
Abstract
Talaromyces (Penicillium) marneffei is an important pathogenic thermally dimorphic fungus causing systemic mycosis in Southeast Asia. The clinical significance of T. marneffei became evident when the human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome epidemic arrived in Southeast Asia in 1988. Subsequently, a decline in the incidence of T. marneffei infection among HIV-infected patients was seen in regions with access to highly active antiretroviral therapy and other control measures for HIV. Since the 1990s, an increasing number of T. marneffei infections have been reported among non-HIV-infected patients with impaired cell-mediated immunity. Their comorbidities included primary adult-onset immunodeficiency due to anti-interferon-gamma autoantibodies and secondary immunosuppressive conditions including other autoimmune diseases, solid organ and hematopoietic stem cell transplantations, T-lymphocyte-depleting immunsuppressive drugs and novel anti-cancer targeted therapies such as anti-CD20 monoclonal antibodies and kinase inhibitors. Moreover, improved immunological diagnostics identified more primary immunodeficiency syndromes associated with T. marneffei infection in children. The higher case-fatality rate of T. marneffei infection in non-HIV-infected than HIV-infected patients might be related to delayed diagnosis due to the lack of clinical suspicion. Correction of the underlying immune defects and early use of antifungals are important treatment strategies. Clinicians should be familiar with the changing epidemiology and clinical management of T. marneffei infection among non-HIV-infected patients.
INTRODUCTION
Talaromyces (Penicillium) marneffei is an important pathogenic thermally dimorphic fungus causing systemic mycosis in Southeast Asia.Citation1, Citation2, Citation3 T. marneffei is a member of the family Trichocomaceae, order Eurotiales, class Eurotiomycetes, division Ascomycota. It is the only member in the Talaromyces genus which is considered to be an important human pathogen. T. marneffei infection is endemic in tropical regions, especially Thailand, Vietnam, northeastern India, Southern China, Hong Kong, Taiwan, Laos, Malaysia, Myanmar, Cambodia and Laos.Citation1 The fungus was first isolated from the hepatic lesions of a bamboo rat (Rhizomys sinensis) which died spontaneously from the infection in 1956.Citation4 Subsequent studies showed that bamboo rats (Rhizomys sp. and Cannomys sp.) and soil from their burrows were important enzootic and environmental reservoirs of T. marneffei, respectively.Citation4, Citation5, Citation6, Citation7 The prevalence of T. marneffei infection in these susceptible animal species varies widely across Southeast Asia. Historically, T. marneffei infection in human has been considered to be exclusively associated with acquired immunodeficiency syndrome (AIDS) caused by human immunodeficiency virus (HIV) infection.Citation1, Citation8 In some regions such as Hong Kong and southern China, T. marneffei infection has long been considered as one of the top three AIDS-defining opportunistic infections, alongside tuberculosis and cryptococcosis.Citation2, Citation9 In recent years, improved treatment of HIV infection with highly active antiretroviral therapy and control of the HIV/AIDS epidemic with other measures have led to a change in the epidemiology of T. marneffei infection, with an increasing number and proportion of cases being reported in non-HIV-infected patients who had other immunocompromising conditions (). T. marneffei infection in non-HIV-infected children has been discussed elsewhere.Citation10 In this article, we thoroughly reviewed the epidemiological and clinical characteristics of T. marneffei infection among non-HIV-infected adult patients, and discussed on the specific management strategies for each at-risk group.
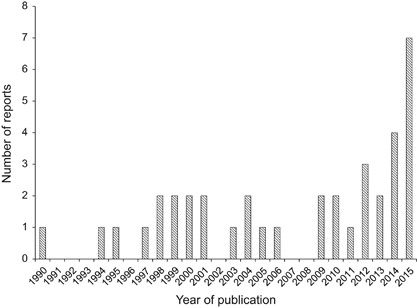
Figure 1 The number of reports of Talaromyces marneffei infection in non-HIV-infected adult patients described in the English-language literature between 1 January 1990 and 1 October 2015. Reports involving patients with uncertain human immunodeficiency virus infection status were excluded.
THE CHANGING EPIDEMIOLOGY OF T. MARNEFFEI INFECTION
The first human case of T. marneffei infection occurred as a laboratory-acquired infection in 1959Citation11 (). A laboratory researcher accidentally inoculated the fungus into his own finger while performing experiments on mice and caused a localized small nodule at the inoculation site.Citation11 The first natural human case of infection was reported in 1973 and involved an American minister with Hodgkin’s disease who resided in Southeast Asia.Citation12 Over the next 10 to 15 years, a few more sporadic cases were reported in Thailand, Hong Kong and southern China.Citation13, Citation14, Citation15, Citation16, Citation17, Citation18, Citation19, Citation20, Citation21, Citation22 The HIV status of most of these patients was not known as the virus was not discovered until 1981 and laboratory diagnostics for HIV infection was not readily available in Southeast Asia in the early 1980s. The incidence rate of T. marneffei infection markedly increased after the HIV/AIDS epidemic arrived in Southeast Asia in 1988.Citation1 T. marneffei infection was reported not only among HIV-infected patients residing in endemic areas, but also in HIV-infected patients who had traveled to these endemic areas.Citation1
Figure 2 Major milestones in the changing epidemiology of Talaromyces marneffei infection. HAART, highly active antiretroviral therapy; HIV, human immunodeficiency virus; IFN-γ, interferon-gamma; mAb, monoclonal antibodies.
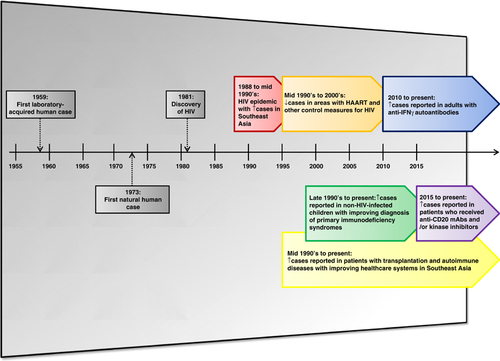
The economic boom in Southeast Asian countries since the 1990s was accompanied by an improvement in their healthcare infrastructures. These included better control of HIV infection and improved diagnosis of non-AIDS conditions associated with impaired cell-mediated immunity. The availability of highly active antiretroviral therapy and other control measures for the HIV/AIDS epidemic led to a decrease in the incidence rate of HIV-associated T. marneffei infection.Citation1 On the other hand, T. marneffei infection was increasingly reported in different groups of patients with primary or secondary immunocompromising conditions (). The use of potent immunosuppressive drugs in patients with transplantation and autoimmune diseases was associated with an increased incidence of T. marneffei infection among these non-HIV-infected patients since the mid 1990s. Improved genetic testing for various primary immunodeficiency syndromes led to the recognition of more cases of T. marneffei infection in non-HIV-infected children.Citation10, Citation23 The recently identified association between T. marneffei infection and the adult-onset immunodeficiency syndrome caused by anti-interferon-gamma (anti-IFN-γ) autoantibodies helped to explain many previous cases of T. marneffei infection among non-HIV-infected adult Asian patients who had no other comorbidities.Citation24 Recently, T. marneffei infection was also observed in non-HIV-infected hematology patients who were treated with novel targeted therapies including anti-CD20 monoclonal antibodies and kinase inhibitors.Citation25, Citation26
OVERVIEW OF THE IMMUNOLOGICAL BASIS AND CLINICAL CHARACTERISTICS OF T. MARNEFFEI INFECTION IN NON-HIV-INFECTED ADULT PATIENTS
T. marneffei proliferates in macrophages and disseminates via the reticuloendotheial system.Citation1 Clinically, the infection is characterized by fungal invasion of multiple body organ systems, especially blood, bone marrow, skin, lungs and reticuloendothelial tissues.Citation1 Similar to other intracellular pathogens, the activation of macrophages by T-lymphocyte-derived cytokines, especially those of the Th1 response such as interleukin (IL)-12, IFN-γ and tumor necrosis factor (TNF)-α, is important for host defense against T. marneffei infection.Citation27 This is supported by the observation that T. marneffei infection in nude or T-lymphocyte-depleted mice was invariably fatal, whereas the fungus could be cleared within three weeks in healthy mice.Citation28, Citation29 A polarized Th1 response prevented immunoevasion by T. marneffei in parasitized mononuclear phagocytes and stimulated macrophage killing of intracellular T. marneffei via the L-arginine-dependent nitric oxide pathway.Citation30, Citation31 Furthermore, granuloma formation, which is important for containment of the fungus, was found in wild-type mice but not in IFN-γ-knocked out mice.Citation27 These evidences suggest that patients with defective cell-mediated immunity may be at risk of developing T. marneffei infection.
The severity of the infection varies among patients with different degrees of immunosuppression. In HIV-infected patients, T. marneffei infection is often disseminated and involves multiple organs.Citation1, Citation2 In non-HIV-infected patients, the infection may be focal or disseminated, depending on the underlying immunocompromising condition and the timing of diagnosis. In a retrospective cohort study involving 116 HIV-infected and 34 non-HIV-infected patients with T. marneffei infection in Thailand, it was found that the non-HIV-infected patients were significantly older, less likely to have fever, splenomegaly and umbilicated skin lesions, and more likely to have Sweet’s syndrome and osteoarticular lesions.Citation32 The non-HIV-infected patients also had higher leukocyte, CD4 lymphocyte and platelet counts, and lower alanine transaminase level and blood culture-positive rate.Citation32
To further analyze the clinical characteristics of non-HIV-infected patients with T. marneffei infection, we reviewed the reports of non-HIV-related T. marneffei infection in the English-language literature found in a PubMed search using the key words ‘Talaromyces’, ‘Penicillium’, ‘marneffei’ and ‘penicilliosis’ on 1 October 2015. Reports involving patients with uncertain HIV status were excluded. A total of 119 patients with detailed clinical information were identified (). There were 65 males and 54 females. Their median age was 42.8 years (range, 22 to 79 years). Common clinical features of T. marneffei infection among these non-HIV-infected patients included fever, malaise, weight loss, skin and soft tissue lesions, hepatosplenomegaly, lymphadenopathy, cough and dyspnea (). Some patients also had osteoarticular involvement and abdominal symptoms such as abdominal pain and diarrhea due to mesenteric lymphadenopathy or terminal ileitis mimicking Crohn’s disease. Less common clinical features included tracheomediastinal fistula and neurological manifestations such as seizure and confusion due to the presence of intracranial lesions. Laboratory investigations often revealed leukocytosis or leukopenia, anemia, thrombocytosis, deranged liver function test results and elevated inflammatory marker levels including those of C-reactive protein and erythrocyte sedimentation rate. Patients with pulmonary involvement exhibited various chest X-ray abnormalities, including uni- or multi-lobar consolidations, cavities, interstitial infiltrates, pleural effusion, pericardial effusion and enlarged hilar shadow due to mediastinal and hilar lymphadenopathies.
Table 1 Talaromyces marneffei infection in non-HIV-infected adult patientsFootnotea
Table 2 Clinical and laboratory features of Talaromyces marneffei infections in non-HIV-infected adult patientsFootnotea
Overall, 33/119 (27.7%) non-HIV-infected patients with T. marneffei infection died despite most of them having received antifungal treatment with anti-T. marneffei activity, such as amphotericin B, itraconazole and voriconazole (). This case-fatality rate was similar to that of non-HIV-infected patients with T. marneffei infection in another study, in which 10/34 (29.4%) died.Citation32 Both of these rates were higher than that of HIV-infected patients (24/116, 20.7%) in the same cohort, and might reflect delayed diagnosis of T. marneffei infection among non-HIV-infected patients due to the lack of clinical suspicion in the early stage. Notably, many of the non-HIV-infected patients with T. marneffei infection were initially misdiagnosed and empirically treated as tuberculosis because both infections are endemic in Southeast Asia, have similar predisposing factors and overlapping clinical manifestations (). The diagnosis of T. marneffei infection in these patients was often established weeks to months later when the clinical condition failed to improve to empirical anti-tuberculosis treatment. Moreover, some of the patients residing in non-endemic regions only became symptomatic months to years after returning from endemic areas.Citation56, Citation59 These factors likely led to delayed commencement of appropriate antifungal treatment. Familiarity with the non-AIDS conditions associated with T. marneffei infection would facilitate clinicians to improve the clinical management of the infection among these at-risk patients.
SPECIFIC CHARACTERISTICS OF NON-AIDS CONDITIONS ASSOCIATED WITH T. MARNEFFEI INFECTION
Anti-IFN-γ autoantibodies
Immunodeficiency due to anti-IFN-γ autoantibodies is an emerging adult-onset immunodeficiency syndrome first described in 2004.Citation68, Citation69 The affected patients have high-titer serum neutralizing anti-IFN-γ autoantibodies that inhibit STAT1 phosphorylation and IL-12 production, leading to a severely compromised Th1 response.Citation70 As a result, these patients develop recurrent, severe and/or disseminated opportunistic infections caused by various intracellular pathogens.Citation24, Citation70 Over the past decade, this condition has been increasingly reported among adult Asian patients, including Filipino, Thai, Vietnamese, Japanese and Chinese residents in Hong Kong, Taiwan and mainland China.Citation24, Citation57, Citation70, Citation71, Citation72, Citation73, Citation74, Citation75 This ethnic predilection is likely related to genetic predispositions among Asians. Recently, the association between anti-IFN-γ autoantibodies and HLA class II alleles, including HLA-DR*15:02/16:02 and HLA-DQ*05:01/05:02, was reported.Citation72, Citation76
As the initial reports mostly involved patients residing in areas non-endemic of T. marneffei, only non-tuberculous mycobacteriosis was recognized as an important opportunistic pathogen in these patients.Citation68, Citation69, Citation77 It was not until 2010 when the association between anti-IFN-γ autoantibodies and T. marneffei infection was described among eight Chinese patients living in Hong Kong.Citation24 The susceptibility of patients with anti-IFN-γ autoantibodies to other intracellular pathogens including non-typhoidal Salmonella sp., Burkholderia sp., varicella zoster virus and less commonly, Histoplasma capsulatum and Cryptococcus neoformans, was also recognized subsequently.Citation24, Citation70 T. marneffei infections in patients with anti-IFN-γ autoantibodies usually manifest as fever of unknown origin, cervical lymphadenitis and/or mild symptomatic infection with positive serology.Citation24 Occasionally, T. marneffei infection or non-tuberculous mycobacteriosis might precipitate the development of reactive dermatoses such as Sweet’s syndrome, erythema nodosum, exanthematous pustulosis and pustular psoriasis, or cause direct infective cutaneous lesions in these patients.Citation51
The treatment of T. marneffei infection in patients with anti-IFN-γ autoantibodies comprises of both effective antifungal therapy and immunomodulation to control the underlying immunological defect. These patients often responded poorly or developed recurrent infections when they were treated with antifungal therapy alone. The most effective immunomodulating treatment available currently is rituximab, an anti-CD20 antibody which targets B lymphocytes to reduce the production of serum-neutralizing anti-IFN-γ autoantibodies.Citation78, Citation79 However, since rituximab has recently been identified as a potential risk factor for T. marneffei infection, a delicate balance to minimize the level of anti-IFN-γ autoantibodies, while not over-suppressing the immune system, needs to be established.Citation25 The dosing regimen and time intervals of administering rituximab in patients with anti-IFN-γ autoantibodies should be further evaluated in larger clinical trials.
Other autoimmune diseases
T. marneffei infection has been reported in at least 15 patients with various other autoimmune diseases, including systemic lupus erythematosus (SLE), mixed connective tissue disease, Sjögren’s syndrome, primary biliary cirrhosis, primary immune (idiopathic) thrombocytopenia and autoimmune hemolytic anemia.Citation32, Citation34, Citation35, Citation36, Citation37, Citation40, Citation41, Citation43, Citation45, Citation53, Citation54, Citation80 Although the immunological defects of these autoimmune diseases were variable, the predisposing factors for T. marneffei infection could be broadly classified into treatment-related and disease-related. In patients with organ- or tissue-specific conditions, such as Sjögren’s syndrome, primary biliary cirrhosis, primary immune thrombocytopenia and autoimmune hemolytic anemia, the degree of systemic immunosuppression was usually not severe. Therefore, T. marneffei infection usually occurred when these patients received high-dose or prolonged treatment with T-lymphocyte-depleting drugs, including corticosteroids, cyclosporine, azathioprine, tacrolimus and mycophenolate mofetil. Treatment of T. marneffei in these patients usually required a reduction of immunosuppressive drugs together with antifungal therapy. In patients with SLE or mixed connective tissue disease who had more severely compromised cell-mediated immunity, T. marneffei infection might occur even with less immunosuppressive therapy. In patients with active SLE, marked lymphopenia may occur in the absence of immunosuppressive therapy and is an important risk factor for not only T. marneffei infection, but also opportunistic infections caused by other intracellular organisms such as Mycobacterium tuberculosis, non-tuberculous mycobacteria, Nocardia sp., Rhodococcus sp., Burkholderia pseudomallei, C. neoformans, Pneumocytis jirovecii, Toxoplasma gondii and herpesviruses.Citation81, Citation82 The management of T. marneffei infection in these patients thus requires both effective antifungal agents and careful titration of immunosuppressive therapy to control the underlying lupus activity.
Organ transplantation
T. marneffei infection has been occasionally reported in solid organ transplantation and hematopoietic stem cell transplantation (HSCT) recipients. Most of these patients developed T. marneffei infection when escalated doses of immunosuppressive drugs were used to treat graft rejection. T. marneffei infection was otherwise uncommon among transplantation recipients who had minimal maintenance anti-rejection therapy. The most common type of transplantation associated with T. marneffei infection was renal transplantation, with at least 12 cases having been reported.Citation22, Citation36, Citation38, Citation41, Citation44, Citation45, Citation46, Citation52, Citation56, Citation83 T. marneffei infection has also been uncommonly reported in liver transplantation, lung transplantation and HSCT recipients on multiple T-lymphocyte-depleting immunosuppressive drugs.Citation47, Citation66, Citation80, Citation84
Due to the small number of cases, it is difficult to determine the reasons for the apparently higher incidence of T. marneffei infection among renal than other solid organ transplantation and HSCT recipients. Possible reasons include the earlier adoption and higher annual number of renal transplantation than the other types of transplantation in T. marneffei-endemic areas, and the different antifungal prophylaxis regimens used in these transplantation recipients. For example, in Hong Kong, the first cadaveric and living-related donor renal transplantations were performed in 1969 and 1980, respectively.Citation85 The first HSCT was performed in 1990, and the first liver and lung transplantations were performed in 1991 and 1995, respectively.Citation86, Citation87, Citation88 Furthermore, renal transplantation has consistently remained as one of the most common types of solid organ transplantation performed each year in Hong Kong over the past few decades. While HSCT recipients are generally considered to have more severe immunosuppression and thus higher risk of developing invasive fungal infections than solid organ transplantation recipients, they tend to receive more potent and prolonged antifungal prophylaxis and/or empirical antifungal treatment with activities against T. marneffei, such as itraconazole, voriconazole, posaconazole and amphotericin B.Citation89, Citation90, Citation91, Citation92, Citation93 In contrast, fluconazole and nystatin are commonly used as antifungal prophylaxis in patients with solid organ transplantations including renal transplantation, and thus may not be effective against T. marneffei infection.
Hematological malignancies and novel anti-cancer targeted therapies
In addition to a HSCT recipient with IgA myeloma, T. marneffei infection has also been reported in a few adult patients with hematological malignancies or proliferative diseases including non-Hodgkin’s lymphoma, Waldenström’s macroglobulinemia and Langerhans cell histiocytosis.Citation32, Citation42, Citation43, Citation47, Citation48, Citation67, Citation80 The incidence of T. marneffei infection in this group of patients has remained low in the past decades. Recently, however, we were alerted by four unprecedented cases of disseminated T. marneffei infection among hematology patients who received novel targeted therapies including anti-CD20 monoclonal antibodies and kinase inhibitors.Citation25, Citation26
Rituximab and obinutuzumab are types I and II anti-CD20 monoclonal antibodies, respectively, that predominantly target B lymphocytes. In contrast to Th1 response, the role of B-lymphocyte-mediated humoral response in T. marneffei infection is not well-defined. Patients with B-lymphocyte dysfunction may have impaired production of neutralizing antibodies against key virulence factors of T. marneffei identified in genome sequencing, proteome profiling and other downstream studies.Citation94, Citation95, Citation96, Citation97, Citation98, Citation99, Citation100, Citation101, Citation102, Citation103, Citation104, Citation105, Citation106, Citation107, Citation108 Treatment with rituximab induces long-lasting B-lymphocyte-depleting effects. B-lymphocyte reconstitution, characterized by the expansion of functionally immature B lymphocytes and decreased memory B lymphocytes, may take more than one year after treatment completion.Citation109 During this period, latent infections such as hepatitis B or even T. marneffei infection may become reactivated.Citation110 The newer obinutuzumab is even more potent than rituximab in depleting B lymphocytes.Citation111 Therefore, T. marneffei infection should be considered not only in patients who are receiving, but also those who have already completed treatment with anti-CD20 monoclonal antibodies, when they develop compatible clinical features.
Kinase inhibitors such as ruxolitinib and sorafenib have been increasingly used to treat hematological and solid organ malignancies and/or benign conditions such as psoriasis and alopecia acreata in recent years. Ruxolitinib is a selective Janus kinase (JAK) 1 and 2 inhibitor that interferes with the signal transduction for types I and II cytokines including IFN-γ and the JAK-STAT pathway.Citation112 Besides T. marneffei infection, opportunistic infections and reactivation due to other intracellular organisms, including M. tuberculosis, C. neoformans, herpes simplex virus and hepatitis B virus, have also been reported in patients who received treatment with ruxolitinib.Citation113, Citation114, Citation115, Citation116 Sorafenib is a multi-kinase inhibitor that exhibits various immunomodulatory effects, including impairment of T-lymphocyte proliferation, IFN-γ production, natural killer cell activity, dendritic cell function and pro-inflammatory cytokine secretion.Citation117, Citation118, Citation119 The use of sorafenib has been associated with reactivation of latent tuberculosis.Citation120 With the expanding list of targeted therapies becoming available in the market and being used in endemic regions of T. marneffei, it would be important for clinicians to maintain a high index of suspicion and possibly perform serial serological surveillance for T. marneffei infection in patients who have received these agents to avoid a delay in diagnosis and treatment.Citation121
Other non-AIDS conditions
Sporadic cases of T. marneffei infection have been reported in a few other non-HIV-infected patients. Their underlying conditions included idiopathic CD4+ thrombocytopenia, Job’s syndrome, diabetes mellitus, splenectomy and colonic, breast and buccal cancers.Citation32, Citation43, Citation45, Citation49, Citation50, Citation54, Citation62, Citation65, Citation67 However, it is difficult to assess the exact role of these conditions in T. marneffei infection because of the limited number of cases. Interestingly, an increasing number of non-HIV-infected Asian patients with T. marneffei infection who were previously considered to have no underlying comorbidities were subsequently found to be positive for anti-IFN-γ autoantibodies.Citation32 Advances in immunological diagnostics may help to identify more novel immunodeficiency syndromes and their association with T. marneffei infection in the future.
CONCLUDING REMARKS
The epidemiology of T. marneffei infection has changed significantly in the past three decades. It is now widely recognized that the infection is not limited to HIV-infected patients. Looking ahead, more cases of T. marneffei infection are likely to be reported in the future because of several reasons. First, improvement in the healthcare systems of developing countries in Southeast Asia, such as mainland China, Thailand and Vietnam, will likely lead to an enlarging population of non-HIV-infected patients at risk of the infection, including transplantation recipients and cancer patients on targeted therapies. The discovery of novel immunodeficiency syndromes in children and adults will continue to identify more at-risk patient groups. The availability of new diagnostic and typing methods will facilitate the detection and molecular characterization of the T. marneffei strains infecting the patients in these areas.Citation9, Citation121, Citation122, Citation123, Citation124, Citation125, Citation126 Finally, further studies to address key questions regarding the use of prospective surveillance and optimal treatment strategies will become feasible with this continuously expanding population of non-HIV-infected patients with T. marneffei infection.
Fungal infection: increasing outside the HIV population
A fungal infection that rose to prominence in the HIV/AIDS epidemic is becoming increasingly common in non-HIV-infected patients. The life-threatening Talaromyces (Penicillium) marneffei fungus became clinically significant in Southeast Asia with the rise of HIV infection in the 1980s. It is now a declining problem for HIV patients thanks to anti-retroviral drug programs and other HIV control measures. Patrick Woo and co-workers at the University of Hong Kong report, however, in a review article that T. marneffei infections have been increasing in people without HIV infection since the 1990s. The most vulnerable group are those with some deficiency in that part of the immune system known as cell-mediated immunity. The authors recommend that clinicians should become more aware of the changing epidemiology of T. marneffei, and of the importance of early use of antifungal drugs.
This work was partly supported by donations from the Hui Hoy and Chow Sin Lan Charity Fund Limited; the Health and Medical Research Fund (ref. NO 13121342) and HKM-15-M07 (commissioned study) of the Food and Health Bureau of Hong Kong Special Administrative Region Government; the Strategic Research Theme Fund, The University of Hong Kong; and a Croucher Senior Medical Research Fellowship. JFWC has received travel grants from Pfizer Corporation Hong Kong and Astellas Pharma Hong Kong Corporation Limited. JFWC and PCYW were invited speakers Second Asia CARE Forum, which was sponsored by the Gilead Sciences, Inc. The funding sources had no role in study design, data collection, analysis and interpretation, and writing of the report.
Related Research Data
- VanittanakomN,CooperCRJr,FisherMCet al.Penicillium marneffei infection and recent advances in the epidemiology and molecular biology aspects.Clin Microbiol Rev2006; 19:95–110.
- WongSS,SiauH,YuenKY.Penicilliosis marneffei—West meets East.J Med Microbiol1999; 48:973–975.
- HuY,ZhangJ,LiXet al.Penicillium marneffei infection: an emerging disease in mainland China.Mycopathologia2013; 175:57–67.
- CapponiM,SegretainG,SureauP.Penicillosis from Rhizomys sinensis.Bull Soc Pathol Exot Filiales1956; 49:418–421.
- DengZL,YunM,AjelloL.Human penicilliosis marneffei and its relation to the bamboo rat (Rhizomys pruinosus.J Med Vet Mycol1986; 24:383–389.
- ChariyalertsakS,VanittanakomP,NelsonKEet al.Rhizomys sumatrensis and Cannomys badius, new natural animal hosts of Penicillium marneffei.J Med Vet Mycol1996; 34:105–110.
- GugnaniH,FisherMC,Paliwal-JohsiAet al.Role of Cannomys badius as a natural animal host of Penicillium marneffei in India.J Clin Microbiol2004; 42:5070–5075.
- DuongTA.Infection due to Penicillium marneffei, an emerging pathogen: review of 155 reported cases.Clin Infect Dis1996; 23:125–130.
- YuenKY,WongSS,TsangDNet al.Serodiagnosis of Penicillium marneffei infection.Lancet1994; 344:444–445.
- LeePP,ChanKW,LeeTLet al.Penicilliosis in children without HIV infection—are they immunodeficient?Clin Infect Dis2012; 54:e8–e19.
- SegretainG.Penicillium marneffei n.sp., agent of a mycosis of the reticuloendothelial system.Mycopathologia1959; 11:327–353.
- Di SalvoAF,FicklingAM,AjelloL.Infection caused by Penicillium marneffei: description of first natural infection in man.Am J Clin Pathol1973; 60:259–263.
- PautlerKB,PadhyeAA,AjelloL.Imported penicilliosis marneffei in the United States: report of a second human infection.Sabouraudia1984; 22:433–438.
- JayanetraP,NitiyanantP,AjelloLet al.Penicilliosis marneffei in Thailand: report of five human cases.Am J Trop Med Hyg1984; 33:637–644.
- DengZL,ConnorDH.Progressive disseminated penicilliosis caused by Penicillium marneffei. Report of eight cases and differentiation of the causative organism from Histoplasma capsulatum.Am J Clin Pathol1985; 84:323–327.
- ChanJK,TsangDN,WongDK.Penicillium marneffei in bronchoalveolar lavage fluid.Acta cytologica1989; 33:523–526.
- ChanYF,WooKC.Penicillium marneffei osteomyelitis.J Bone Joint Surg Br1990; 72:500–503.
- SoSY,ChauPY,JonesBMet al.A case of invasive penicilliosis in Hong Kong with immunologic evaluation.Am Rev Respir Dis1985; 131:662–665.
- YuenWC,ChanYF,LokeSLet al.Chronic lymphadenopathy caused by Penicillium marneffei: a condition mimicking tuberculous lymphadenopathy.Br J Surg1986; 73:1007–1008.
- LiJS,PanLQ,DengZLet al.[A case report on Penicillium marneffei.].J Clin Dermatol (China)1985; 14:24–26.
- WangIL,YehHP,ChangSCet al.Penicilliosis caused by Penicillium marneffei. A case report.Derm Sin1989; 7:19–22.
- ChanYF,ChowTC.Ultrastructural observations on Penicillium marneffei in natural human infection.Ultrastructur Pathol1990; 14:439–452.
- LeePP,MaoH,YangWet al.Penicillium marneffei infection and impaired IFN-gamma immunity in humans with autosomal-dominant gain-of-phosphorylation STAT1 mutations.J Allergy Clin Immunol2014; 133:894–896.e5.
- TangBS,ChanJF,ChenMet al.Disseminated penicilliosis, recurrent bacteremic nontyphoidal salmonellosis, and burkholderiosis associated with acquired immunodeficiency due to autoantibody against gamma interferon.Clin Vaccine Immunol2010; 17:1132–1138.
- ChanJF,ChanTS,GillHet al.Disseminated infections with Talaromyces marneffei in Non-AIDS patients given monoclonal antibodies against CD20 and kinase inhibitors.Emerg Infect Dis2015; 21:1101–1106.
- TseE,LeungRY,KwongYL.Invasive fungal infections after obinutuzumab monotherapy for refractory chronic lymphocytic leukemia.Ann Hematol2015; 94:165–167.
- SistoF,MiluzioA,LeopardiOet al.Differential cytokine pattern in the spleens and livers of BALB/c mice infected with Penicillium marneffei: protective role of gamma interferon.Infect Immun2003; 71:465–473.
- KudekenN,KawakamiK,KusanoNet al.Cell-mediated immunity in host resistance against infection caused by Penicillium marneffei.J Med Vet Mycol1996; 34:371–378.
- KudekenN,KawakamiK,SaitoA.CD4+ T cell-mediated fatal hyperinflammatory reactions in mice infected with Penicillium marneffei.Clin Exp Immunol1997; 107:468–473.
- KudekenN,KawakamiK,SaitoA.Different susceptibilities of yeasts and conidia of Penicillium marneffei to nitric oxide (NO)-mediated fungicidal activity of murine macrophages.Clin Exp Immunol1998; 112:287–293.
- RongrungruangY,LevitzSM.Interactions of Penicillium marneffei with human leukocytes in vitro.Infect Immun1999; 67:4732–4736.
- KawilaR,ChaiwarithR,SupparatpinyoK.Clinical and laboratory characteristics of penicilliosis marneffei among patients with and without HIV infection in Northern Thailand: a retrospective study.BMC Infect Dis2013; 13:464.
- LouthrenooW,ThamprasertK,SirisanthanaT.Osteoarticular penicilliosis marneffei. A report of eight cases and review of the literature.Br J Rheumatol1994; 33:1145–1150.
- LoCY,ChanDT,YuenKYet al.Penicillium marneffei infection in a patient with SLE.Lupus1995; 4:229–231.
- LamKY,CheungF,YamLYet al.Atypical manifestations in a patient with systemic lupus erythematosus.J Clin Pathol1997; 50:174–176.
- HungCC,HsuehPR,ChenMYet al.Invasive infection caused by Penicillium marneffei: an emerging pathogen in Taiwan.Clin Infect Dis1998; 26:202–203.
- ChimCS,FongCY,MaSKet al.Reactive hemophagocytic syndrome associated with Penicillium marneffei infection.Am J Med1998; 104:196–197.
- KoCI,HungCC,ChenMYet al.Endoscopic diagnosis of intestinal penicilliosis marneffei: report of three cases and review of the literature.Gastrointest Endosc1999; 50:111–114.
- SaadiahS,JeffreyAH,MohamedAL.Penicillium marneffei infection in a non aids patient: first case report from Malaysia.Med J Malaysia1999; 54:264–266.
- PunTS,FangD.A case of Penicillium marneffei osteomyelitis involving the axial skeleton.Hong Kong Med J2000; 6:231–233.
- HsuehPR,TengLJ,HungCCet al.Molecular evidence for strain dissemination of Penicillium marneffei: an emerging pathogen in Taiwan.J Infect Dis2000; 181:1706–1712.
- WongSS,WooPC,YuenKY.Candida tropicalis and Penicillium marneffei mixed fungaemia in a patient with Waldenström's macroglobulinaemia.Eur J Clin Microbiol Infect Dis2001; 20:132–135.
- WongSS,WongKH,HuiWTet al.Differences in clinical and laboratory diagnostic characteristics of penicilliosis marneffei in human immunodeficiency virus (HIV)- and non-HIV-infected patients.J Clin Microbiol2001; 39:4535–4540.
- WangJL,HungCC,ChangSCet al.Disseminated Penicillium marneffei infection in a renal-transplant recipient successfully treated with liposomal amphotericin B.Transplantation2003; 76:1136–1137.
- LiyanX,ChangmingL,XianyiZet al.Fifteen cases of penicilliosis in Guangdong, China.Mycopathologia2004; 158:151–155.
- ChanYH,WongKM,LeeKCet al.Pneumonia and mesenteric lymphadenopathy caused by disseminated Penicillium marneffei infection in a cadaveric renal transplant recipient.Transpl Infect Dis2004; 6:28–32.
- WooPC,LauSK,LauCCet al.Penicillium marneffei fungaemia in an allogeneic bone marrow transplant recipient.Bone Marrow Transplant2005; 35:831–833.
- DeesomchokA,TanprawateS.A 12-case series of Penicillium marneffei pneumonia.J Med Assoc Thai2006; 89:441–447.
- BehCP,GeorgeJ.Disseminated Penicilium marneffei infection.Med J Malaysia2009; 64:86–88.
- MaBH,NgCS,LamRet al.Recurrent hemoptysis with Penicillium marneffei and Stenotrophomonas maltophilia in Job's syndrome.Can Respir J2009; 16:e50–e52.
- ChanJF,Trendell-SmithNJ,ChanJCet al.Reactive and infective dermatoses associated with adult-onset immunodeficiency due to anti-interferon-gamma autoantibody: Sweet's syndrome and beyond.Dermatology2013; 226:157–166.
- LinJN,LinHH,LaiCHet al.Renal transplant recipient infected with Penicillium marneffei.Lancet Infect Dis2010; 10:138.
- LuoDQ,ChenMC,LiuJHet al.Disseminated Penicillium marneffei infection in an SLE patient: a case report and literature review.Mycopathologia2011; 171:191–196.
- ChongYB,TanLP,RobinsonSet al.Penicilliosis in lupus patients presenting with unresolved fever: a report of 2 cases and literature review.Trop Biomed2012; 29:270–276.
- JoostenSA,HannanL,HeroitGet al.Penicillium marneffei presenting as an obstructing endobronchial lesion in an immunocompetent host.Eur Respir J2012; 39:1540–1543.
- HartJ,DyerJR,ClarkBMet al.Travel-related disseminated Penicillium marneffei infection in a renal transplant patient.Transpl Infect Dis2012; 14:434–439.
- LeeWI,HuangJL,WuTSet al.Patients with inhibitory and neutralizing auto-antibodies to interferon-gamma resemble the sporadic adult-onset phenotype of Mendelian Susceptibility to Mycobacterial Disease (MSMD) lacking Bacille Calmette-Guerin (BCG)-induced diseases.Immunobiology2013; 218:762–771.
- QiuY,ZhangJ,LiuGet al.A case of Penicillium marneffei infection involving the main tracheal structure.BMC Infect Dis2014; 14:242.
- De MonteA,RissoK,NormandACet al.Chronic pulmonary penicilliosis due to Penicillium marneffei: late presentation in a french traveler.J Travel Med2014; 21:292–294.
- FurusawaH,MiyazakiY,SonodaSet al.Penicilliosis marneffei complicated with interstitial pneumonia.Intern Med2014; 53:321–323.
- LiuGN,HuangJS,ZhongXNet al.Penicillium marneffei infection within an osteolytic lesion in an HIV-negative patient.Int J Infect Dis2014; 23:1–3.
- XiaXJ,ShenH,XuAE.Cutaneous Penicillium marneffei infection in a patient with idiopathic CD4(+) lymphocytopenia.J Dermatol2015; 42:812–814.
- JiangX,ZhouD.Diagnosis of Penicillium marneffei infection from a blood film.Br J Haematol2015; 171:670.
- YeF,LuoQ,ZhouYet al.Disseminated penicilliosis marneffei in immunocompetent patients: a report of two cases.Indian J Med Microbiol2015; 33:161–165.
- WangPH,WangHC,LiaoCH.Disseminated Penicillium marneffei mimicking paradoxical response and relapse in a non-HIV patient with pulmonary tuberculosis.J Chin Med Assoc2015; 78:258–260.
- StathakisA,LimKP,BoanPet al.Penicillium marneffei infection in a lung transplant recipient.Transpl Infect Dis2015; 17:429–434.
- QiuY,ZhangJ,LiuGet al.Retrospective analysis of 14 cases of disseminated Penicillium marneffei infection with osteolytic lesions.BMC Infect Dis2015; 15:47.
- HoflichC,SabatR,RosseauSet al.Naturally occurring anti-IFN-gamma autoantibody and severe infections with Mycobacterium cheloneae and Burkholderia cocovenenans.Blood2004; 103:673–375.
- DoffingerR,HelbertMR,Barcenas-MoralesGet al.Autoantibodies to interferon-gamma in a patient with selective susceptibility to mycobacterial infection and organ-specific autoimmunity.Clin Infect Dis2004; 38:e10–e14.
- BrowneSK,BurbeloPD,ChetchotisakdPet al.Adult-onset immunodeficiency in Thailand and Taiwan.N Engl J Med2012; 367:725–734.
- ChanJF,YeeKS,TangBSet al.Adult-onset immunodeficiency due to anti-interferon-gamma autoantibody in mainland Chinese.Chin Med J (Engl)2014; 127:1189–1190.
- ChiCY,ChuCC,LiuJPet al.Anti-IFN-gamma autoantibodies in adults with disseminated nontuberculous mycobacterial infections are associated with HLA-DRB1*16:02 and HLA-DQB1*05:02 and the reactivation of latent varicella-zoster virus infection.Blood2013; 121:1357–1366.
- TanakaY,HoriT,ItoKet al.Disseminated Mycobacterium avium complex infection in a patient with autoantibody to interferon-gamma.Intern Med2007; 46:1005–1009.
- KoyaT,TsubataC,KagamuHet al.Anti-interferon-gamma autoantibody in a patient with disseminated Mycobacterium avium complex.J Infect Chemother2009; 15:118–122.
- PatelSY,DingL,BrownMRet al.Anti-IFN-gamma autoantibodies in disseminated nontuberculous mycobacterial infections.J Immunol2005; 175:4769–4776.
- KuCL,LinCH,ChangSWet al.Anti-IFN-γ autoantibodies are strongly associated with HLA-DR*15:02/16:02 and HLA-DQ*05:01/05:02 across Southeast Asia.J Allergy Clin Immunol2015 pii: S0091-6749(15)01356-1.
- KampmannB,HemingwayC,StephensAet al.Acquired predisposition to mycobacterial disease due to autoantibodies to IFN-gamma.J Clin Invest2005; 115:2480–2488.
- BrowneSK,ZamanR,SampaioEPet al.Anti-CD20 (rituximab) therapy for anti-IFN-gamma autoantibody-associated nontuberculous mycobacterial infection.Blood2012; 119:3933–3939.
- CzajaCA,MerkelPA,ChanEDet al.Rituximab as successful adjunct treatment in a patient with disseminated nontuberculous mycobacterial infection due to acquired anti-interferon-gamma autoantibody.Clin Infect Dis2014; 58:e115–e118.
- ZhouF,BiX,ZouXet al.Retrospective analysis of 15 cases of Penicilliosis marneffei in a southern China hospital.Mycopathologia2014; 177:271–279.
- NgWL,ChuCM,WuAKet al.Lymphopenia at presentation is associated with increased risk of infections in patients with systemic lupus erythematosus.QJM2006; 99:37–47.
- Merayo-ChalicoJ,Gomez-MartinD,Pineirua-MenendezAet al.Lymphopenia as risk factor for development of severe infections in patients with systemic lupus erythematosus: a case-control study.QJM2013; 106:451–457.
- WuTC,ChanJW,NgCKet al.Clinical presentations and outcomes of Penicillium marneffei infections: a series from 1994 to 2004.Hong Kong Med J2008; 14:103–109.
- SeoJY,MaYE,LeeJHet al.A case of disseminated Penicillium marneffei infection in a liver transplant recipient.Korean J Lab Med2010; 30:400–405.
- TongMK.Overview of Renal Transplant. Renal Transplantation in Hong Kong.Hong Kong Society of Transplantation: Hong Kong.2006Available at http://www.hkst.org/the-education-corner/49-overview-of-renal-transplant.html/accessed on 8 October 2015.
- LieAK,AuWY,LiangR.Haematopoietic stem cell transplantation in Hong Kong.Hong Kong Med J2009; 15(3 Suppl 3):17–21.
- ChanSC,CheungTT,ChanACet al.New insights after the first 1000 liver transplantations at The University of Hong Kong.Asian J Surg2015pii S1015-9584(15)00065-2.
- WongCF,FungSL,YanSWet al.Lung transplantation in Hong Kong: 12 years of experience.Respirology2008; 13:903–907.
- YuenKY,WooPC,IpMSet al.Stage-specific manifestation of mold infections in bone marrow transplant recipients: risk factors and clinical significance of positive concentrated smears.Clin Infect Dis1997; 25:37–42.
- ChimCS,HoPL,YuenSTet al.Fungal endocarditis in bone marrow transplantation: case report and review of literature.J Infect1998; 37:287–291.
- HoPL,YuenKY.Aspergillosis in bone marrow transplant recipients.Crit Rev Oncol Hematol2000; 34:55–69.
- ChengVC,ChanJF,NganAHet al.Outbreak of intestinal infection due to Rhizopus microsporus.J Clin Microbiol2009; 47:2834–2843.
- WooPC,LeungSY,ToKKet al.Internal transcribed spacer region sequence heterogeneity in Rhizopus microsporus: implications for molecular diagnosis in clinical microbiology laboratories.J Clin Microbiol2010; 48:208–214.
- CaoL,ChanCM,LeeCet al.MP1 encodes an abundant and highly antigenic cell wall mannoprotein in the pathogenic fungus Penicillium marneffei.Infect Immun1998; 66:966–973.
- WongLP,WooPC,WuAYet al.DNA immunization using a secreted cell wall antigen Mp1p is protective against Penicillium marneffei infection.Vaccine2002; 20:2878–2886.
- WooPC,LamCW,TamEWet al.First discovery of two polyketide synthase genes for mitorubrinic acid and mitorubrinol yellow pigment biosynthesis and implications in virulence of Penicillium marneffei.PLoS Negl Trop Dis2012; 6:e1871.
- YuenKY,PascalG,WongSSet al.Exploring the Penicillium marneffei genome.Arch Microbiol2003; 179:339–353.
- YangE,WangG,WooPCet al.Unraveling the molecular basis of temperature-dependent genetic regulation in Penicillium marneffei.Eukaryot Cell2013; 12:1214–1224.
- YangE,ChowWN,WangGet al.Signature gene expression reveals novel clues to the molecular mechanisms of dimorphic transition in Penicillium marneffei.PLoS Genet2014; 10:e1004662.
- WooPC,ZhenH,CaiJJet al.The mitochondrial genome of the thermal dimorphic fungus Penicillium marneffei is more closely related to those of molds than yeasts.FEBS Lett2003; 555:469–477.
- WooPC,TamEW,ChongKTet al.High diversity of polyketide synthase genes and the melanin biosynthesis gene cluster in Penicillium marneffei.FEBS J2010; 277:3750–3758.
- WooPC,LauSK,LiuBet al.Draft genome sequence of Penicillium marneffei strain PM1.Eukaryot Cell2011; 10:1740–1741.
- WooPC,LamCW,TamEWet al.The biosynthetic pathway for a thousand-year-old natural food colorant and citrinin in Penicillium marneffei.Sci Rep2014; 4:6728.
- WooPC,ChongKT,TseHet al.Genomic and experimental evidence for a potential sexual cycle in the pathogenic thermal dimorphic fungus Penicillium marneffei.FEBS Lett2006; 580:3409–3416.
- NimmaneeP,WooPC,VanittanakomPet al.Functional analysis of atfA gene to stress response in pathogenic thermal dimorphic fungus Penicillium marneffei.PLoS One2014; 9:e111200.
- NimmaneeP,WooPC,KummasookAet al.Characterization of sakA gene from pathogenic dimorphic fungus Penicillium marneffei.Int J Med Microbiol2015; 305:65–74.
- LauSK,TseH,ChanJSet al.Proteome profiling of the dimorphic fungus Penicillium marneffei extracellular proteins and identification of glyceraldehyde-3-phosphate dehydrogenase as an important adhesion factor for conidial attachment.FEBS J2013; 280:6613–6626.
- LauSK,ChowWN,WongAYet al.Identification of microRNA-like RNAs in mycelial and yeast phases of the thermal dimorphic fungus Penicillium marneffei.PLoS Negl Trop Dis2013; 7:e2398.
- AnolikJH,FriedbergJW,ZhengBet al.B cell reconstitution after rituximab treatment of lymphoma recapitulates B cell ontogeny.Clin Immunol2007; 122:139–145.
- SetoWK,ChanTS,HwangYYet al.Hepatitis B reactivation in patients with previous hepatitis B virus exposure undergoing rituximab-containing chemotherapy for lymphoma: a prospective study.J Clin Oncol2014; 32:3736–3743.
- van OersMH.CD20 antibodies: type II to tango?Blood2012; 119:5061–5063.
- NaqviK,VerstovsekS,KantarjianHet al.A potential role of ruxolitinib in leukemia.Expert Opin Investig Drugs2011; 20:1159–1166.
- TongLX,JacksonJ,KerstetterJet al.Reactivation of herpes simplex virus infection in a patient undergoing ruxolitinib treatment.J Am Acad2014; 70:e59–e60.
- CaocciG,MurgiaF,PoddaLet al.Reactivation of hepatitis B virus infection following ruxolitinib treatment in a patient with myelofibrosis.Leukemia2014; 28:225–227.
- WyshamNG,SullivanDR,AlladaG.An opportunistic infection associated with ruxolitinib, a novel janus kinase 1,2 inhibitor.Chest2013; 143:1478–1479.
- HopmanRK,LawrenceSJ,OhST.Disseminated tuberculosis associated with ruxolitinib.Leukemia2014; 28:1750–1751.
- HoubenR,VoigtH,NoelkeCet al.MAPK-independent impairment of T-cell responses by the multikinase inhibitor sorafenib.Mol Cancer Ther2009; 8:433–440.
- ZhaoW,GuYH,SongRet al.Sorafenib inhibits activation of human peripheral blood T cells by targeting LCK phosphorylation.Leukemia2008; 22:1226–1233.
- HippMM,HilfN,WalterSet al.Sorafenib, but not sunitinib, affects function of dendritic cells and induction of primary immune responses.Blood2008; 111:5610–5620.
- TeoM,O'ConnorTM,O'ReillySPet al.Sorafenib-induced tuberculosis reactivation.Onkologie2012; 35:514–516.
- WangYF,XuHF,HanZGet al.Serological surveillance for Penicillium marneffei infection in HIV-infected patients during 2004-2011 in Guangzhou, China.Clin Microbiol Infect2015; 21:484–489.
- JanIS,ChungPF,WangJYet al.Cytological diagnosis of Penicillium marneffei infection.J Formos Med Assoc2008; 107:443–447.
- WooPC,LauCC,ChongKTet al.MP1 homologue-based multilocus sequence system for typing the pathogenic fungus Penicillium marneffei: a novel approach using lineage-specific genes.J Clin Microbiol2007; 45:3647–3654.
- WangYF,CaiJP,WangYDet al.Immunoassays based on Penicillium marneffei Mp1p derived from Pichia pastoris expression system for diagnosis of penicilliosis.PLoS One2011; 6:e28796.
- CaoL,ChenDL,LeeCet al.Detection of specific antibodies to an antigenic mannoprotein for diagnosis of Penicillium marneffei penicilliosis.J Clin Microbiol1998; 36:3028–3031.
- YuenKY,WooPC,LauSK.A multilocus sequence typing system for Penicillium marneffei: an international molecular cyber system for tracking its origin and transmission.Hong Kong Med J2010; 16:45–46.