
Abstract
Introduction
Burns are one of the most common and devastating forms of trauma. Patients with serious thermal injury require immediate specialized care in order to minimize morbidity and mortality. (1) The main purpose of this study was to determine the prevalence of bacterial wound infection in critically ill burn patients in surgical intensive care unit in Egypt.
Objectives
The aim of this study was to determine the bacterial isolates in sever burn wound infection, suitability to antibiotics and there are mortalities.
Methods
We conducted a one year retrospective study in the surgical ICU. Wound swab Culture and sensitivity reports of admitted patients. All the patients of all age groups suffering with flame burnt and both sexes having complete Culture and sensitivity reports were included.
Results
The main finding of the current study described herein was the percent of isolates from burn wound (60%). The most common organism was pseudomonas (49%). Multidrug resistant gram negative organisms represent about 60% of the isolates. Pattern of antibiotic sensitivity was 84% for colistin, 39% for amikacin and 35% for imipenem. The mortalities in our study were 80%.
Introduction
Burns are one of the most common and devastating forms of trauma. Patients with serious thermal injury require immediate specialized care in order to minimize morbidity and mortality [Citation1]. It has been estimated that 75% of all deaths following thermal injuries are related to infection [Citation2]. Burn patients are at a high risk for infection as a result of the nature of the burn injury itself, the immune compromise effects of burns, prolonged hospital stays, intensive diagnostic and therapeutic procedures. In addition, control and prevention of infectious diseases among burned patients present a greater and more specialized problem due to disrupting the skin barrier and the environment in Burn Units that might be contaminated with resistant organisms. These organisms can easily transmit from one patient to another. Those burn care units can be the site of explosion and prolonged outbreaks caused by resistant organisms [Citation3,Citation4].
Burn wound surfaces are sterile immediately following thermal injury, and these wounds eventually become colonized with microorganisms [Citation5], gram positive bacteria that survive the thermal insult, such as Staphylococcus aureus located deep within sweat glands and hair follicles, heavily colonizing the burn wound surface within first 48 h [Citation5]. Topical antimicrobials decrease microbial overgrowth but seldom prevent further colonization with other potentially invasive bacteria and fungi. Gastrointestinal and upper respiratory tract and the hospital environment [Citation6]. Following colonization, these organisms start penetrating the viable tissue depending on their invasive capacity, local wound factors and the degree of the patients’ immunosuppression [Citation7]. If sub-eschar tissue is invaded, disseminated infection is likely to occur, and the causative infective microorganisms in any burn facility changes with time [Citation8]. The pattern of antimicrobial susceptibility of S. aureus and other organisms has changed worldwide, especially in developing countries that antimicrobial agents have become increasingly less effective [Citation9]. We will propagate retrospective observational study to assess the prevalence of bacterial wound infections in critically ill burn patients and their outcome.
Patient and methods
This study was performed in a surgical ICU at Cairo University in Egypt retrospectively conducted on wound swab Culture and sensitivity reports of admitted patient.
All the patients suffering with severe flame burnt of all age groups and both sexes having complete Culture and sensitivity reports were included.
Patients were resuscitated using the modified Parkland formula [Citation10]. Enteral nutrition was started within the 24 h of injury and gradually increased during the first 3 days.
Excision of the burn wound will begin after the first 2 days. Burn wounds were treated daily with closed dressings after application of silver sulfadiazine.
Wound swaps were obtained twice weekly to monitor colonization and when infection was suspected samples were cultured on thioglycollate medium and blood agar in Department of Microbiology laboratory.
Prophylactic antibiotics were given 30 min before debridement. Adding or changing antibiotics was based on culture and sensitivity.
The isolation practices implemented in the ICU included hand decontamination before each patient contact, washing hands and changing gloves between sequences of care, and wearing gloves in case of contact with burn wound body substance [Citation11].
Results
Among 35 burn patients enrolled in our study, female patients were 16 (46%) and male patients were 19 (54%). 11 (31%) patients lied in age group (21–30); mean age was 24 ± 18 and median age was 22 years. 21(60%) patients were TBA more than 50% mean burn area 58.6 ± 20 and median of burn area was 60 .
able 1 Demographic data characteristics and percent of burn surface area.
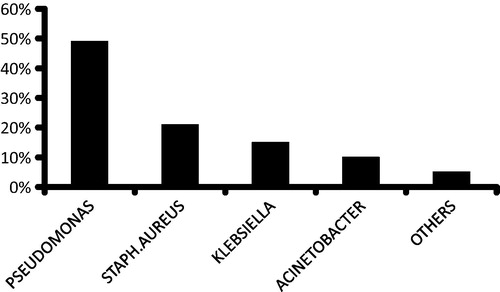
Growth of burn wound bacterial organisms and culture sensitivity pattern were recorded. The most common organism was pseudomonas (49%) followed by S. aureus (21%) and Klebsiella (15%) .
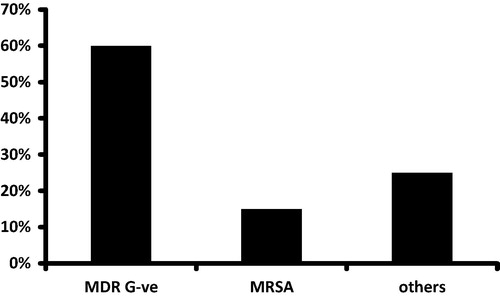
Multidrug resistant gram negative organisms represent about 60% of the isolate .
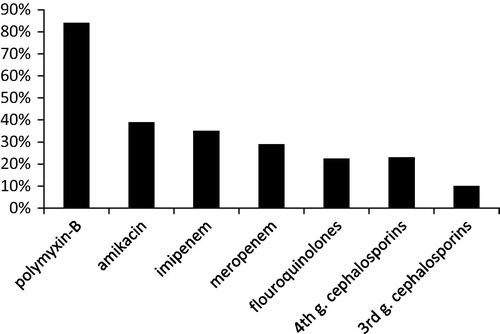
Pattern of antibiotic sensitivity was 84% for colistin, 39% for amikacin and 35% for imipenem .
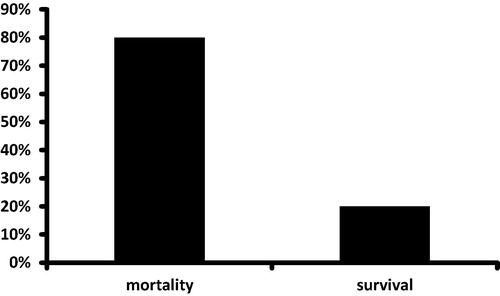
The mortalities in our study were 80% while 20% of patients survived and were discharged from the ICU .
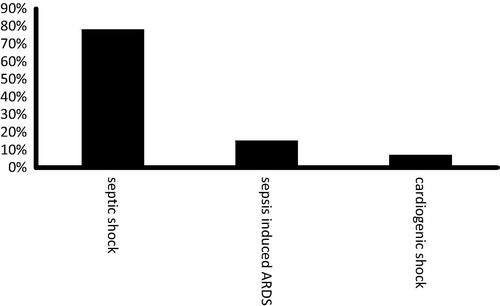
78% of mortalities were due to septic shock while 15% died from sepsis induced ARDS and 7% of mortalities were caused by cardiogenic shock .
Discussion
Burns are one of the most common and devastating forms of trauma. Patients with serious thermal injury require immediate specialized care in order to minimize morbidity and mortality [Citation1]. Burn wound if not excised and grafted early becomes an ideal culture medium for the growth of microorganisms [Citation12]. Infection is an important cause of morbidity and mortality in burns. Severe burn patients are very susceptible to infection because of wide exposed raw areas, the presence of necrotic tissue, protein rich exudates, inability of blood to reach the colonized areas of wounds and other host defense mechanisms [Citation13]. Also mattresses, bed sheets, dressing materials, and other equipment used for patient care, prolonged catheterization, central/peripheral lines, inefficient isolation of infected patients, decreased host resistance, and inappropriate antibiotic use are the most important causes for nosocomial infections in Burn Units [Citation14].
The colonization and later invasion of tissues are from patient’s normal flora of skin or from gastrointestinal tract or more usually by cross infection [Citation15]. Many burn patients die as a result of infection during their hospital courses. The rate of infection in burn cases is extremely high in developing countries [Citation16].
We conducted a retrospective observational study from January 2014 to January 2015 to assess the prevalence of burn wound infections, type and pattern of the bacterial isolates and their outcome in our surgical ICU.
The main finding of the current study described herein was that the percent of isolates from burn wound from 35 burn patients was 32 from 53 wound cultures (60%). This is in agreement with Agnihotri et al. [Citation17] who found isolates present in 57.8% of cases.
In the present study the most common organism was Pseudomonas aeruginosa (49%) followed by S. aureus (21%) and Klebsiella (15%). This finding is in agreement with Hodle et al. [Citation18] that found P. aeruginosa (44%) and methicillin-resistant S. aureus (MRSA) (33%) as the most prevalent organisms isolated in burn centers in survey of 104 U.S. burn units. Another study performed in Egypt by Naser et al. [Citation19] reported their results coincide with our results.
In contrast to our results Imran et al. [Citation20] reported that Staphylococcus was found to be the most common organism isolated. The explanation of this different results may be due to they reported there results in pediatric ICU, differences in geographical location, hygienic measures and cross infection by the hand of the medical personnel, air and other materials. Our center did not have the facilities to cover the burn wound early allowing the gram negative pathogens to be colonized and invade the wound and we performed our study in surgical ICU not specialized isolated once for burn patients.
In the present study the highest incidence of burn occurred in the age group (21–30) by 31%. This finding was consistent with Ansari Lari et al. [Citation21], where this age group was the most active, impulsive and adolescence.
In the current study we found that antibiotic sensitivity was 84% for colistin and 39% for amikacin while other antibiotics had poor sensitivity. This is in agreement with Pavoni et al. [Citation22] reported that most of organisms causing infection in burn patients were highly resistant to routinely used antibiotic. In contrast to our finding Zhang et al. [Citation23] and Revathi et al. [Citation24] found that P. aeruginosa was sensitive to the commonly used antibiotics. This may be due to high prevalence of drug resistant organisms in our unit due to prolonged antibiotic consumption, non-adherent to hospital policy of antibiotics in particular this type of patients who were immunocompromized and improbably isolated.
Our study demonstrated that the mortality of the severe burn patients was unfortunately high (80%) mostly due to septic shock (78%) in contrast to Pavoni et al. [Citation22] who reported 54% mortalities in this study. This could be explained by the following: improper early coverage, isolations and prevalence of pan-resistant organisms in our study. On the other hand Akerlund et al. [Citation25], in a large national-wide epidemiological study of burned patients, reported a low mortality rate (3%). Unfortunately, the data on burn size and depth were not found and usable as a large number of patients in this database lacked such information.
Our study have several limitations, First, it is an observational and is potentially susceptible to several forms of bias, nonetheless. Second, it is retrospective electronic patient records make it difficult to distinguish infection from colonization. Lastly it is single study performed in surgical ICU not specialized in burn trauma.
Conclusion
Multidrug resistance gram negative organisms are the most common isolates from severe burn wound. Our study has high mortalities, and this is due to growth of multidrug-resistant organisms, improper isolation and late coverage of burn area. Aggressive infection control measures and early coverage of burn wound should be propagated strictly to decrease burn related mortalities.
Conflict of interest
The authors declare that there is no conflict of interest in this work.
Notes
Peer review under responsibility of Egyptian Society of Anesthesiologists.
References
- S.G.SantucciS.GobaraC.R.SantosC.FontanaA.S.LevinInfections in a burn intensive care unit: experience of seven yearsJ Hosp Infect532003613
- B.H.Bowser WallaceD.B.GravesF.T.CaldwellAn epidemiological profile and trend analysis of wound flora in burned children: 7 years experienceBurns Incl Therm inj1119841625
- E.E.TredgetH.A.ShankowskyR.RennieR.E.BurrellS.LogsettyPseudomonas infections in the thermally injured patientBurns3012004 Feb326
- A.R.QaderJ.A.MuhamadNosocomial infection in Sulaimani Hospital, IraqAnn Burns Fire Disasters2342010177181
- W.W.MonafoB.FreedmanTopical therapy for burnsSurg Clin North Am671987133145
- J.F.HansbroughBurn wound sepsisJ Intensive Care Med21987313327
- W.L.MansonP.C.PernotV.FidlerE.W.SauerColonization of burns and duration of hospital stay of severely burned patientsJ Hosp Infect2219925563
- Forbes BA, Sahm DF, Weissfeld AS. Bailley and Scott diagnostic microbiology. 10th ed. Mosby; 1998.
- T.AlebachewG.YismawA.DerabeStaphylococcus aureus burn wound infection among patients attending yekatit 12 hospital burn unit, addis ababa, ethiopiaEthiop J Health Sci2232012209213
- C.R.BaxterFluid volume and electrolyte changes of the early post-burn periodClin Plast Surg11974693709
- J.J.LeeJ.A.MarvinD.M.HeimbachInfection control in a burns centerJ Burn Care Rehabil111990575580
- BauerKirbySherriTurkekAntibiotic susceptibility testing methodsAm J Clin Pathol451966493498
- B.TayyabaA.JamshedA.SoofiaAntibiotic sensitivity pattern in burn wound | culturesJ Surg Pakistan102005811
- C.ParadeeC.PiyapongS.PipatComparison between Hospital Single Air Unit and Central Air Unit for Ventilation Performances and Airborne MicrobesAerosol Air Qual Res8120082836
- G.L.FrenchJ.LingY.W.HuiDetermination of methicillin-resistance in Staphylococcus aureus by agar dilution and disc diffusion methodsJ Antimicrob Chemother201987599608
- Wiwing V. Peran Mikroorganisme Lingkungan Dalam Menimbulkan Infeksi Nosokomial di Unit Luka Bakar Rumah Sakit Ciptomangunkusumo. Perpustakaan Universitas Indonesia; 2005.
- N.AgnihotriV.GuptaR.M.JoshiAerobic bacterial isolate from burn wound infections and their antibiograms – a five-year studyBurns302004241243
- A.E.HodleK.P.RichterR.M.ThompsonInfection control practices in U.S. burn unitsJ Burn Care Res2722006142151
- S.NaseerA.MabroukA.MaherColonization of Burn wounds in Ain shams University Burn UnitBurns292003229233
- MohammadImranMohammadFaheemViqarAslamAwalHakeemInayat Ur RehmanAzhar shah JPMI2342009304308
- M.Ansari LariM.AskarianEpidemiology of burns presenting to an emergency department in Shiraz, South IranBurns292003579581
- PavoniScandinavian J Trauma Resuscitation Emerg Med18201024
- Y.P.ZhangCommon pathogens in burn infections and changes in their drug sensitivityChinese J Plastic Surg Burns71991108110
- G.RevathiJ.PuriB.K.JainBacteriology of burnsBurns241998347349
- E.AkerlundF.HussF.SjobergBurns in Sweden: an analysis of 24.538 cases during the period 1987–2004Burn3320073136