compared with four patients in group T (). No difference in the incidence of vomiting, PACU time and DSU time were observed between the two groups. There were no ketorolac related side effects like oozing, or bleeding either intra or postoperative. No patient in either group required admission to hospital again due to pain or nausea and vomiting or bleeding at the surgical wound.
Table 2 Postoperative pain and sedation scores.
Table 3 Perioperative data.
4 Discussion
Preemptive analgesia, starting treatment before surgical stimulus, may reduce the need for postoperative analgesia [Citation12]. Preemptive analgesia is currently being used for the management of postoperative pain and is no longer actively researched [Citation9]. Postoperative pain management is one of the most important issues in the outcome of the surgery. Despite all the developments in anesthetic and regional techniques, newer drugs, drug combinations, its impact in pediatric patient groups may sometimes be under estimated due various reasons like pediatric metabolism, facility problems, pediatric limitation of certain drugs, techniques, lacking knowledge of evaluation parameters [Citation2]. Intravenous ketorolac has been shown to have preemptive analgesic effects in patients undergoing ankle fracture repair [Citation13]. Ketorolac does not improve or prolong postoperative analgesia compared to systemic administration when it was added to lidocaine infiltration for hernia repair [Citation14]. Inguinal hernia repair is one of the most painful ambulatory surgeries, with 40–50% patients reporting moderate to severe pain 24 h later [Citation15].
Our data showed that intravenous administration of tramadol 1 mg/kg at induction of anesthesia significantly reduced postoperative pain following day case herniotomy in pediatrics compared with ketorolac 1 mg/kg. In agreements with our results, Putland and McCluskey [Citation16] concluded that preemptive administration of tramadol 1.5 mg/kg at induction of anesthesia significantly reduced pain following day-case laparoscopic sterilization compared with patients who received ketorolac.
Administration of tramadol in addition to bupivacaine in caudal block for pediatric inguinal herniorrhaphy resulted in superior analgesia and less demand for additional analgesics compared with caudal bupivacaine alone without an increase of side effects [Citation17,Citation18].
In a multicenter study, Finkel et al. [Citation19], showed that oral tramadol 1–2 mg/kg is well tolerated and effective in pediatric postoperative pain. Inclusion criteria in this study include tolerability to oral intake and when their pain was manageable with PCA bolus morphine without a basal infusion.
A study comparing intravenous ketorolac versus rectal acetaminophen in pediatric patients undergoing tonsillectomy found that ketorolac (1 mg/kg) is no more effective than high-dose rectal acetaminophen (35 mg/kg) for analgesia and was associated with significantly more measures to achieve hemostasis in the patient undergoing tonsillectomy [Citation20].
A randomized study by Norman et al. [Citation13] studied the preemptive effect of intravenous ketorolac in adult undergoing ankle fracture surgery. They reported that there was no increase in pain postoperatively in patients given ketorolac before tourniquet compared with their preoperative baseline. Meanwhile, patients who received ketorolac after tourniquet inflation had significant increases in their postoperative pain compared with the preoperative baseline. Mendel et al. compared intravenous ketorolac (0.9 mg/kg) and fentanyl (1 μg/kg) in children undergoing strabismus surgery and concluded that neither ketorolac nor fentanyl was associated with less postoperative vomiting or analgesic requirements compared to saline placebo administered during pediatric strabismus surgery. They recommend avoiding fentanyl as it was associated with a significantly greater incidence of postoperative vomiting compared to ketorolac or placebo [Citation21].
On the other hand, Splinter et al. [Citation3] investigated effect of intravenous ketorolac versus caudal anesthesia for reducing pain after pediatric inguinal repair and found that 1 mg/kg intravenous ketorolac, compared to caudal anesthesia, resulted in lower pain scores and earlier ambulation after inguinal repair in children.
A comparative study of analgesic efficacy of 30 mg ketorolac versus 100 mg tramadol administered intravenously and at fixed times over the 24 h after abdominal hysterectomy in adults showed that postoperative pain scores in the tramadol group, in the first 12 h after surgery, were statistically lower than those of the ketorolac group [Citation22].
In this study, although bleeding time was significantly higher in ketorolac group compared to tramadol group, but still within normal (3–8 min) and no hemostatic measures were needed either intra or postoperatively. However, Rusy et al. [Citation20] reported that extra measures are needed to obtain hemostasis in pediatric patients undergoing tonsillectomy when ketorolac was given in a dose of 1 mg/kg. This discrepancy could be due to different type of surgery.
In conclusion, preemptive tramadol 1 mg/kg provided longer duration of postoperative analgesia and reduced requirement for rescue analgesic compared with intravenous ketorolac 1 mg/kg in children undergoing inguinal herniotomy. Further studies are needed to compare effects of ketorolac before and after surgery or combination with other non steroidal anti inflammatory drugs.
Notes
Peer review under responsibility of Egyptian Society of Anesthesiologists.
References
- S.MoinicheH.KehletJ.B.DahlA qualitative and quantitative systematic review of preemptive analgesia for postoperative pain relief: the role of timing of analgesiaAnesthesiology9632002725741
- G.Köknel TaluN.S.OzyalçinR.BalsakM.KaradenizThe efficacy of preemptive ketamine and ropivacaine in pediatric patients: a placebo controlled, double-blindAgri20220083136
- W.M.SplinterC.W.ReidD.J.RobertsJ.BassReducing pain after inguinal hernia repair in children: caudal anesthesia versus ketorolac tromethamineAnesthesiology8731997542546
- S.IdeM.MinamiK.IshiharaG.R.UhlI.SoraK.IkedaMu opioid receptor dependent and independent components in effects of tramadolNeuropharmacology512006651658
- S.GrondA.SablotzkiClinical pharmacology of tramadolClin Pharmacokinet432004879923
- C.GillenM.HaurandD.J.KobeltS.WnendtAffinity, potency and efficacy of tramadol and its metabolites at the cloned human mu-opioid receptorNaunyn-Schmiedeberg Arch Pharmacol3622000116121
- E.A.ShiptonJ.A.RoelofseR.J.BlignautAn evaluation of analgesic efficacy and clinical acceptability of intravenous tramadol as adjunct to propofol sedation for third molar surgeryAnesth Prog5032003121128
- L.G.PatrocínioO.Rangel MdeG.S.Marques MiziaraA.M.RodriguesJ.A.PatrocínioT.G.PatrocinioA comparative study between ketorolac and ketoprofen in postoperative pain after uvulopalatopharyngoplastyBraz J Otorhinolaryngol7332007339342
- J.Y.HongThe effect of preoperative ketorolac on WBC response and pain in laparoscopic surgery for endometriosisYonsei Med J4662005812817
- J.A.AldreteThe post-anesthesia recovery score revisitedJ Clin Anesth719958991
- M.R.J.SuryP.V.ColeNalbuphine combined with midazolam for outpatient sedationAnaesthesia431988285288
- I.KissinAnalgesiaAnesthesiology934200011381143
- P.H.NormanM.D.DaleyR.W.LindseyPreemptive analgesic effects of ketorolac in ankle fracture surgeryAnesthesiology942001599603
- K.J.KardashJ.GarzonA.M.VellyM.J.TesslerKetorolac analgesia for inguinal hernia repair is not improved by peripheral administrationCan J Anaesth5262005613617
- B.McGrathH.ElgendyF.ChungD.KammingB.CurtiS.KingThirty percent of patients have moderate to severe pain 24 h after ambulatory surgery: a survey of 5703 patientsCan J Anesth512004886891
- A.J.PutlandA.McCluskeyThe analgesic efficacy of tramadol versus ketorolac in day-case laparoscopic sterilisationAnaesthesia5441999382385
- A.C.SenelA.AkyolD.DohmanM.SolakCaudal bupivacaine-tramadol combination for postoperative analgesia in pediatric herniorrhaphyActa Anaesthesiol Scand4562001786789
- R.TaheriS.ShayeghiS.S.RazaviA.SadeghiK.GhabiliM.GhojazadehM.RouzrokhEfficacy of bupivacaine-neostigmine and bupivacaine-tramadol in caudal block in pediatric inguinal herniorrhaphyPaediatr Anaesth2092010866872
- J.C.FinkelJ.B.RoseM.L.SchmitzP.K.BirminghamG.A.UlmaJ.B.GunterA.CnaanC.J.CotéR.A.MedveM.S.SchreinerAn evaluation of the efficacy and tolerability of oral tramadol hydrochloride tablets for the treatment of postsurgical pain in childrenAnesth Analg946200214691473
- L.M.RusyC.S.HouckL.J.SullivanL.A.OhlmsD.T.JonesT.J.McGillC.B.BerdeA double-blind evaluation of ketorolac tromethamine versus acetaminophen in pediatric tonsillectomy: analgesia and bleedingAnesth Analg8021995226229
- H.G.MendelK.M.GuarnieriL.M.SundtM.C.TorjmanThe effects of ketorolac and fentanyl on postoperative vomiting and analgesic requirements in children undergoing strabismus surgeryAnesth Analg806199511291133
- G.Ollé FortunyL.Opisso JuliaF.Oferil RieraM.Sánchez PallarésR.Calatayud MontesaCabré Roca IKetorolac versus tramadol: comparative study of analgesic efficacy in the postoperative pain in abdominal hysterectomyRev Esp Anestesiol Reanim4742000162167