
Abstract
A young male, aged 32 years, was brought to the emergency operation theatre, with a household knife-in-situ, in the neck. A detailed history revealed psychiatric illness to be the cause of this self inflicted injury. His vitals were found to be stable and he had no respiratory embarrassment and was conversing comfortably. Intubating him with a knife-in-situ was a great challenge. A simple technique using two endotracheal tubes was used which helped in securing the airway avoiding any further injury with the knife-in-situ.
1 Introduction
Penetrating neck injuries constitute a vital fraction of the challenging emergencies encountered by the anaesthesiologists. The situation is complicated manifolds if the object involved is sharp edged, and is brought in situ. Airway management becomes the key aspect here, as further damage can result in development of haematoma, tissue swelling or primary laryngeal injury; disrupting the airway and making intubation efforts extremely difficult especially in an emergency set up [Citation1]. We describe here such a patient who was managed successfully using two endotracheal tubes.
2 Case report
A young male, aged 32 years, was brought to the emergency operation theatre, with a household knife-in-situ, in the neck (). A detailed history revealed psychiatric illness to be the cause of this self inflicted injury [Citation2]. His vitals were found to be stable, he had no respiratory embarrassment and was conversing comfortably, though with a minimal change of voice. He was asked not to touch or move the knife and keep his head and neck and shoulders immobile.

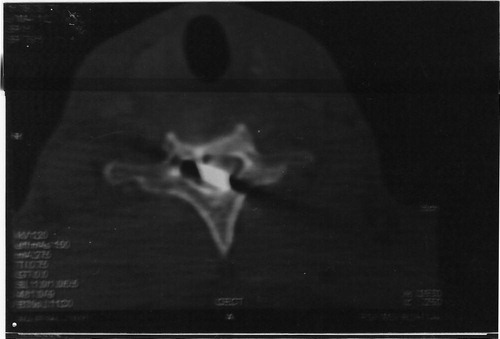
On examination, the knife was 1 cm to the right of the midline, 2 cms above the medial end of the clavicle, at an angle of 85° to the neck in supine position, with approximately half of its length (10 cms) showing outside (). Further examination showed minimal tracheal deviation to the left side and paresis of the left half of the body, lower limbs more than the upper limbs. There were no signs of surgical emphysema. Systemic examination did not reveal any other abnormality. Blood investigations and ECG were normal. Chest X-ray confirmed the left deviation of the trachea with a metallic opacity (knife) lying lateral to it. CT scan in AP view ( and ) showed the knife in-situ, passing through the tracheal wall, sparing the great neck veins, carotid sheath with its contents laterally and the thyroid gland with its vessels above. In the lateral view of the CT scan (), the knife was seen to pierce, the base of the C6 spinous process after crossing the spinal canal through the intervertebral disc between C5 and C6, hence the contralateral paresis.


Patient was shifted to the operation table gently, ensuring stability of the neck. Monitors for ECG, SpO2, NIBP were attached and preoperative vitals were recorded to be: pulse 88/min, BP 124/88 mmHg with SpO2 100% on air. Intravenous access was established using 16G and 18G cannula with Ringer Lactate solution. Anaesthesia was administered with Inj Glycopyrrolate 0.2 mg and Inj Pethidine 30 mg followed by preoxygenation for 5 min. Induction was achieved with Inj Thiopentone sodium 300 mg. After assessing adequacy of mask ventilation, Inj Succinylcholine 100 mg was given to facilitate endotracheal intubation [Citation3].
After manual in line stabilization of the head and neck by an assistant, laryngoscope was gently introduced, wherein the soft palate, posterior pharyngeal wall as well as the epiglottis could be seen, but laryngeal inlet could not be visualized (Cormack & Lehane grade III) [Citation4]. Further movement of the laryngoscope was avoided with the fear of displacing the knife and hence exaggerating the spine injury. In this unusual circumstance for intubation, one endotracheal tube of ID 7.5 mm was passed along the posterior pharyngeal wall deliberately into the oesophagus and its cuff then inflated to avoid any regurgitation, followed by a second endotracheal tube with ID 8 mm with stylet passed, directing its tip towards the laryngeal inlet, blindly. Its connector was then connected to the Bains circuit and its position confirmed by auscultation and ETCO2, cuff was then inflated, bilateral air entry was checked and tube was fixed.
Preoperatively, anaesthesia was maintained using nitrous oxide and halothane (0.5–1%) in oxygen and Inj Vecuronium bromide as required. Proper fluid management and continuous monitoring worked to achieve a smooth per-operative course, wherein, neck was explored and knife removed successfully, sparing all vital structures [Citation5,Citation6]. At the end of surgery, anaesthetics were withdrawn and neuromuscular blockade was reversed with Inj glycopyrrolate 0.4 mg and Inj Neostigmine 2.5 mg after arrival of spontaneous respiration .A smooth extubation was done during deep inspiration on arrival of adequate reflexes, muscle power and tone.
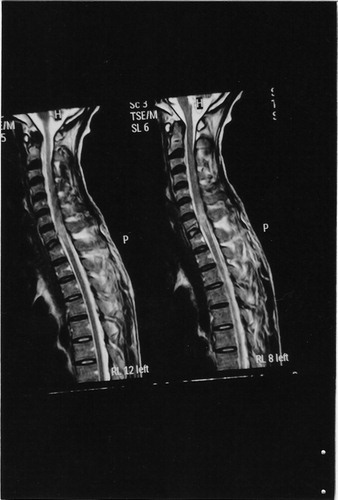
A post operative MRI () showed injury to the spinal cord at C5–C6 level as MRI is superior to CT [Citation7]. However, the post operative course proved to be smooth and uneventful without any increase in the contralateral paresis. Regular follow-up up to two months, showed progressive improvement of the contralateral paresis after which the patient was discharged with baseline mental status [Citation5,Citation6].
3 Discussion
Penetrating neck injuries represent 5–10% of all traumas with mortality rates up to 2–6% [Citation1]. Airway protection in this context is the prime focus of the anaesthetic management. This case presented a rare and unusual circumstance for intubation [Citation8]. The sharp edge of the household knife-in-situ, on its slightest displacement, threatened injury to the most vital structures like spinal cord, great neck viens, carotid vessels, thyroid gland with its vessels, oesophagus and the tracheal wall itself. Proper laryngoscopy was further restricted with the wooden butt of the knife, which had a risk of hitting the handle of the laryngoscope with consequent change in its position causing further damage inside [Citation5].
In such a situation, awake fibreoptic was desirable but our patient, suffering from psychiatric illness, was not cooperative enough. Moreover awake procedure sometimes leads to violent undue coughing and jerking movements which were obviously undesirable in this patient. If airway cannot be secured awake, then omitting muscle relaxant for endotracheal intubation is considered safer in cases of difficult airway. However, in our patient, it required least movement of the head and neck and best intubating conditions for tube insertion which, in view of adequate mask ventilation led us to choose relaxant technique. Moreover owing to the clean cut wound with sharp edged object, still in-situ and negative CT findings for any gross tissue oedema affecting airway, this was considered optimal.
Fibreoptic intubation is the gold standard, but unavailability of the same in an emergency set up was our limitation. Blind nasal intubation though recommended by Wetzel et al, was ruled out as it would require neck movements for tube negotiation risking displacement of the knife and further damage to vital structures [Citation1]. A gum elastic bougie is a useful alternative and is a recommended technique in such situation [Citation9]. Laryngeal mask airway and Intubating LMA seat in the hypopharynx, and hence carried the risk of displacing both the knife and its surroundings. Classic LMA provided an alternative for mask ventilation, which was otherwise satisfactory in this case, using a face mask. Its use for maintenance of airway during surgery was ruled out foreseeing the unpredictability of surgical exploration and risk of aspiration. Intubating LMA was risky as its handle would have hit the knife butt and caused further damage. Thus, in this scenario, this method using two endotracheal tubes provided a safe, easy and simple access to the laryngeal inlet by neither displacing the knife nor, exaggerating the angle of the neck, hence avoiding any further injury to the patient.
To conclude, endotracheal intubation using two endotracheal tubes is a good alternative in such unusual circumstances of difficult intubation, and hence recommended wherever a similar situation is faced.
Conflict of interest
There is no conflict of interest.
Notes
Available online 18 September 2014
ReReferences
- NathaenWeitzelJohnKendallPeterPonsBlind nasotracheal intubation for patients with penetrating neck traumaJ Trauma56200410971101
- D.P.MandaviaS.QuallsI.RokosEmergency airway management in penetrating neck injuriesAnnals Emerg Med3532000221225
- S.KiharaS.WatanabeJ.BrimbacombeN.TaguchiY.YaghuciY.YamaskiSegmental cervical spine movement with ILMA during manual in line stabilization in patients with cervical pathology undergoing cervical spine surgeryAnaes Anal912000195200
- H.ImokawaT.TazawaPenetrating neck injuries involving wooden foreign BodiesAuris Nasus Larynx30Suppl February2003S145S147
- R.B.BellT.OsbonManagement of penetrating neck trauma: a new paradigm for civilian traumaOral Maxillofacial Surg6542007691705
- J.SteinfeldtT.A.BevJ.M.RichUse of GEB in zone II penetrating neck traumaJ Emerg Med2004
- R.W.NasonG.N.AssurasP.R.GrayPenetrating neck injuries: analysis of experience from a Canadian trauma centreCan J Surg4422001122126 April
- D.BarnesF.ClarkP.BaguleyN.BradySelf inflicted neck injury with an electric drillInjury3372002635638 September
- E.GraciaP.PrimmPenetrating neck trauma: an unusual presentationPediatric Emerg Care1642000270272 August