Abstract
Background
This study was designed to compare magnesium sulphate with dexmedetomidine, regarding their efficiency in inducing deliberate hypotension and providing a better surgical field exposure during middle ear surgery. It also compared the influence of their use on postoperative pain and recovery time.
Methods
Eighty-eight adult patients undergoing middle ear surgery were included. Patients were randomly divided into two equal groups. Patients were assigned to receive either magnesium sulphate (M group) or dexmedetomidine (D group). Anaesthesia was induced by propofol 2 mg/kg iv and fentanyl 1 μg/kg. Patients in the M group received an iv bolus of magnesium sulphate 50 mg/kg in a total of 100 ml saline over 10 min followed by infusion of 15 mg/kg/h until the end of surgery. Similarly, patients in the D group received dexmedetomidine 1 μg/kg over 10 min followed by 0.4–0.8 μg/kg/h until the end of operation. The target MAP during operation was between 60 and 70 mmHg. The surgeon who was blinded of the selected hypotensive agent was asked to assess the quality of the surgical field. In the postanaesthesia care unit (PACU), postoperative pain was assessed and recovery time was recorded.
Results
Both study drugs succeeded to reach the target MAP. The quality of the surgical field was not different between the two groups. Postoperative pain was not different between the two group and only eight patients in the M group and seven patients in the D group required analgesics. Recovery time was significantly longer for the patients in group D (p < 0.05).
Conclusion
We concluded that both magnesium sulphate and dexmedetomidine successfully induced deliberate hypotension in patients undergoing middle ear surgery but magnesium sulphate was associated with shorter recovery time and earlier discharge from the PACU.
1 Introduction
Deliberate hypotension is a technique which has been used to decrease intraoperative bleeding and improve the quality of the surgical field for better visualization during middle ear surgery and other head and neck operations [Citation1–Citation4].
Several pharmacologic agents have been used to produce deliberate hypotension. Direct vasodilators as nitroprusside and nitroglycerine, alpha-2 adrenergic agonists as clonidine and dexmedetomidine, beta adrenergic antagonists as propranolol and esmolol, alpha and beta adrenergic antagonists as labetalol, inhalational anaesthetics as isoflurane and sevoflurane, μ-receptors agonist as remifentanil, and N-methyl d-aspartate antagonist as magnesium were all used to induce hypotension during middle ear surgery [Citation5–Citation11].
Magnesium is the fourth most common salt in the human body after phosphorus, calcium and potassium [Citation12]. Magnesium sulphate was previously used to induce deliberate hypotension [Citation13,Citation14]. It produces its hypotensive effect by limiting the outflow of calcium from the sarcoplasmic reticulum and produces a vasodilating effect by increasing the synthesis of prostacyclin and inhibiting angiotensin converting enzyme activity [Citation15]. Hypotension induced by magnesium during surgery is also explained by its powerful analgesic effect [Citation16]. The analgesic action of magnesium is explained by its antagonistic effect at N-methyl d-aspartate receptors [Citation17].
Dexmedetomidine is an α-2 adrenoreceptor agonist. It decreases heart rate and arterial blood pressure by reducing norepinephrine and epinephrine plasma levels [Citation18]. Activation of postsynaptic receptors in the central nervous system by α2-agonists inhibits the sympathetic activity and decreases heart rate and blood pressure and causes sedation.
No studies have been published to compare magnesium sulphate and dexmedetomidine regarding their hypotensive effects in patients undergoing middle ear surgery. The main objective of this prospective randomized study was to compare magnesium sulphate with dexmedetomidine as regards their efficacy in inducing deliberate hypotension and providing better quality of the surgical field during middle ear surgery. The effect of both drugs on postoperative pain and recovery time was also compared.
2 Methods
In this study, 88 adults ASA physical status I and II patients undergoing middle ear surgery were included. A written informed consent was obtained from all patients after approval by the Local Ethics Committee. The enrollment period lasted from January 2010 to March 2011 in Kasr El Eini University Hospital in Cairo (Egypt). Patients with hepatic, renal, cardiovascular, neuromuscular or haematological disorders were excluded. Those with history of using sedatives, narcotics or anticoagulants were also excluded. Patients were randomly assigned to receive either magnesium sulphate (M) or dexmedetomidine (D). Randomization was accomplished by using computerized randomization tables. Anaesthesia was induced by propofol 2 mg/kg iv and fentanyl 1 μg/kg. Patients in the M group received an iv bolus of magnesium sulphate 50 mg/kg in a total of 100 ml saline over 10 min followed by infusion of 15 mg/kg/h until the end of operation. Similarly, patients in the D group received dexmedetomidine 1 μg/kg over 10 min followed by 0.4–0.8 μg/kg/h until the end of surgical procedure. The study drugs were infused using an infusion pump (Module DPS+IS3-Fresenius vial, Le Grand Chemin-38590, Brezins, France). When the eyelid reflex was lost, rocuronium 0.6 mg/kg was injected. A peripheral nerve stimulator (Plexygon nerve stimulator Vygon I Talia S.r.L Via P. Dona, II, Padova, Italy, Ref. 7501031 S/N0507PB202) was used at the wrist to monitor neuromuscular block and the trachea was intubated when T1 was 0%. Additional doses of rocuronium were not administered to allow intraoperative monitoring of facial nerve. When T1 was 25%, muscle relaxation was reversed with atropine 0.02 mg/kg and neostigmine 0.04 mg/kg iv. Anaesthesia was maintained with 1–2 MAC sevoflurane and lungs were ventilated with oxygen and medical air at a ratio of 1:1. Ringer's solution was infused continuously at a rate of 5 ml/kg/h. Mean arterial pressure (MAP) and heart rate (HR) were recorded before induction of anaesthesia (baseline), 1 min after induction of anaesthesia, 1 min before intubation, 1 min after intubation then every 15 min intraoperatively, 1 min before extubation and 5 min after extubation. (Drager Medical systems, Inc., Telford, PA 18969, USA). Blood samples for serum magnesium were obtained before and after surgery. The target MAP during operation was between 60 and 70 mmHg. If hypertension or tachycardia more than 20% of the preoperative value occurred, fentanyl 1 μg/kg was given iv. Sevoflurane concentration was manipulated according to targeted MAP and its end-tidal concentration was recorded every 15 min while the patients were intubated. If hypotension or bradycardia more than 20% of the preoperative value occurred, 5 mg ephedrine for hypotension or 0.5 mg atropine for bradycardia was given iv. Before skin closure all patients were given ondansetron 4 mg iv as an antiemetic prophylaxis. The surgeon who was not aware of the selected hypotensive agent was asked to assess the quality of the surgical field according to the quality scale proposed by Fromme and colleagues [Citation19].
0 = no bleeding.
1 = slight bleeding – blood evacuation not necessary.
2 = slight bleeding – sometimes blood has to be evacuated.
3 = low bleeding – blood has to be often evacuated. Operative field is visible for some seconds after evacuation.
4 = average bleeding – blood has to be often evacuated. Operative field is visible only right after evacuation.
5 = high bleeding – constant blood evacuation is needed. Sometimes bleeding exceeds evacuation. Surgery is hardly possible.
At the end of surgery, study drugs and sevoflurane were discontinued. Patients, after the end of surgery, were transferred to the postanaesthesia care unit (PACU). In the PACU, MAP and HR were recorded on admission and then 15 and 30 min later. Pain was evaluated using visual analogue scale (VAS) starting from 0 for no pain to 100 for worst pain. If VAS was >40, ketorlac 30 mg iv was administered. Patients complaining of postoperative nausea and vomiting were given metoclopramide 10 mg iv. Patients were discharged when fulfilling a score of 9 using a modified Aldrete scoring system [Citation20]. Nurses of the PACU were blinded to patients’ group allocation.
The primary outcome was the quality of surgical field assessed by the surgeon. A sample size of 44 in each group was based on a pilot study we have conducted before. We assumed that a 30% difference in the score of surgical field quality would be clinically significant. A sample size was calculated to be 40 at an alpha error of 0.05 and a beta error of 0.2. Because the primary outcome on which we calculated the sample size was ordinal, we increased the sample size by 10%.
Data were statistically described in terms of mean (±SD), frequencies (number of cases) and percentages when appropriate. Data were tested first for normal distribution by Klomogorov–Smirnov test. Comparison of quantitative variables between the study groups was done using Student t test for independent samples if normally distributed. Mann–Whitney U test was used for non-normally distributed quantitative and ordinal data. For comparing categorical data, Chi square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. A probability value (p value) less than 0.05 was considered statistically significant. All statistical calculations were done using computer programs Microsoft Excel 2007 (Microsoft Corporation, NY, USA) and SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) version 15 for Microsoft Windows.
3 Results
One hundred and forty-one patients were found eligible for the study. Forty-three patients met our exclusion criteria and 10 patients refused participation. Eighty-eight patients were randomized to two groups: group M (n = 44) and group D (n = 44). No patient was excluded from the study.
There were no significant differences between the two groups with regard to age, gender, weight, height and ASA classification as shown in . Postoperative magnesium levels were significantly higher in group M than in group D as shown in .
Table 1 Patients characteristics. Data are mean (SD) or number.
Table 2 Pre- and postoperative serum magnesium levels. Data are mean (SD).
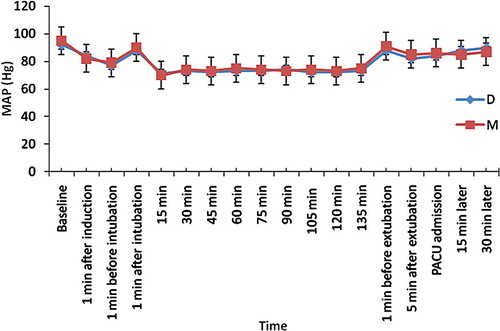
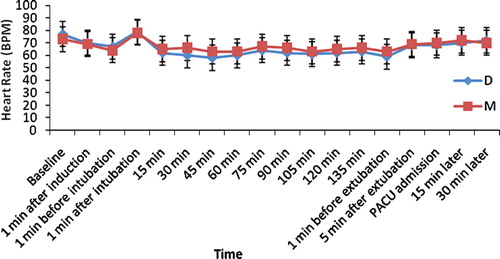
There were no significant differences between the two groups neither in MAP as shown in nor in HR as shown in .
The two study groups were similar in terms of duration of surgery and anaesthesia, type of surgery, bleeding quality score and the need to atropine, ephedrine and fentanyl ()
Table 3 Intraoperative data. Data are mean (SD), median (range) or number.
Again the end-tidal concentrations of sevoflurane were similar in the two study groups ()
Table 4 End-tidal concentrations of sevoflurane. Data are mean (SD).
shows the difference between the two groups in the PACU. Discharge from the PACU required a significantly longer time for the patients in the D group (p < 0.001).
Table 5 PACU data. Data are mean (SD) or number.
4 Discussion
This study shows the ability of both magnesium sulphate and dexmedetomidine to induce deliberate hypotension in patients undergoing middle ear surgery. Mean arterial pressure was successfully reduced to the target values in both groups. Both drugs were equally successful to produce satisfactory surgical field. However the discharge time from PACU in dexmedetomidine group was almost double that in magnesium sulphate group.
Magnesium sulphate is known to augment the action of non-depolarizing neuromuscular blocking drugs and reduce their consumption [Citation21]. However, facial nerve monitoring is required during middle ear surgery and neuromuscular blocking agents were reversed shortly after the beginning of the operation.
Recovery in patients receiving dexmedetomidine was prolonged most probably due its sedative-sparing effects via central actions in the locus coreuleus [Citation22,Citation23]. Other studies observed that recovery time was prolonged in patients who received dexmedetomidine for induced hypotension when compared with control groups [Citation6,Citation24]. Another study observed that there was a prolonged recovery time in patients received dexmedetomidine when compared with those who received remifentanil during gynaecologic laparoscopic surgery [Citation25].
Several studies have reported the ability of both drugs in providing deliberate hypotension. Ryu and colleagues compared magnesium sulphate and remifentanil and proved that both drugs can induce adequate deliberate hypotension for middle ear surgery but magnesium sulphate was associated with better postoperative analgesia and less postoperative nausea, vomiting and shivering [Citation26]. Elsharnouby and colleagues performed a placebo controlled study and concluded that magnesium sulphate reduced MAP, HR and blood loss and was associated with less anaesthetic requirements and emergence time for patients underwent functional endoscopic sinus surgery [Citation13]. Yosri and colleagues designed a comparative study between magnesium sulphate and nitroprusside and concluded that magnesium sulphate could produce deliberate hypotension and provided good surgical conditions for resection of choroidal melanoma with no need for adding potent hypotensive agents [Citation14]. Durmus and colleagues have proved in a placebo controlled study that dexmedetomidine decreased bleeding and anaesthetic requirements in patients undergoing tympanoplasty and septorhinoplasty [Citation24]. Ayoglu and colleagues in a placebo controlled study concluded that dexmedetomidine reduced bleeding and improved visibility and decreased analgesic requirements in septoplasty operations [Citation27]. Although magnesium sulphate and dexmedetomidine were previously investigated as hypotensive agents, there were no studies designed to compare between them as regards their efficiency in controlling MAP and HR, analgesic effect and emergence from general anaesthesia.
The target MAP between 60 and 70 mmHg was decided to achieve hypotensive anaesthesia and bloodless field without subjecting the patients to peripheral tissue ischaemia. This target MAP was determined after revising previous studies in which metabolic and hormonal responses were observed in patients subjected to induced hypotension. Yoshikawa and colleagues induced hypotensive anaesthesia using a similar target MAP of 60–70 mmHg in patients undergoing mandibular osteotomy. They measured blood pyruvate, lactate and glucose and observed insignificant increase in their levels. They concluded that hypotension can be induced safely, if MAP is maintained between 60 and 70 mmHg [Citation28]. Newton and colleagues targeted a MAP of 55 mmHg in patients undergoing middle ear surgery. They also observed insignificant increase in blood lactate and pyruvate levels [Citation29].
Our study was limited by the unavailability of two monitors. We used a subjective scoring system to evaluate the quality of the surgical field instead of a Laser Doppler flowmetry which was used by Degoute and colleagues to measure the middle ear blood flow [Citation9]. We could not assess the depth of anaesthesia as we lacked a bispectral index (BIS) monitor. However the lack of any significant differences in end-tidal sevoflutane concentrations between the two groups suggests that hypotensive properties of the two study drugs are similar in the doses that we used.
Only 16% of patients in the magnesium group and 14% of patients in the dexmedetomidine group required rescue analgesics. These results can be explained by the analgesic properties of both study drugs [Citation17,Citation18]
We concluded that both magnesium sulphate and dexmedetomidine successfully induced deliberate hypotension and good surgical field visibility but magnesium sulphate was associated with shorter recovery time and earlier discharge from the PACU.
Notes
Peer review under responsibility of Egyptian Society of Anesthesiologists.
References
- A.P.BoezaartJ.MerweeA.CoetzeeComparison of sodium nitroprusside and esmolol induced hypotension for functional endoscopic sinus surgeryCan J Anaesth421995373376
- D.B.CoursinD.B.CoursinG.A.MaccioliDexmedetomidineCurr Opin Crit Care72001221226
- J.M.MarchalA.Gomez-LuqueF.Martos-CrespoClonidine decreases intraoperative bleeding in middle ear microsurgeryActa Anaesthesiol Scand452001627633
- C.S.DegouteM.J.RayM.ManchonRemifentanil and controlled hypotension; comparison with nitroprusside or esmolol during tympanoplastyCan J Anaesth4820012027
- C.S.DegouteM.J.RayP.Y.GueugniaudC.DubreuilRemifentanil induces consistent and sustained controlled hypotension in children during middle ear surgeryCan J Anaesth5032003270276
- F.RichaA.YazigiG.SleilatyP.YazbekComparison between dexmedetomidine and remifentanil for controlled hypotension during tympanoplastyEur J Anaesthesiol2552008369374
- G.V.DietrichM.HeesenJ.BoldtG.HempelmannPlatelet function and adrenoceptors during and after induced hypotension using nitroprussideAnesthesiology856199613341340
- J.D.TobiasControlled hypotension in children: a critical review of available agentsPaediatr Drugs42002439453
- C.S.DegouteControlled hypotension: a guide to drug choiceDrugs67200710531076
- L.D.TestaJ.D.TobiasPharmacologic drugs for controlled hypotensionJ Clin Anesth71995326337
- A.DelhumeauJ.C.GranryJ.-P.MonrigalTherapeutic use of magnesium in anaesthesia and intensive careAnn Fr Anesth Reanim141995406416
- N.E.SarisE.MervaalaH.KarppanenMagnesium. An update on physiological, clinical and analytical aspectsClin Chim Acta2942000126
- N.M.ElsharnoubyM.M.ElsharnoubyMagnesium sulphate as a technique of hypotensive anaesthesiaBr J Anaesth962006727731
- M.YosriI.S.OthmanControlled hypotension in adults undergoing choroidal melanoma resection: comparison between the efficacy of nitroprusside and magnesium sulphateEur J Anaesthesiol252008891896
- G.M.SandersK.M.SimIs it feasible to use magnesium sulphate as a hypotensive agent in oral and maxillofacial surgery?Ann Acad Med Singapore271998780785
- A.BuvanendranR.J.McCarthyJ.S.KroinIntrathecal magnesium prolongs fentanyl analgesia: a prospective, randomized, controlled trialAnesth Analg952002661666
- L.DubeJ.C.GranryThe therapeutic use of magnesium in anesthesiology, intensive care and emergency medicine: a reviewCan J Anaesth502003732746
- B.C.BloorD.S.WardJ.P.BellevilleEffects of intravenous dexmedetomidine in humans II. Hemodynamic changesAnesthesiology77199211341142
- G.A.FrommeR.A.MackenzieA.B.GouldJrB.A.LundK.P.OffordControlled hypotension for orthognathic surgeryAnesth Analg6561986683686
- W.F.ThomasA.MacarioThe postanesthesia care unitR.D.MillerAnesthesia2005Churchill LivingstonePhiladelphia27082709
- S.HerroederM.E.SchonherrS.G.De HertM.W.HollmannMagnesium-essentials for anesthesiologistsAnesthesiology1142011971993
- M.MazeI.SegalB.BloorClonidine and other alpha2 adrenergic agonists: strategies for the rational use of these novel anesthetic agentsJ Clin Anesth11988146157
- T.Z.GuoJ.Y.JiangA.E.ButtermanM.MazeDexmedetomidine injection into the locus coreuleus produces antinociceptionAnesthesiology841996873881
- M.DurmusA.K.ButZ.DoganEffect of dexmedetomidine on bleeding during tympanoplasty or septorhinoplastyEur J Anaesthesiol242007447453
- N.M.BulowN.V.BarbosaJ.B.RochaOpiod consumption in total intravenous anesthesia is reduced with dexmedetomidine: a comparative study with remifentanil in gynecologic videolaparoscopic surgeryJ Clin Anesth192007280285
- J.H.RyuI.S.SohnS.H.DoControlled hypotension for middle ear surgery: a comparison between remifentanil and magnesium sulphateBr J Anaesth10342009490495
- H.AyogluO.YapakciM.B.UgurL.UzunH.AltunkayaY.OzerEffectiveness of dexmedetomidine in reducing bleeding during septoplasty and tympanoplasty operationsJ Clin Anesth202008437441
- F.YashikawaH.KohaseM.UminoH.FukayamaBlood loss and endocrine responses in hypotensive anaesthesia with sodium nitroprusside and nitroglycerin for mandibular osteotomyInt J Oral Maxillofac Surg38200911591164
- M.C.NewtonG.D.ChaddB.O'donghueS.M.Sapsed-ByrneG.M.HallMetabolic and hormonal responses to induced hypotension for middle ear surgeryBr J Anaesth7631996352357