
Abstract
Little is known about sexual activity in old age, particularly in Africa. The objective of this paper is to estimate years of sexually active life for older men and women, and examine the association between sexual activity and self-rated health status. Data were extracted from two large cross sectional HIV household surveys conducted in 2005 and 2012 in South Africa. The Sullivan method was used to estimate sexually active life expectancy, whilst logistic regression was used to assess associations with sexual activity. Sexually active life expectancy was higher among men across all the age groups in both surveys. At age 50, the sexually active life expectancy for men was double that for women – 2005 (12.6 vs. 5.9 years), 2012 (12.7 vs. 7.2 years). Self-rated health was significantly associated with sexual activity in men (adjusted Odds Ratio (aOR) 1.56; 95% CI 1.11-2.19; p < 0.001). Among older women, moderate exercise was associated with being sexual active, while HIV infection was significantly associated with reduced sexual activity. The presence of chronic conditions was also significantly associated with reduced sexual activity among men. The results confirm that older adults are sexually active, and that factors associated with sexual activity are different for men and women. HIV among women and chronic conditions among men are areas of intervention to improve sexual activity in older people.
Resumé
On sait peu de chose de l’activité sexuelle des personnes âgées, en particulier en Afrique. L’objectif de cet article est d’estimer les années de vie sexuelle active des hommes et femmes à un âge avancé, et d’examiner l’association entre activité sexuelle et état de santé auto-évalué. Les données proviennent de deux vastes enquêtes transversales sur le VIH menées auprès de ménages en 2005 et 2012 en Afrique du Sud. La méthode de Sullivan a été utilisée pour estimer l’espérance de vie sexuelle active, alors que la régression logistique a servi à évaluer les associations avec l’activité sexuelle. Dans les deux enquêtes, l’espérance de vie sexuelle active était plus élevée chez les hommes dans tous les groupes d’âge. À 50 ans, l’espérance de vie sexuelle active des hommes était deux fois celle des femmes – 2005 (12,6 contre 5,9 années), 2012 (12,7 contre 7,2 années). L’état de santé auto-évalué était sensiblement associé à l’activité sexuelle, alors que l’infection à VIH s’accompagnait significativement d’une activité sexuelle réduite. La présence de pathologies chroniques était aussi associée de manière significative à une réduction de l’activité sexuelle chez les hommes. Les résultats confirment que les adultes âgés sont sexuellement actifs et que les facteurs associés à l’activité sexuelle diffèrent entre hommes et femmes. Le VIH chez les femmes et les pathologies chroniques chez les hommes sont des domaines d’intervention pour améliorer l’activité sexuelle chez les personnes âgées.
Resumen
No se sabe mucho acerca de la actividad sexual en la tercera edad, particularmente en África. El objetivo de este artículo es estimar los años de vida sexual activa para hombres y mujeres de edad avanzada, y examinar la asociación entre la actividad sexual y un estado de salud autocalificado. Se extrayeron datos de dos importantes encuestas domiciliarias transversales sobre el VIH, realizadas en 2005 y 2012 en Sudáfrica. Se utilizó el método Sullivan para estimar la esperanza de vida sexual activa, y la regresión logística para evaluar las asociaciones con la actividad sexual. En ambas encuestas, la esperanza de vida sexual activa fue mayor entre hombres en todos los grupos de edad. A los 50 años, la esperanza de vida sexual activa de los hombres era el doble que la de las mujeres – 2005 (12.6 vs. 5.9 años), 2012 (12.7 vs. 7.2 años). La salud autocalificada estaba asociada de manera significativa con la actividad sexual en hombres (proporción de probabilidades ajustadas (aOR) 1.56; 95% CI 1.11-2.19; p < 0.001). Entre las mujeres de edad más avanzada, el ejercicio moderado estaba asociado con ser sexualmente activas, mientras que la infección por VIH estaba asociada con menor actividad sexual. La presencia de enfermedades crónicas también estaba asociada de manera significativa con menor actividad sexual entre hombres. Los resultados confirman que los adultos de edad más avanzada son sexualmente activos y que los factores asociados con la actividad sexual son diferentes para hombres y mujeres. El VIH entre mujeres y las enfermedades crónicas entre mujeres son áreas de intervención para mejorar la actividad sexual en personas mayores.
Introduction
The sexuality of older people is generally neglected.Citation 1 Little is known about the sexual activity of older people, especially in the African context with conservative social norms. Further, data on different indicators of sexual health including HIV prevalence, which are collected in major surveys such as the Demographic and Health Surveys (DHS), are typically collected only for individuals of reproductive age, i.e. from 15 to 49 years.Citation 2 It is assumed that people cease to be sexually active or no longer have sexual desires beyond 50 or 60 years of age. However, there is increasing evidence demonstrating that older women and men remain sexually active later in life.Citation 3,4 Data from the US national social, health and aging project (NSHAP) also shows that many older men and women in the US are sexually active even in their 80s.Citation 5 Similarly, evidence from five cohorts in South Africa, Uganda and Zimbabwe reveals that most men and fewer women remain sexually active in their 50s and 60s.Citation 6
Sexual intimacy is an important aspect of overall health, quality of life and emotional wellbeing throughout the life course.Citation 7,8 In later life, the importance of sexual activity and sexual health is increasingly being recognised as people live longer and remain healthy.Citation 8 It is important, therefore, to study sexual health beyond reproductive age.Citation 9 As life expectancy increases and older populations grow in low- and middle-income countries, projecting years of sexual activity is important in informing public health policy and programmes aimed at improving the sexual health of older people. At an individual level, knowledge of sexual life expectancy can motivate individuals to adopt healthy life styles, such as a healthy diet and regular exercise, that can prolong the sexually active lifespan. In addition, studies show that people living with HIV are also growing olderCitation 10 as a result of successful rollout of treatment efforts. This makes it imperative to understand the risks for HIV infection, sexual needs and desires of older people living with HIV. Older people are also at risk of being infected with HIV as they often underestimate the risk of infection.Citation 11,12
The aim of this paper is to better understand the extent of sexual activity in older age in South Africa, and to understand sexual health and needs in later life. The paper estimates sexually active life expectancy and examines the association between sexual activity and self-rated health status.
Methods
Data sources
The study is based on a secondary analysis of the 2005 and 2012 South African National HIV Incidence, Prevalence, Behaviour and Communication Survey (SABSSM) conducted in South Africa by the Human Sciences Research Council. Both surveys targeted persons above two years of age and residing in community dwellings. The sampling frame for the surveys was based on a master sample consisting of 1,000 census enumerator areas (EA) and 15 households per EA were randomly selected. The selection of EAs was stratified by province and locality type (formal urban settlements, informal/unplanned urban settlements, formal rural settlements, and tribal authority areas) and race (in urban localities). The surveys excluded institutionalized individuals (including those in educational institutions, military barracks, old age homes, or hospitals), who were hence not considered in the study. The surveys include a multistage cluster sample stratified by province and settlement geography (geotype), with the predominant population group in each area used. Further details about the sampling procedures are explained elsewhere.Citation 13,14 The household response rates were; 84.1% (2005)Citation 14 and 87.2% (2012).Citation 13 The individual response rates were; 96.0% (2005)Citation 14 and 89.1% (2012).Citation 13 In both surveys, socio-demographic and behavioural information was collected with participant’s consent through face-to-face questionnaires administered by trained fieldworkers. The sample used in this analysis included the ages 50 years and older.
Measures
Sexually active – Sexual activity was assessed by responses to the question “Have you had sex during the past 12 months”, which was asked with same wording in both surveys. Individuals responding in the affirmative were considered to be “sexually active”. This follows other studies.Citation 15
Self-rated health – This was assessed from the question “In general, would you say that your health is excellent, good, fair or poor?” The same wording of the question was used in both the 2005 and 2012 surveys. A binary variable was created by categorising; excellent and good as ‘good health’ and fair and poor as ‘poor health’.
Chronic conditions – In the SABSSM surveys a general question was asked on the presence of any chronic condition:
“Do you have any chronic medical condition that is affecting what you do or how you feel?”
This assessment is based on self-reports, and respondents who answered ‘Yes’ were considered to have a chronic condition.
HIV status – Dried blood spot (DBS) specimens for HIV testing were collected from each participant who assented or consented using finger prick. Samples were tested for HIV using an enzyme immunoassay (EIA) and samples which tested positive were retested using a second EIA. A third EIA was used for any samples with discordant results on the first two EIAs.
Exercise – Two questions were asked to assess whether the respondent did any form of exercise. The first question was:
“Do you do any vigorous intensity sport, fitness or recreational activities in your leisure or spare time, that cause large increases in breathing or heart rate (like running or strenuous sports, weightlifting) for three times a week at least 30 minutes at a time?”
And the second question was
“Do you do any moderate-intensity sport, fitness or recreational activities in your leisure or spare time that cause small increases in breathing and heart rate (like brisk walking, cycling or swimming) for three times a week at least 30 minutes at a time?”
Analysis
The Sullivan methodCitation 16,17 was used to calculate the sexually active life expectancies, which is the number of remaining sexually active years an individual can expect to live at a particular age. This is a new concept recently introduced by Lindau and Gavrilova.Citation 15 It is an extension of healthy expectancy indicators, which have become important measures of summarising population health. The Sullivan method requires age-specific mortality information taken from a period life table and information on the age-specific prevalence of the health status usually obtained from cross-sectional surveys. The prevalence data is used to partition person-years lived in the life table population, implied by current mortality rates, into healthy and unhealthy years. In this case, age-specific prevalence of sexual activity was used to divide the number of person-years lived into years with and without sexual activity. The prevalence data of sexual activity was obtained from the 2005 and 2012 national HIV household surveys mentioned above. The Sullivan method was used in this study because it provides a means of making comparisons for two groups, in this case men and women, and two time points. The purpose of using the two surveys was to establish the trend of sexual activity over time. Life expectancy estimates were obtained from UN Life TablesCitation 18 for 2005-2010 and 2010-2015, i.e. for the corresponding 2005 and 2012 surveys. Standard errors and confidence intervals were calculated from the formulae suggested by the International Network on Health Expectancy.Citation 19
Multiple logistic regression was used to model the likelihood of being sexually active. The main variable of interest was self-rated health, and covariates included: age, marital status, exercises (vigorous or moderate intensity), HIV status and presence of chronic medical conditions. The data were analysed using STATA 12,Citation 20 incorporating the complex sampling design of the two surveys by using the ‘svy’ commands in obtaining all estimates. The analysis here was restricted to older people aged 50 years and over. The association between the outcome and exposure variables was assessed by the odds ratios (OR) and 95% confidence intervals (95% CI). All variables statistically significant (p < 0.05) in univariate analyses were included in the multivariable models. The models were fitted separately for men and women.
Results
Sample characteristics, self-rated health and sexual activity
shows the distribution of the sample of older adults (50 years and above) across socio-demographic and behavioural characteristics. In both surveys, the majority of adults were in the age group 50-59 years and still married, although a significant proportion were widowed. Wide gender differentials existed in widowhood, that is, the proportion of adult women who were widowed was four and three times that of adult men in the 2005 and 2012 surveys, respectively. Most of the adults had attained primary education, with more men having completed high school and tertiary education than women. Almost two thirds of the adults across gender in both surveys were Black Africans. The prevalence of poor and fair health was higher among women than men in both surveys. Older men were significantly more likely to report being sexually active than women (p < 0.001). However, the prevalence of sexual activity among older women slightly increased over time, from 28.8% in 2005 to 33.8% in 2012.
Table 1 Descriptive characteristics of sample 50 years and older by gender, 2005 and 2012, SABSSM survey.
Factors associated with sexual activity
Among indicators included in the study, good health was strongly associated with sexual activity in older men (aOR 1.56; 95% CI 1.11-2.19). As expected, increasing age was strongly associated with reduced odds of being sexually active for both sexes. Older people who were single were less likely to be sexually active. Women who engaged in moderate exercise were twice as likely to be sexually active compared to those who did not (aOR 1.99; 95%CI 1.32-3.00). Presence of a chronic medical condition among men (aOR 0.64; 95% CI 0.46-0.91) significantly reduced sexual activity, whilst HIV reduced sexual activity in older women by almost half (aOR 0.52; 95%CI 0.27-0.98) ( ).
Table 2 Factors associated with sexual activity among older adults (50 years and older), 2012 SABSSM survey.
Sexually active life expectancies
The total life expectancy in South Africa is higher for women than men across all ages ( ). According to 2012 data, a 50-year old woman would be expected to live on average 29 years longer compared to 24 years for men. However, in both surveys men had consistently higher sexually active life expectancy. A 50-year old man would have expected to live a sexually active life for another 12.7 years in 2012, whilst a woman of the same age would only be estimated to be sexually active for 7.2 years. The gender differences persist across age groups and widen further with age. For example, at age 70, the estimated sexually active years are 3.0 for men and 1.0 for women.
Table 3 Gender differences in sexually active life expectancy by health status at ages 50, 60, 70 and 80, based on the 2005 and 2012 SABSSM surveys.
In women, there was a positive change in sexually active life expectancy from 2005 to 2012. The gains were significant in all age groups with the exception of the last age group (80 +). Men in good health at age 80 and above had significant gains in sexually active life in the period 2005-2012. and show the sexually active life expectancy by health status and gender for 2005 and 2012 respectively. In both years, men and women in good health had higher sexually active life expectancy compared to those in poor health. The gap between the curves (good and poor health) appears to be much wider in men, especially from the 2012 survey.
Figure 1. Sexually active life expectancy in South African men and women in Good or Poor Health, based on 2005 SABSSM surveys.
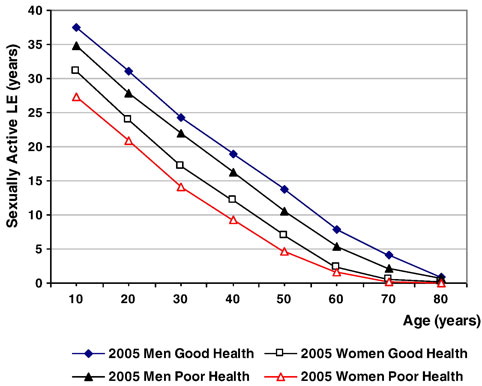
Figure 2. Sexually active life expectancy in South African men and women in Good or Poor Health, based on 2012 SABSSM surveys.

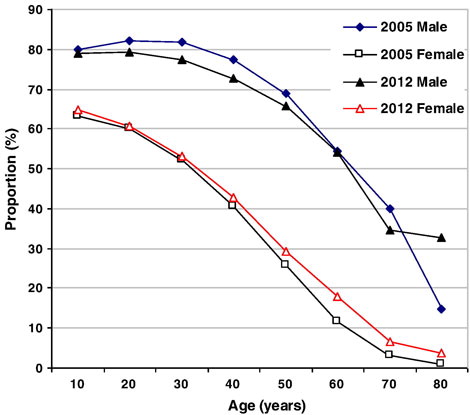
also gives a summary of the proportion of remaining years spent as sexually active. This was derived as years of sexual activity as a fraction of total remaining years of life. From the 2012 survey, the proportion for men is actually double that for women (65.7 vs. 29.4%) at age 50. shows a wide gap between men and women across all ages in the proportion of remaining life spent sexually active. However, when comparing data from 2005 and 2012, it can be seen that the proportion dropped among men, whilst some increases can be seen among women, especially at the oldest ages. The estimates at the oldest ages are less stable and need to be interpreted with caution due to the smaller sample sizes at these ages.
Figure 3. Proportion of remaining sexually active life for men and women, 2005 and 2012.
Discussions
This study was aimed at projecting estimates of sexually active life expectancy, and examining factors associated with sexual activity in older people. The factors explored in this study include: age, marital status, HIV status, exercise and presence of chronic medical conditions. Data from this South African study show that older people are still sexually active and, if anything, they are actually staying sexually active longer. This means that the myth that older people are ‘asexual’ needs to be dispelled. HIV prevention, mitigation and support programmes need to be spilled over beyond the conventional reproductive age group to the old and even oldest ages. Total life expectancy in South Africa has started to rise steadily again after being brought down by AIDS during the last decade 2000-2010.Citation 21,22 Along with these gains, sexually active life expectancy seems to be increasing as well.
The estimates of sexually active life expectancy found in this study are lower than those found in the NSHAP and the national survey of midlife development in the United States (MIDUS) from the USA.Citation 15 Whereas the estimates from the 2012 survey in this study at 55 years were 12.1 years (men) and 5.5 years (women), the corresponding estimates from the USA study were 14.9 and 10.6 years for men and women respectively. This shows that older people in the USA remain sexually active for a longer time beyond age 55 compared to older people in South Africa. For men, the estimates from the two studies are close, whilst the estimates for US women are double that of South African women. However, it is important to note that the MIDUS study was specifically targeted for older people whilst the SABSSM surveys used in this study included all ages above two years. Further, the data from the former was collected via telephone whilst face-to-face interviews were used for the latter. These differences in design, the exact wording of questions, and differential recall bias could limit direct comparison of estimates from the two studies. Nevertheless, regardless of these differences, the gap in women between the two studies is worth noting. Other factors such as culture, ethnicity, religion, and socio-economic factors have been found to explain regional differences in sexual activity in older people.Citation 23
The results corroborate previous studies which found that sexual activity was reported more among men and those in unions.Citation 24 Similar to other studies,Citation 7,15 this study has shown that poor health status is associated with decreased sexual activity. Other studies also found that due to decline in ‘strength’ among men, they could no longer perform the sexual act despite having the desire to do so.Citation 25,26 This further supports other studies which have found that it is poor health, rather than age per se, that is associated with a decline in active sex life.Citation 27,28 This is an important finding which goes along with new understanding among demographers and policy makers that aging is not about numbers, but rather more about other dimensions of life such as health, functioning and well-being. In other words, defining aging based on chronological age might be misleading.Citation 26,29,30
The study findings have significant policy implications. It is interesting to note that HIV reduces sexual activity amongst older women, whilst chronic conditions seem to limit sexual activity among older men. This implies that there is need for gender responsiveness and sensitivity when addressing sexual health among the elderly, since the underlying determinants are different. More research is also needed to gain more in-depth understanding of underlying factors and implications on health and well-being. Adult sexuality studies such as the Global Study of Sexual Attitudes and Behaviours (GSSAB)Citation 4 and othersCitation 27 have reported that chronic conditions such as vascular and prostate conditions lead to declines in sexual activity. Other conditions include diabetes mellitus, which can lead to impotence and osteoarthritis, which causes poor mobility, and others, such as depression, which are prevalent at these ages. Further, medications taken for chronic conditions have been known to reduce libido, hence limiting sexual activity.Citation 31 Risk factors for chronic conditions are largely behavioural, and can be mitigated at an earlier age. It is important therefore to ensure prevention programmes for chronic conditions among young men. Based on the results of this study, there is need to raise awareness about the negative effect chronic conditions might have on sexual activity later in life.
Studies have also shown higher HIV-related mortality in males than in females.Citation 32 Therefore, the results might suggest that HIV-infected women are less likely to be sexually active because most are likely to be widows. In later life, women are more likely to be without a partner because they outlive men. Further, women are less likely to remarry following the death of a partner at this age compared to men.Citation 24 On the other hand, HIV does not seem to deter men from sexual activity. These results have important implications on public health policies aimed at primary and secondary prevention of HIV, given the aging of people living with HIV. Studies have reported that older people are less likely to use condoms and get tested for HIV, and more likely to have multiple partners.Citation 33–35 Sexual health concerns of women are less well understood than those of men.Citation 27 Therefore, further research is needed to further understand the sexuality of older women, also in the context of HIV. In this study, there was an association between moderate exercise and sexual activity in women but not in men. This finding is in contrast to a study from Taiwan which did not find significant associations between regular exercise and maintaining sexual activity.Citation 36 However, the Taiwan study found that self-reported capacity for daily activities was associated with sexual activity.Citation 36 Further research is needed on the influence of exercise on sexual activity, and how this could be promoted in older people in South African setting.
Strengths and limitations
The strength of this study is that it is based on two cross-sectional nationally representative surveys, with relatively larger sample sizes of older people. This helps to check trends of estimates over the years. The two surveys asked similar question for the outcome and main exposure variables, which strengthens content validity. Sex in this study was defined as being penetrative. However, a qualitative study from the UK noted that ‘sex’ at old age may have other meaning and forms, such as cuddling and touching, which still maintain physical intimacy.Citation 28 This is important when penetrative sex is no longer possible. Hence, the narrow definition of sex used in this study could be a limitation and could result in underestimating the level of sexual activity in both sexes. In-depth qualitative studies are required to understand the various meanings and forms of sex at old ages within a South African context. The Sullivan method used in this study does not take account of the possibility of recovery from ill-health.Citation 17 However, the estimates derived using the method have been shown to be unbiased and consistent under the assumption of a stationary population,Citation 37 and to be close to those from other methods e.g. multi-state life tables, which utilize longitudinal data.Citation 38 However, the limits of cross sectional data exist. The SABSSM surveys did not include institutionalized individuals in the sample and the exclusion of older people living in institutions means that the results are not representative of this important segment of the elderly population. Unfortunately, there are no surveys on sexuality of older institutionalized populations from which this information could possibly have been obtained. Further, although not mentioned anywhere, bias in reporting sexual activity cannot be ruled out. It can be suspected that older women are less likely to report sexual activity, especially if they are not married or in union, due to possibilities of being stigmatized as having ‘loose’ morals. On the other hand, men can over-report sexual activity because it is associated with manhood, and for covering up sexual dysfunction.Citation 39
Conclusions
This paper contributes to the sparse literature on sexuality of older people in South Africa. The projection of patterns of sexual activity at old age is useful for predicting need for public health services related to improving sexual health, and preventing HIV or risky sexual behaviour. The results show that older adults are sexually active, and that factors associated with sexual activity are different for men and women. HIV among women and chronic conditions among men are areas of intervention to improve sexual activity in old people.
Acknowledgements
The data used in this study were obtained from the South African National HIV Incidence, Prevalence, Behaviour and Communication Survey (SABSSM). The surveys are funded by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC) under the terms of 5U2GGH000570. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of CDC. The authors are grateful to Prof Sandra Reynolds for her comments on the manuscript.
Related Research Data
References
- B.L. Walker. Sexuality and the elderly: A research guide. 1997
- J.C. Negin, R.G. Cumming. HIV infection in older adults in sub-Saharan Africa: extrapolating prevalence from existing data. Bulletin of the World Health Organization. 88: 2010; 1847–1853.
- J. Negin, A. Rozea, A.L. Martiniuk. HIV behavioural interventions targeted towards older adults: a systematic review. BMC Public Health. 14(1): 2014; 1.
- E.O. Laumann, A. Nicolosi, D.B. Glasser, et al. Sexual problems among women and men aged 40–80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. International Journal of Impotence Research. 17(1): 2005; 39–57.
- S.T. Lindau, P. Schumm, E.O. Laumann, et al. A Study of Sexuality and Health among Older Adults in the United States. New England Journal of Medicine. 35: 2007.
- J. Todd, I. Cremin, N. McGrath, et al. Reported number of sexual partners: comparison of data from four African longitudinal studies. Sexually Transmitted Infections. 85: 2009; i72–i80.
- D.M. Lee, J. Nazroo, D.B. O’Connor, et al. Sexual health and well-being among older men and women in England: findings from the English Longitudinal Study of Ageing. Archives of Sexual Behavior. 45(1): 2016; 133–144.
- W.P. Bouman, J. Arcelus, S.M. Benbow. Nottingham Study of Sexuality & Ageing (NoSSA I). Attitudes regarding sexuality and older people: A review of the literature. Sexual and Relationship Therapy. 21(02): 2006; 149–161.
- World Health Organization. Defining sexual health: report of a technical consultation on sexual health, 28-31 January 2002. 2006; World Health Organization: Geneva
- J. Negin, R.C. Bennett, E. Lelerai, et al. HIV Attitude, Awareness and Testing among Older Adults in Africa. AIDS and Behavior. 16: 2011; 63–68.
- C. Wallrauch, T. Barnighausen, M. Newell. HIV infection of concern also in people 50 years and older in rural South Africa. South African Medical Journal. 100(12): 2010; 812–814.
- G.P. Schmid, B.G. Williams, J.M. Garcia-Calleja, et al. The unexplored story of HIV and ageing. Bulletin of the World Health Organization. 87(3): 2009; 162-A.
- O. Shisana, D. Labadarios, L. Simbayi, et al. South African national HIV prevalence, incidence and behaviour survey, 2012. 2015; HSRC Press: Cape Town
- O. Shisana, T. Rehle, L. Simbayi, et al. South African national HIV prevalence incidence behaviour and communication survey 2008: a turning tide among teenagers?. 2009; HSRC Press: Cape Town
- S.T. Lindau, N. Gavrilova. Sex, health, and years of sexually active life gained due to good health: evidence from two US population based cross sectional surveys of ageing. BMJ. 340: 2010; c810.
- D.F. Sullivan. A single index of mortality and morbidity. HSMHA Health Reports. 86(4): 1971; 347–354.
- C. Jagger, J.M. Robine. Healthy life expectancy. International handbook of adult mortality. 2011; Springer: Netherlands 551–568.
- U. DeSA. World population prospects: the 2012 revision. 2013; Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat: New York
- C. Jagger, B. Cox, S. Le Roy, E. Team. Health Expectancy Calculation by the Sullivan Method. 2006
- StataCorp. Stata Statistical Software. Release 122011.
- J. Bor, A.J. Herbst, M.L. Newell, et al. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 339(6122): 2013; 961–965.
- B.M. Mayosi, S.R. Benatar. Health and health care in South Africa – 20 years after Mandela. New England Journal of Medicine. 371(14): 2014; 1344–1353.
- F.E. Kaiser. Sexuality in the elderly. Urologic Clinics of North America. 23(1): 1996; 99–109.
- T.F. Wang, C.H. Lu, I.J. Chen, et al. Sexual knowledge, attitudes and activity of older people in Taipei, Taiwan. Journal of Clinical Nursing. 17(4): 2008; 443–450.
- S. Van der Geest. “No strength”: sex and old age in a rural town in Ghana. Social Science & Medicine. 53(10): 2001; 1383–1396.
- E.K. Freeman, E. Coast. Sex in older age in rural Malawi. Ageing and Society. 34(07): 2014; 1118–1141.
- M.A. Taylor, A. Gosney. Sexuality in older age: essential considerations for healthcare professionals. Age and Ageing. 40: 2011; 538–543.
- M. Gott, S. Hinchliff. How important is sex in later life? The views of older people. Social Science & Medicine. 56(8): 2003; 1617–1628.
- W. Sanderson, S. Scherbov. Rethinking Age and Aging. Population Bulletin. 63(4): 2008; 3–16.
- W.C. Sanderson, S. Scherbov. Remeasuring aging. Science. 329(5997): 2010; 1287–1288.
- B. Kessel. Sexuality in the older person. Age and Ageing. 301(2): 2001; 121–124.
- M. Cornell, M. Schomaker, D.B. Garone, et al. Gender differences in survival among adult patients starting antiretroviral therapy in South Africa: a multicentre cohort study. PLoS Medicine. 9(9): 2012; e1001304.
- C.M. Gott. Sexual activity and risk-taking in later life. Health & Social Care in the Community. 9(2): 2001; 72–78.
- K. Peltzer, N. Phaswana-Mafuya, T. Mzolo, et al. Sexual behaviour, HIV status, and HIV risk among older South Africans. Journal of Ethnobiology and Ethnomedicine. 4(3): 2010; 163–172.
- E. Freeman, P. Anglewicz. HIV prevalence and sexual behaviour at older ages in rural Malawi. International Journal of STD & AIDS. 23(7): 2012; 490–496.
- M. Young, T. Penhollow. Sexual desirability and sexual performance: Does exercise and fitness really matter. Electronic Journal of Human Sexuality. 7: 2004.
- K. Imai, S. Soneji. On the estimation of disability-free life expectancy: Sullivan’s method and its extension. Journal of the American Statistical Association. 102(480): 2007; 1199–1211.
- C.D. Mathers, J.-M. Robine. How good is Sullivan’s method for monitoring changes in population health expectancies?. Journal of Epidemiology and Community Health. 51(1): 1997; 80–86.
- B. Kumar, S. Gupta. Sexually transmitted infections. 2014; New Delhi: Elsevier Health Sciences