

Abstract
The radiation exposure in the cath lab of patients, cardiologists, and nurses was measured during three consecutive periods of 8 weeks. The first 8 weeks the baseline radiation exposure was obtained. In the second period standard incidences for coronarography and frame rate were changed, without compromising the image quality of the examination. In the third period, a pelvic shield covered the lower part of the patient. This pilot quality project demonstrates that further significant reduction in radiation exposure of 37% is possible for patients. A significant reduction in radiation exposure of 53 and 62% was obtained among cardiologists and nurses working in the cath lab, even with the already diminished radiation exposure over the last years by better equipment and general radioprotection measures.
Medical radiological examinations are the most important source of radiation exposure for the average person in the Western world [Citation1]. It is capital that the cardiologist aims for the best image quality at the lowest achievable radiation dose for the patient. This benefits not only the patient but also the medical operator who performs the radiologic procedure over a period of many years.
Radiation in the cath lab can cause health problems for the patient and for the operator through deterministic and stochastic effects. Radiation can cause direct and indirect injury of the DNA. Changes in the genome increase the risk for cancer [Citation2,Citation3]. It has been documented that radiation causes a 3-fold increase in risk of lens opacities (cataract) in interventional cardiologists, compared to people who are not exposed to medical radiation at work [Citation4]. This risk increases already at low doses.
The protective clothing with lead can cause musculoskeletal problems. Several studies mention the higher risk for psychological problems [Citation5,Citation6].
Vital for radiation reduction is the use of performant and recent cath lab equipment. It is well known that education and sensitisation of the operators and the employees lead to a significant reduction in patient and operator radiation exposure [Citation7].
Over the last years, we invested heavily in the most modern cath lab equipment. The operators and the collaborators both did follow the yearly radiation training in compliance with the Belgian legal requirements.
Can additional sensitisation, education and fine tuning of the radiation protocols still realise a further decrease of patient and operator radiation exposure?
Here, we describe a quality project:
The literature describes a radiation dose reduction up to 90% by the standard radioprotective measures. Most of these are already operative in our cath lab AZ Delta. Is a supplementary education in radioprotective measures for all cath lab operators and employees combined with adaptations in the standard hardware settings effective to give an additional radiation exposure reduction for patients and operators?
Are the current thermoluminescent dosimeters sensitive enough for the detection of a very low radiation exposure? Even a very low radiation exposure frequently received mounts up to a significant lifetime radiation exposure.
Does the use of a protective apron on the patient (‘pelvic shield’) lead to a significant radiation load reduction for the operator? Has this any effect on the patient’s radiation load?
Method
Study population
This pilot project collects the radiation data of 1353 examinations over a period of 24 weeks. The radiation load for the patient is measured by the dose area product (DAP). This is the multiplication of the absorbed dose and the radiated surface. It is expressed in Gray.cm2. It reflects the radiation load for a determined body surface area.
The radiation load data for seven cardiologists (seven male) and 16 nurses (four male and 12 female) are collected over the same period of 24 weeks. These data are expressed in milliSievert (mSv).
Measurements
All DAP radiation measurement is derived from Quaelum Philips (Philips Allura Xper with Clarity software, Philips, Amsterdam, Netherlands). They can be read out directly from the Philips hardware.
The two dosimeters, the one worn under the lead apron (at the height of the left nipple) and the other placed above the lead apron (at the left thyroid level), are both thermoluminescent detectors () delivered by and read out by the Belgian Study Center for Nuclear Energy (SCK-CEN).
Figure 1. The different dosimeters used in this quality project. (A) Thermoluminescent detector delivered by and read out by the Belgian Study Center for Nuclear Energy (SCK-CEN). The dosimeters are collected each month and send to the SCK-CEN. (B) The more sensitive Tracerco dosimeter. The radiation exposure is directly displayed. An audio alarm can be programmed to warn the operator during the examination when exceeding a radiation exposure threshold.
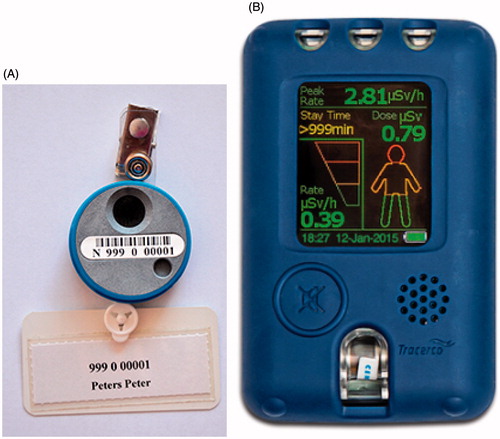
Their minimal detectable dose is 50 µSv. They detect beta, gamma, and X-rays. They have three detectors: one for surface measurement (Hp 0.07), one for more deep measurement (Hp 10), and one for back-up. They measure 4.2 cm in diameter, the thickness is 10 mm and the weight is 15 g. The price is 84.32 Euro per year.
The Tracerco dosimeter (Tracerco, Billingham, UK) () is more sensitive. They can detect radiation exposure below 1 µSv. The radiation exposure can be read out directly on the screen. An audio alarm can be programmed. The operator will be warned by this audio alarm during the procedure when a programmed threshold is exceeded. The price is 730 Euro.
Hardware configuration/timeline
Over the first period of 8 weeks, we measure the real-life radiation exposure for patient and operator in the cath lab. The standard settings for coronarography are: two incidences for the right coronary artery and six incidences for the left coronary artery. Where relevant a left ventricular angiogram is performed, in 1 or 2 incidences. For angioplasty, the number of films/incidences is left at the discretion of the operator.
For scopy three different setting are available on the Philips system. This remains unchanged over the three periods. The cardiologist uses these settings at his own discretion.
For graphy the temporal resolution is 15 frames per second in this first period.
At the end of this first period, two educational lectures of 1 h about general radioprotection points of interest in the cath lab are given to all the first and second cath lab operators. All operators attended at least one of these sessions.
The second period lasts also 8 weeks. Here the standard settings for coronarography are: two incidences for the right coronary artery and four incidences for the left coronary artery. When indicated a left ventricular angiogram is also performed, in 1 or 2 incidences. The operator is free to take more incidences as needed. For angioplasty, the number of films and/or incidences is left at the discretion of the operator.
The scopy mode is standard set at the lowest intensity mode. However, the operator can change this anytime at his own discretion.
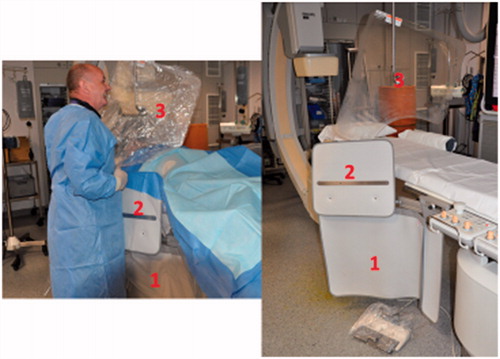
The temporal resolution (graphy) is reduced to 7.5 frames per second. The operator can eventually reset the temporal resolution to 15 frames per second. The operators are motivated to use maximally the radiation protection shields that are fixed to the table and the ceiling (). However, they are asked not to change the use of these shields between period 2 and 3.
Figure 2. Radioprotection shields 1 and 3 are used routinely. Shield 2 is used less frequently, but when used leads to significant radiation dose reduction for the operator (discussion 6).
These settings remain unchanged over the third period of 8 weeks.
During this period, a lead apron (pelvic shield) is placed over the patient: for a radial arterial procedure from the navel to the feet, for a femoral arterial procedure from just beneath the access site in the groin to the feet ().
Figure 3. Lead pelvic shield covers the lower part of the patient.

Data collection
Hence, obtained measurements are thus classified:
Patient measurements:
The DAP radiation measurements are obtained for all patients that underwent a left heart cardiac catheterisation/coronarography (or coronary cineangiography), whether or not followed by angioplasty (or PCI), during the three different periods of 8 weeks.
For period 2 and 3, a dosimeter is positioned at 20 cm above the centre point between the two knees of the patient. This dosimeter measures the radiation load of the patient. In period 3, the dosimeter lies beneath the lead pelvic shield that covers the patient.
Operator measurements:
The dosimeter measurements under the lead apron and above it are registered for the three consecutive periods.
One operator wears an additional Tracerco dosimeter beneath his apron. These measurements are to be compared with these from the thermoluminescent dosimeter worn under the apron (mentioned above, 1(a)) for the three periods.
Statistical analysis
The data are presented as mean ± standard deviations or median and interquartile ranges.
Normality was checked graphically using a histogram and a normal probability plot. If non-normality was detected, a logarithmic transformation was applied.
For group comparisons, parametric test (analysis of variance), non-parametric tests (Kruskal–Wallis test) and post-hoc comparisons with Bonferroni corrections were used. The differences were considered statistically significant when the p value was below .05. Statistical analysis was performed using Stata version 14.1 software (StataCorp LP, College Station, TX).
Results
Examination distribution
The 1353 cath lab examinations are equally distributed between the three periods ().
Table 1. Procedure type. Distribution per period (%).
Radiation exposure of the patient
The average DAP per procedure decreases significantly between period 1 and 2, 3 ( and ). There is a DAP reduction of 37% between period 1 and 2 (significant p value <.01). There is no significant difference between period 2 and 3 (p value 1).
Air Kerma decreases proportionally the same as DAP over the different periods.
There is no significant change in average fluoro time (scopy and graphy) over the three periods. The fear that lower scopy/graphy intensity and frame rate with possible diminished image quality results in longer fluoro times is unfounded ().
The mean radiation exposure measured by the thermoluminescent dosimeter (above the knees) does increase by 9% from period 2 to 3. The effect of a pelvic lead shield over the patient results in a smaller (non-significant) increase in patient radiation exposure than expected from the literature [Citation6] ().
Radiation dose 1st operator/cardiologist
The radiation dose for cardiologists (1st operator) is significantly higher than for nurses (2nd operator) (). Both the radiation measured above and under the lead apron is significantly higher for cardiologists.
The cardiologist radiation dose measured above the apron (unprotected) decreases significantly over the three periods.
There is a nearly significant reduction of 11% for period 2 (p value = .053), and a significant reduction of 53% for period 3 (p value = .008).
The measured radiation dose, compared to the DAP (relative radiation dose), is the highest for period 2 (129%) and the lowest for period 3 (63%).
The cardiologist radiation dose measured under the apron (protected) also decreases significantly over the three consecutive periods (). There is a nearly significant reduction of 20% in period 2 (p value = .053), and a significant reduction of 50% in period 3 (p value = .008).
The relative radiation dose is also highest in period 2 (116%) and lowest in period 3 (66%).
There is a clear difference between the measurement of the Tracerco dosimeter and of the thermoluminescent dosimeter, both worn under the apron (). The Tracerco dosimeter is much more sensitive than the thermoluminescent dosimeter.
The daily worn thermoluminescent dosimeter measures a radiation dose of 0 mSv for the three periods. For the Tracerco dosimeter, the measured dose for the three periods are: 121, 62.4, and 40 µSv. This gives a yearly radiation dose of, respectively, 0.786, 0.405, and 0.260 mSv. Though these doses are very low, they are not negligible, and are not measured by the normally worn thermoluminescent dosimeter.
Table 2. DAP, fluoroscopy time, and Air Kerma per period.
Table 3. Patient radiation exposure, measured by DAP and by dosimeter at knee level.
Table 4. Comparison radiation exposure 1st vs. 2nd operator.
Table 5. Cardiologist radiation exposure.
Table 6. Comparison thermoluminescent dosimeter and Tracerco dosimeter, both worn under the apron.
Radiation dose 2nd operator/nurse
The results are similar to these from the 1st operator. The radiation dose measured above the apron decreases significantly over the three consecutive periods. There is a measured reduction of 29% for period 2 (p value .11) and of 62% for period 3 (p value .017).
The relative radiation dose for the operator is similar for period 1 and 2, and lowest for period 3.
The radiation dose measured under the apron is barely measurable over the three periods, respectively, 0.00467, 0.00667, and 0.00333 mSv. The measured differences are non-significant.
Discussion
This pilot quality study demonstrates that a further significant reduction in radiation exposure dose is possible for cardiologists and nurses working in the cath lab even with the modern equipment and the standard radioprotective rules:
Educational lectures for sensitisation of all operators, combined with structural measures, leads to a significant reduction in radiation dose of 37% for the patient.
This goes together with a reduction in radiation exposure at the unprotected area of the body for both the first and the second operator of, respectively, 11 and 29%.
For the first operator/cardiologist, the radiation exposure is reduced by 20% at the protected body surface area. The measured radiation exposure for the second operator is here negligible.
The fear that structural measurements as frame rate and radiation intensity would lead to a longer fluoro time could not be demonstrated.
Between period 2 and 3, a pelvic shield covered the lower part of the patient. This leads to a small non-significant dose augmentation for the patient. This augmentation was lower than described in the study of Prof Anees Musallam [Citation7]. This can be due by the 19% of the procedures being performed with a femoral access puncture site (with less covering of the pelvic shield). As the dosimeter was placed on the backside of the patient, the increased reading in period 3 cannot be attributed to fluorescent radiation from the lead shield (a local condition).
However, the dose reduction for the first and second operator by the pelvic shield is spectacular: for the non-protected body surface area, there is a dose reduction of 53% for the cardiologist and of 62% for the nurse. This reduction is, respectively, 50 and 29% at the protected body surface areas.
The pelvic shield gives the most radiation reduction for the operators. The structural measures reduce the radiation load from 100 to 80–89%. In the third period, the pelvic shield gives a reduction from 80–89 to 47–50% for, respectively, unprotected and protected body surface area.
As the use of the protective shields does not change for each individual cardiologist between period 2 and 3, the reduction in radiation exposure between these two periods can only be explained by the use of the pelvic shield.
The currently used thermoluminescent dosimeter, as worn under the apron, underestimates the yearly received radiation dose for the operators. For the first operator zero mSv was reported, while a significant radiation load was measured by the Tracerco dosimeter.
The relative radiation dose (the measured radiation dose by the dosimeter divided by the cumulative DAP over the same period) is highest in period 2, and lowest in period 3. Probably, the scatter radiation does not decrease linearly with a reduction in radiation intensity. Lower intensity can lead to relatively more scatter for the operator. However, the scatter is very efficiently blocked by the pelvic shield in period 3.
The measured radiation dose is very different between the cardiologists. The unprotected dosimeter during period 1 measures a dose of 3.31 mSv for one cardiologist and 0.55 mSv for another, with a calculated yearly load of 20 mSv for the first, and of 6.5 mSv for the second. The cumulative DAP and the fluoro time during the first period were similar for both cardiologists. This can be explained by the use of the lead protection shield that is fixed to the table and can be folded up at the right side of the patient at the beginning of the procedure (shield nr 2, ). Each cardiologist uses the lead protection shield fixed to the cath lab table (shield nr 1, ), and to the ceiling (shield nr 3, ).
During the third period, this difference decreased. The radiation dose for the first cardiologist was 0.87 mSv (yearly dose 5.2 mSv), and for the second cardiologist 0.41 mSv (yearly dose 2.4 mSv). The cardiologists that started in period 1 with the highest radiation dose achieved the most pronounced dose reductions in period 3.
Disclosure statement
No potential conflict of interest was reported by the authors.
We thank Mrs Christine Bazelmans for the statistical analysis of our results and we thank Mrs Sofie Cremmery (cath lab nurse) for supervising this project on the work floor.
References
- Picano E. Sustainability of medical imaging. BMJ. 2004;328:578–580.
- BELCOLORE Continual education session. Study Centre for Nuclear Energy SCK-CEN, België. Brussels (Belgium): University Hospital Brussels; 2016.
- Rajaraman P, Doody MM, Yu CL. Cancer risks in US radiologic technologists working with fluoroscopically guided interventional procedures, 1994–2008. AJR Am J Roentgenol. 2016;206:1101–1109.
- Elmaraezy A, Morra MA, Mohammed AT. Risk of cataract among interventional cardiologists and catheterization lab staff: a systematic review and meta-analysis. Catheter Cardiovasc Intv. 2017;90:1–9.
- Andreassi MG. Occupational health risks in cardiac catheterization laboratory workers. Circ Cardiovasc Interv. 2016;9:e003273.
- Vano E, Gonzalez L, Guibelalde E. Radiation exposure to medical staff in interventional and cardiac radiology. Catheter Cardiovasc Interv. 2015;85:1164–1170.
- Anees M, Ina V.Svetlana Dadaev A randomized study comparing the use of a pelvic lead shield during trans-radial interventions: threefold decrease in radiation to the operator but double exposure to the patient. Catheter Cardiovasc Interv. 2015;85:1164–1170.

