
Abstract
Background and aim
Post-operative pain is considered an important complication of Intravenous regional anesthesia (IVRA) which is gaining popularity especially for surgeries on upper limbs.
Methods
The present double blind randomized clinical trial was conducted on 60 candidates of upper limb surgeries aged between 20 and 60 years who were of ASA classes 1 or 2. Subjects were randomly assigned to 4 groups: the first group was treated solely with 3 mg/kg of Lidocaine. The second and third groups received the same amount of Lidocaine plus 8 mg of Dexamethasone or 300 mg of Paracetamol respectively and for the fourth group a combination of all medications was used. For all patients, Lidocaine was diluted with normal saline until a total volume of 40 cc was reached. Onset of Sensory and motor nerve blocks, severity of post-operative pain and amount of mepridine consumption in the first 24 h after surgery were assessed.
Results
Onset of Sensory and motor nerve block was significantly accelerated in the fourth group (p < 0.01). Post-operative pain and analgesic consumption were significantly reduced in the fourth group when compared with the other groups (p < 0.05).
Conclusion
A combination of Paracetamol and Dexamethasone significantly enhances the analgesic effect of Lidocaine in IVRA by accelerating the establishment of both the sensory and motor nerve blocks and prolonging the period of analgesia as well as improving the quality of analgesia and reducing the need for analgesic medications during and after the operation.
Introduction
Many orthopedic surgeries may be performed under nerve blocks or other alternatives of GA such as Intravenous regional anesthesia (IVRA). Named after the German Surgeon August Bier who developed the IVRA or the Bier method in 1908, this technique is still deemed useful for limb surgeries [Citation1], especially when GA is highly associated with risks such as difficult intubation or aspiration. The advantages of this technique include cost effectiveness, rapid achievement of anesthesia feasibility at a variety of settings such as day case or the A&E department, desirable site of operation and reduced risk of hemorrhage [Citation2]. However, this technique is also associated with a number of untoward reactions which include toxicity of the local anesthetic agent, obtunded onset of anesthesia, fatigue and hypotonia of muscles and the pain of applying the tourniquet application discomfort and the pain that afflicts the limb following deflation of the tourniquet [Citation3]. The anesthetic agent that is to be used in IVRA should ideally yield short onset, long lasting anesthesia with a low dose and minimal side effects. Efforts are currently underway to optimize the effect of local anesthetics and minimize their side effects by using a combination of drugs including opioids such as fentanyl [Citation4,Citation5], Mepridine [Citation6,Citation7], Morphine, Sufentanil and Tramadol [Citation1]; NSAIDs such as Ketorolac [Citation1,Citation8], Tenoxicam and Acetyl Acetate [Citation1]; α2 agonists such as Clonidin [Citation1,Citation9,Citation10] and Dexmedetomidine [Citation1,Citation11]; Muscle relaxants such as Pancronium [Citation4], Atracurium, cis-Atracurium and Mivacurium [Citation1], Neostigmin [Citation12,Citation13], Ketamin [Citation14], Magnesium [Citation15] and Bicarbonate [Citation1].
Among a host of trials on a wide range of agents to optimize the quality and quantity of anesthesia, some suggest that addition of Dexamethasone [Citation16] or Paracetamol [Citation17,Citation18] may be conducive to the effect of Lidocaine in achieving a desirable state of anesthesia. In the absence of any study to compare the independent effect of Paracetamol and Dexamethasone and their combined effect on IVRA with Lidocaine, particularly in the upper limb, and in view of the increasing use of IVRA for operations in the upper limb, this study was conducted to evaluate the effect of those medications on the depth and duration of IVR anesthesia in upper limbs.
Materials and methods
The present double blind randomized clinical trial was conducted on 60 candidates of upper limb surgeries who were referred to the Shahid Bahonar Hospital in the city of Kerman. The study was endorsed by the research council of Kerman University of Medical Sciences and was approved by its ethical committee (Ethical code No. k/90/462). Before recruitment of first subject, study protocol was registered in Iran Registration of Clinical Trials (IRCT) database under the ID:
IRCT201209053104N2.Citation1
Informed consent was obtained from all subjects who aged between 20 and 60 years and were of ASA classes 1 or 2. Subjects were randomly assigned to 4 groups: the first group was treated solely with 3 mg/kg of Lidocaine. The second and third groups received the same amount of Lidocaine plus 8 mg of Dexamethasone or 300 mg of Paracetamol respectively and for the fourth group a combination of all medications was used. For all patients, Lidocaine was diluted with normal saline until a total volume of 40 cc was reached. Subjects who were suspected of any substance or drug abuse, those who were allergic to Lidocaine or had sustained open fractures of upper limb or had a history of hepatic disease, those cases who were complicated by infection and those who had received any other anesthetic or analgesic medicament prior to the operation were excluded from the study. Blood pressure, heart rate and arterial oxygen saturation were monitored for all patients in the operation theater and IV canula was fitted to the healthy limb of all subjects as a route of fluid or drug administration. Using a pink venflon, another IV line was secured at the distal end of the affected limb. After applying Smarch bandage for the purpose of blood evacuation, the limb was elevated for 2 min and then the proximal tourniquet was inflated to reach a pressure of 250 mmHg. Medications were administered by an anesthesiologist who was unaware of their content in a period of 90 s. Then, using a 22 gauge needle, sensory function was evaluated in the dermatomes pertaining to the Ulnar, Median and Radial nerves. Motor function was also assessed by flexion and extension of the wrist and fingers. Absence of any movement was regarded as completion of motor nerve block. Upon completion of both sensory and motor nerve blocks, the distal tourniquet would be inflated up to 250 mmHg and the proximal tourniquet would be deflated. Bp, heart rate and arterial O2 saturation readings were recorded before and after application of the tourniquet as well as at 5, 10, 15, 20, 30, 40 and 50 min past the start of the operation. The pain that was associated with tourniquet application was measured by using the Visual Analog Scale (VAS) at 5, 10, 15, 20, 30, 40 and 50 min after inflation of the tourniquet. Once the VAS score exceeded 4, 1 μg/kg of Fentanyl would be administered to the patient. During the surgery, each time the BP dropped to lower than 90 mmHg, it was treated with 5 mg of IV Ephedrin and when the heart rate dropped to lower than 50 b/min, the patient would receive 0.5 mg of IV Atropine. At the end of the operation, an anesthesiologist who was unaware of the group the patient was assigned to, would label the quality of the patient’s anesthesia as poor (in need of further analgesia), moderate (patient often complaining of minor pain but no need for analgesia), Good or Excellent (no complain of pain).
Tourniquets would remain inflated for no shorter than 30 min and no longer than 2 h. Following the deflation of the tourniquet, the restoration of the sensory function was assessed every 30 s with the pin prick test. The re-activation time of the motor function was also recorded once the patient was able to voluntarily move fingers. For two h past the operation when the patient was moved to the recovery room or the ward, he/she was monitored for development of untoward effects such as Nausea, Vomiting, skin rash, Tachycardia, bradycardia, Hypotension, hypertension, vertigo, tinnitus and hypoxia. Any VAS score of higher than 20 was treated with 4 mg of IV Mepridine.
Based on the results of the Sen et al.’s trial [Citation29], sample size was calculated by assuming that m1 = 1.8, m2 = 0.2, sd1 = 2, Sd2 = 1, α = 0.05 and β = 0.8. Accordingly, the size of the sample was equal to 60. Data analysis was performed by means of the SPSS 17. The Post Hoc Tukey test and the Repeated Measure ANOVA were employed for comparing the mean period of time that was required for the establishment of sensory and motor nerve blocks and the mean VAS scores between the 4 groups of subjects. The quality of anesthesia was compared between the 4 groups of subjects by means of the chi2 test. Differences with P values of less than 0.05 were considered significant.
Results
The 4 groups of subjects were equivalent in terms of age, height, weight and gender. No significant difference was observed between the 4 groups in terms of intra operational BP fluctuation or untoward conditions such as bradycardia, Hypotension and need for fentanyl administration during the operation ().
able 1 Demographic particulars and statistical indices of intra operational variables in the 4 groups of subjects.
Mean VAS score during the operation was lowest in the fourth group (receiving all medications) at 1.84 ± 0.8. This figure increased from 2.06 ± 0.8 for the 3rd group (Lidocaine + Paracetamol) to 2.1 ± 0.9 and 2.7 ± 1.2 for the 2nd and 1st groups respectively. The differences were all statistically significant (p < 0.05) except for the difference between the 2nd and the 3rd groups (p > 0.05) ().
able 2 Percentage of analgesic requirement and statistical indices of VAS during the first 24 h past the operation in the 4 groups of subjects.
Analysis of the mean and SD of VAS scores throughout the first 24 h past the operation reveals that the highest fluctuation and thus need for mepridine were in the first 6 h as the VAS score at 6 h past the operation which pertained to the 4th group was equal to 3 ± 0.3 and for the 3rd, 2nd and fourth groups it was equal to 3.4 ± 0.5, 3.3 ± 0.4 and ±0.4 3.8 respectively. These differences were statistically significant between the 4th group and the other 3 groups and between the 1st group and both the 2nd and 3rd groups (P < 0.05). The difference that existed between the 2nd and 3rd groups in this regard was not statistically significant (P > 0.05).
As depicted in table number 2, the difference between the VAS scores at 12 and 24 h past the operation was not statistically significant in all groups.
Mean and SD of the period of time that was required for the establishment of sensory nerve block (in minutes) were 1.86 ± 0.5, 3.2 ± 0.4, 3.2 ± 0.4 and 5.2 ± 0.7 5.2 for the 4th to 1st groups respectively. The decrease in this index was statistically significant from the 4th to the other groups (p < 0.01) and from the 2nd and 3rd groups to the 1st group (P < 0.001) ().
able 3 Comparison of the mean and standard deviation of onset of sensory and motor nerve blocks, Tourniquet associated pain and duration of anesthesia in the 4 groups of patients.
The mean and SD of the latency period for the onset of tourniquet associated pain (in minutes) were 35.4 ± 1.9, 27.8 ± 1.1, 27.6 ± 1.2 and 22 ± 1.6 for the 4th to the 1st groups respectively which implies a significant increase from the 1st three groups to the 4th group and from the 1st group to the 2nd and 3rd groups (p < 0.01) ().
The mean and SD of the duration of analgesia were 63 ± 2.3, 47.6 ± 1.5, 47.9 ± 2.6 and 43 ± 2.3 for the 4th to 1st groups respectively which again implies a significant increase from the 1st three groups to the 4th group and from the 1st group to the 2nd and 3rd groups (p < 0.01) ().
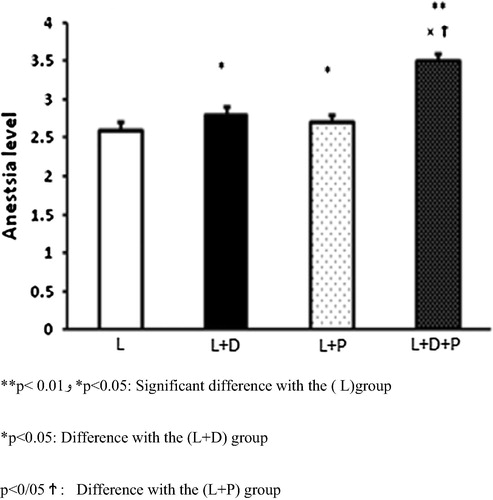
The quality of anesthesia was also significantly higher in the 4th group as compared to the other groups and in the 2nd and 3rd groups as compared to the first group (P > 0.05) ().
Discussion
The synergistic effects of Paracetamol as an analgesic and Dexamethasone as anti-inflammatory agent in pain suppression, when combined with other analgesic medications, have been proved previously in several probes. The present study depicts a more pronounced analgesic effect for Lidocaine when combined with these two widely used medicines.
As a week inhibitor of prostaglandin synthesis, Paracetamol acts in a similar fashion to selective inhibitors of COX II; however, it lacks their anti-inflammatory effects [Citation19,Citation20]. Several mechanisms have been proposed for the analgesic effects of Paracetamol; for instance, Ottani et al. [Citation21] hypothesized that it exerts its effects primarily by modification of Cannabinoid receptors. In line with this assumption, Antagonists of Cannabinoid receptors have been shown to null the analgesic properties of Paracetamol [Citation22,Citation23]. The recent discovery of COX-3 has suggested a central mechanism for Paracetamol induced analgesia [Citation24,Citation25] which is gaining increasing popularity for the purpose of pain control [Citation26].
In view of the increasing popularity of IVRA, particularly for upper limb operations, and the necessity of post-operative pain management, several studies have aimed to strike the optimal combination of medicaments.
Canbay et al. [Citation27] showed that paracetamol may decrease the pain at the site of Propophel injection, which is consistent with the goals of the present study in using the peripheral antinoceptive effect of paracetamol.
Two other reports by Celik et al. [Citation28] and Sen et al. [Citation29] also depicted positive results with Adjuvant use of Paracetamol in IVRA. As implied by the results of the present study, although both Paracetamol and Dexamethasone effectively lower the need for post-operative analgesic medication, the difference in their individual analgesic effect is insignificant. As a Corticosteroid, Dexamethasone is a frequently used medicine which has also been tried individually or in combination with other drugs for the purpose of reducing post-operative complications such as nausea and vomiting. A possible explanation for the benefits of Dexamethasone in controlling post-operative pain is the fact that acute inflammation due to tissue injury is believed to be a main cause of post-operative pain. Several studies have addressed the use of Corticosteroids and Dexamethasone in particular for induction and prolongation of analgesia (16). For example, in a study on 75 candidates of hand surgery, Bigot et al. [Citation30] showed that Dexamethasone improves the quality and quantity of analgesia during the first day after IVRA. No published literature on a controlled trial on comparing the individual analgesic effects of Paracetamol and Dexamethasone as well as their combination was found by the authors of the present study. The results of the present study show that a combination of Paracetamol and Dexamethasone significantly enhances the analgesic effect of Lidocaine in IVRA by accelerating the establishment of both the sensory and motor nerve blocks and prolonging the period of analgesia as well as improving the quality of analgesia and reducing the need for analgesic medications during and after the operation. Hence, a combination of a specific pain killer and an anti-inflammatory agent may be considered as the standard medication in IVRA.
Conflict of interest
We have no conflict of interest to declare.
Notes
Peer review under responsibility of Egyptian Society of Anesthesiologists.
References
- A.ChoyceP.PengA systematic review of adjuncts for intravenous regional anesthesia for surgical proceduresCan J Anaesth49120023245 Jan
- C.N.JohnsonIntravenous regional anesthesia: new approaches to an old techniqueCRNA11220005761 May
- J.GuayAdverse events associated with intravenous regional anesthesia (Bier block): a systematic review of complicationsJ Clin Anesth2182009585594 Dec
- F.SztarkM.ThicoipeJ.F.Favarel-GarriguesP.LassieM.E.PetitjeanP.DabadieThe use of 0.25% lidocaine with fentanyl and pancuronium for intravenous regional anesthesiaAnesth Analg8441997777779 Apr
- M.T.PitkanenM.XuJ.HaasioP.H.RosenbergComparison of 0.5% articaine and 0.5% prilocaine in intravenous regional anesthesia of the arm: a cross-over study in volunteersReg Anesth Pain Med2421999131135 Mar-Apr
- I.AcalovschiT.CristeaIntravenous regional anesthesia with meperidineAnesth Analg8131995539543 Sep
- S.S.ReubenR.B.SteinbergS.D.LurieIs there a place for meperidine in intravenous regional anesthesia?Anesth Analg875199812151216 Nov
- S.S.ReubenR.B.SteinbergH.MaciolekP.ManikantanAn evaluation of the analgesic efficacy of intravenous regional anesthesia with lidocaine and ketorolac using a forearm versus upper arm tourniquetAnesth Analg9522002457460 Aug
- M.GentiliJ.M.BernardF.BonnetAdding clonidine to lidocaine for intravenous regional anesthesia prevents tourniquet painAnesth Analg886199913271330 Jun
- S.S.ReubenR.B.SteinbergJ.L.KlattM.L.KlattIntravenous regional anesthesia using lidocaine and clonidineAnesthesiology9131999654658 Sep
- D.MemisA.TuranB.KaramanliogluZ.PamukcuI.KurtAdding dexmedetomidine to lidocaine for intravenous regional anesthesiaAnesth Analg9832004835840 Mar
- A.TuranB.KaramanlyogluD.MemisG.KayaZ.PamukcuIntravenous regional anesthesia using prilocaine and neostigmineAnesth Analg955200214191422 Nov
- D.SethiR.WasonIntravenous regional anesthesia using lidocaine and neostigmine for upper limb surgeryJ Clin Anesth2252010324328 Aug
- C.M.ViscomiA.FriendC.ParkerT.MurphyM.YarnellKetamine as an adjuvant in lidocaine intravenous regional anesthesia: a randomized, double-blind, systemic control trialReg Anesth Pain Med3422009130133 Mar-Apr
- A.TuranD.MemisB.KaramanliogluT.GulerZ.PamukcuIntravenous regional anesthesia using lidocaine and magnesiumAnesth Analg1004200511891192 Apr
- D.J.KopaczP.G.LacoutureD.WuP.NandyR.SwantonC.LandauThe dose response and effects of dexamethasone on bupivacaine microcapsules for intercostal blockade (T9 to T11) in healthy volunteersAnesth Analg9622003576582 Feb
- A.MirkheshtiM.R.AryaniP.ShojaeiA.DabbaghThe effect of adding magnesium sulfate to lidocaine compared with paracetamol in prevention of acute pain in hand surgery patients under Intravenous regional anesthesia (IVRA)Int J Prev Med392012616621 Sep
- M.J.KoJ.H.LeeS.H.CheongC.M.ShinY.J.KimY.K.ChoeComparison of the effects of acetaminophen to ketorolac when added to lidocaine for intravenous regional anesthesiaKorean J Anesthesiol5842010357361 Apr
- B.J.AndersonParacetamol (Acetaminophen): mechanisms of actionPaediatr Anesth18102008915921 Oct
- J.F.HerreroE.A.Romero-SandovalG.GaitanJ.MazarioAntinociception and the new COX inhibitors: research approaches and clinical perspectivesCNS Drug Rev932003227252 Fall
- A.OttaniS.LeoneM.SandriniA.FerrariA.BertoliniThe analgesic activity of paracetamol is prevented by the blockade of cannabinoid CB1 receptorsEur J Pharmacol5311–32006280281
- S.MitrirattanakulN.RamakulA.V.GuerreroY.MatsukaT.OnoH.IwaseSite-specific increases in peripheral cannabinoid receptors and their endogenous ligands in a model of neuropathic painPain1261–32006102114 Dec 15
- M.DaniJ.GuindonC.LambertP.BeaulieuThe local antinociceptive effects of paracetamol in neuropathic pain are mediated by cannabinoid receptorsEur J Pharmacol5731–32007214215 November 14
- N.V.ChandrasekharanH.DaiK.L.RoosN.K.EvansonJ.TomsikT.S.EltonCOX-3, a cyclooxygenase-1 variant inhibited by acetaminophen and other analgesic/antipyretic drugs: cloning, structure, and expressionProc Natl Acad Sci USA992120021392613931 October 15
- D.H.BeckM.SchenkU.DoepfmerW.J.KoxRectal paracetamol has a significant morphine-sparing effect after hysterectomyBr J Anesth8542000658659 Oct
- P.H.PetterssonJ.JakobssonA.OwallIntravenous acetaminophen reduced the use of opioids compared with oral administration after coronary artery bypass graftingJ Cardiothorac Vasc Anesth1932005306309
- O.CanbayN.CelebiO.ArunA.H.KaragozF.SaricaogluS.OzgenEfficacy of intravenous acetaminophen and lidocaine on propofol injection painBr J Anesth100120089598
- M.CelikF.SaricaogluO.CanbayD.DalA.UzumcigilG.LeblebiciogluWithdrawn the analgesic effect of paracetamol when added to lidocaine for intravenous regional anesthesiaMinerva AnestesiolOct 212011
- H.SenY.KulahciE.BicererS.OzkanG.DagliA.TuranThe analgesic effect of paracetamol when added to lidocaine for intravenous regional anesthesiaAnesth Analg1094200913271330
- Z.BigatN.BoztugN.HadimiogluN.CeteN.CoskunfiratE.ErtokDoes dexamethasone improve the quality of intravenous regional anesthesia and analgesia? A randomized, controlled clinical studyAnesth Analg10222006605609