

Abstract
Background
Elevated pulmonary artery pressure (PAP) in patients with severe aortic stenosis (AS) is a strong predictor of adverse prognosis. This study sought to assess the relation between PAP and clinical and echocardiographic parameters in elderly patients with severe AS, as well as to identify the determinants of the change in PAP after transcatheter aortic valve implantation (TAVI).
Methods
The study included 170 subjects (age 81 ± 7 years, 45% men) with symptomatic severe AS who were treated by TAVI. They underwent a clinical evaluation and a transthoracic echocardiography before the TAVI procedure and 6 months after.
Results
In a multivariable analysis, the independent predictors for baseline PAP were the body mass index (BMI) (β = 0.21, p = .006), COPD GOLD class (β = 0.20; p = .009), the E/e′ ratio (β = 0.20; p = .02) and the degree of aortic regurgitation (β = 0.20; p = .01). After TAVI, there was significantly less (51% vs. 29%, p<.0001) pulmonary hypertension, defined as a tricuspid regurgitation velocity ≥2.8 m/s. The baseline variables related to an improvement in PAP were the tricuspid regurgitation velocity (p = .0001) and the E/e′ (p = .005). From the parameters potentially modified with TAVI, the only independent predictor of PAP variation was the change in the E/e′ ratio (β = 0.23; p = .01).
Conclusions
Independent predictors for baseline PAP in elderly patients with symptomatic AS were the BMI, GOLD class, the aortic regurgitation and the E/e′ ratio. The baseline predictors for a change in PAP 6 months after TAVI were the baseline PAP and E/e′, with only the change in the E/e′ ratio being correlated to the change in PAP.
Introduction
Aortic stenosis (AS) is the most common valvular heart disease in the Western world and its prevalence is expected to increase due to the aging of the population [Citation1]. The rise in pulmonary artery pressure (PAP) in these patients has been clearly demonstrated as a strong predictor of worse prognosis after medical, surgical or interventional management [Citation2–4]. We also know from several studies that PAP improves after relieving the valvular obstacle [Citation5–7]. There is however little data concerning the determinants of this rise in PAP and in particular on the factors associated with post interventional improvement in PAP [Citation8–12]. This study sought to assess the relation between PAP and clinical and echocardiographic parameters in patients with severe AS, as well as to identify the determinants of improvement in PAP after transcatheter aortic valve implantation (TAVI).
Methods
The study design was monocentric and retrospective, involving patients treated by TAVI for severe AS between 2005 and 2014 in our institution. The study was conducted according to the principles of the Declaration of Helsinki. Retrospective clinical studies are waived for approval by our Institutional Ethical Committee. All patients have given written consent for the use of their anonymised data in this research.
Patient population
After exclusion of patients with prior aortic or mitral valvular surgery, mitral stenosis or significant areas of focal LV akinesia (defined as an akinetic region extending to at least three segments, involving the basal septum and/or the basal lateral wall), the study included 170 subjects (mean age 81 ± 78 years, 45% men) with symptomatic severe AS, defined as an aortic valve area less than 1 cm2 and/or less than 0.6 cm2/m2 and/or a mean pressure gradient over 40 mmHg, who were treated by TAVI. All patients underwent a clinical evaluation and a transthoracic echocardiography at baseline before the TAVI procedure and at 6 months post-TAVI.
Venous blood samples were drawn from each patient within 30 min of the Doppler echocardiography study after 30 min of supine rest. For NT-proBNP determination, an electrochemiluminescence immunoassay (ProBNP Elecsys, Roche Diagnostics GmbH, Mannheim, Germany) was used. Due to the very large range of values of the natriuretic peptide and the abnormal distribution of this variable, the log10 of the NT proBNP was used in the analysis.
Transthoracic echocardiography
Two-dimensional echocardiography was performed using a Philips iE33 system (Philips, Best, The Netherlands) with the patient in the left lateral decubitus position. Echocardiographic studies were performed by an independent experienced echocardiographer, blinded to the patient’s clinical status. All echocardiograms were saved as video loops or still frames in a digital database and were reanalysed by an experienced cardiologist (MS). LV ejection fraction was calculated using the biplane modified Simpson rule. The mitral inflow velocity profile (E/A wave ratio, E wave deceleration time) was assessed with pulsed-wave Doppler. The early diastolic velocities at the septal annulus level were assessed with pulse-wave tissue Doppler from a standard apical four-chamber view [Citation13]. Pulmonary artery pressure was estimated from the trans-tricuspid systolic gradient. Tricuspid annular systolic excursion (TAPSE) was measured in standard apical four-chamber view.
Each echocardiographic measurement was performed by at least two different observers: one initial by the sonographer performing the study, validated by a supervising imaging cardiologist; and a second measurement performed by MS (highly experienced imaging cardiologist), who was blinded to the clinical status of the subjects during these measurements. In case of disagreement between the two observers, a highly experienced imaging cardiologist (MG) acted as third observer and adjusted the result.
Definitions
Obesity was defined as a body mass index (BMI) above 30 kg/m2 [Citation14]. COPD was classified according to GOLD class [Citation15]. Severe impairment of the renal function was defined as GFR less than 30 ml/min/1.73 m2, present for more than 3 months, as estimated by the 2009 CKD-EPI creatinine equation [Citation16]. Aortic and mitral regurgitations were assessed semiquantitatively according to current guidelines for the evaluation of native valves [Citation17]. Pulmonary hypertension (PHT) was considered at a value of the trans-tricuspid systolic gradient above 2.8 m/s [Citation18]. Significant coronary artery disease was defined as >50% stenosis in at least one coronary artery.
Statistical analysis
Continuous variables are presented as means (±SD) if normally distributed. Categorical variables are presented as frequencies and percentages. Differences between continuous variables were assessed by the paired-samples t test and between categorical variables by chi-square test. Univariate linear regression was used to identify the factors related to PAP level. The factors found to be significant in univariate analysis or considered relevant based on clinical data were entered into a multivariable linear regression model. The overall performance of the regression model was assessed using R2 statistics. Collinearity diagnostics and Durbin–Watson’s statistics were used to check the assumptions of no multicollinearity and serial independence of errors. A two-sided p value less than .05 was used for declaring statistical significance. All statistical analyses were performed with SPSS 21.0 software (SPSS Inc, Chicago, IL).
Results
The baseline characteristics of the population are shown in . All patients were symptomatic. Ten patients (6%) were in NYHA class I, 53 patients (31%) were in NYHA class II and 102 patients (60%) were in NYHA class III or IV (in five patients NYHA class could not be determined due to immobility). Forty-six patients (27%) had angina and 15 (9%) syncope. Significant COPD (class 2–4) was present in 49 patients (29%), obesity in 32 (18%), severe renal dysfunction in 19 (11%). Ninety-two of these patients (54%) had coronary artery disease, in 38 (22%) already treated by coronary bypass surgery and in 38 (22%) by a percutaneous intervention. In addition, a percutaneous intervention was performed along with the TAVI intervention in 19 (11%) patients. PHT was present in 86 patients (51%). A pacemaker was already present before the TAVI procedure in 15 (9%) and a complete left bundle branch block (LBBB) was diagnosed at baseline in 29 (17%).
Table 1. Baseline characteristics of the study patients.
Determinants of PHT at baseline
In univariate analysis, COPD class, mitral and aortic insufficiency, ejection fraction and E/e′ ratio (, ) were related to baseline PAP. In a multivariable analysis, the independent predictors for PHT were BMI (Beta = 0.21; p = .006), COPD GOLD class (Beta = 0.20; p = .009), aortic regurgitation (Beta = 0.20; p = .01) and the E/e′ ratio (Beta = 0.20; p = .02).
Figure 1. Correlation plot between baseline values of the E/e′ ratio and the value of the pulmonary artery pressure as derived from the maximal transtricuspid gradient. A correlation line was fitted to the data (central thick line), as well as 95% confidence intervals (thin lateral lines).
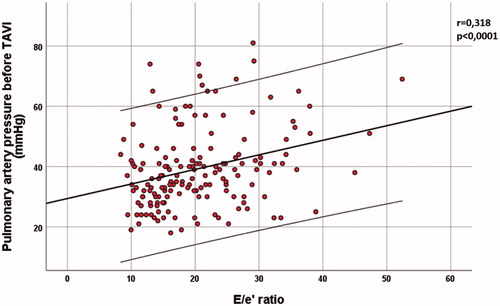
Table 2. Baseline determinants of PHT.
Baseline predictors of improvement in pulmonary artery pressure
Before TAVI, 86 patients (51%) had PHT (). After TAVI an improvement in PAP, defined as a decrease in trans-tricuspid systolic gradient as compared to the baseline value, was noted in 101 patients (59%). No improvement or increased gradient was noted in 69 (41%). After TAVI, the number of PHT patients was significantly lower (50; p<.0001) and 36 (21%) PHT patients normalised the PAP.
Table 3. Comparison between no improvement or worsening PAP vs. improved PAP.
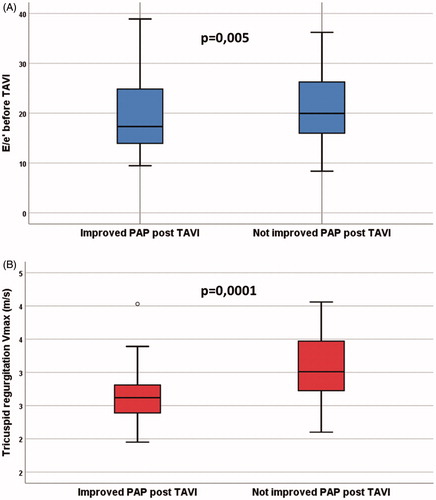
When comparing the baseline parameters in the group with improved trans-tricuspid gradient versus the group without improvement, the only significantly different variables are the baseline value of the trans-tricuspid gradient and the E/e′ ratio ().
Figure 2. Comparison between the groups of patients who improved their transtricuspid gradient 6 months after TAVI implantation (left boxplots) and the ones who did not improve or increased their gradient (right boxplots). The only significantly different parameters measured at baseline (before TAVI) according to our analysis were the E/e′ ratio (A) and maximal velocity of the tricuspid regurgitation (B). The higher E/e′ ratio and higher transtricuspid gradient probably reflect a more advanced state of disease in the patients who did not show improvement in pulmonary artery pressure after TAVI.
Variation of clinical and echographic parameters 6 months after TAVI
There was a significant decrease in NYHA class, mean transaortic gradient, as well as in tricuspid regurgitation velocity (). We noted a significant decrease in Log10NT-proBNP from 2.3 ± 0.6 at baseline to 2.1 ± 0.5 six months after TAVI (p = .002). There was no significant change in the mean degree of mitral and aortic regurgitation. The E and A wave velocity increased significantly, without improvement of mean ejection fraction or E/e′ ratio.
Table 4. Variation of clinical and echocardiographic variables after TAVI.
A new-onset (not present at baseline) LBBB was noticed in 67 (39%) patients. Implantation of a new pacemaker (not present at baseline) was indicated in 46 patients (27%).
Right ventricular function parameters in the whole group did not change significantly (baseline TAPSE = 20.03 ± 5.4 mm; six months after TAVI the average TAPSE = 20.12 ± 5.2 mm; p = .73).
Parameter variation as determinants of a change in PAP 6 months after TAVI
In univariate and multivariate analyses, only the change in E/e′ ratio was a predictor of a change in PAP (, ).
Figure 3. Correlation plot between the variation of the E/e′ ratio before and after the TAVI procedure (delta E/e′) and the variation of the pulmonary artery pressure (delta PAP) as derived from the maximal transtricuspid gradient. A correlation line was fitted to the data (central thick line), as well as 95% confidence intervals (thin lateral lines).
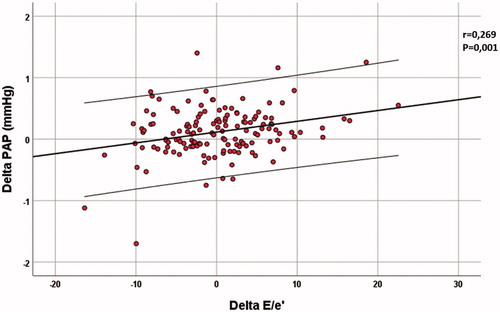
Table 5. Parameter variation as determinants of pulmonary artery pressure change 6 months after TAVI.
Discussion
The main findings of this study in patients with severe AS treated with TAVI were: (1) the independent determinants of the baseline value of the PAP were BMI, the GOLD classification of COPD, aortic regurgitation and E/e′ ratio, (2) there was a significant improvement in PAP 6 months after TAVI, with significantly less patients having PHT, (3) the baseline parameters predicting an improvement in PAP were the tricuspid regurgitation velocity and the E/e′ ratio, and (4) the change in E/e′ ratio was the only predictor of a change in PAP.
PHT is noted in 28–56% of the patients with AS, depending on the definition threshold [Citation3,Citation4,Citation7,Citation9] and clinical characteristics. Elderly persons with severe AS undergoing TAVI may have several comorbidities, especially COPD, leading to a significant increase in PAP that is relatively unrelated to AS. They may also have concomitant regurgitant lesions of the left heart valves that contribute to an increase in PAP. In our study, PHT was present in 51% of patients. Several factors were shown to be related to a rise in PAP in univariate analysis: the GOLD classification of COPD, mitral or aortic regurgitation, E/e′ ratio, and ejection fraction. Surprisingly, the trans-aortic gradient did not reach statistical significance. Moreover, the multivariable model including these parameters yielded only four independent predictors for PHT: COPD severity, filling pressures of the left ventricle, reflected by the E/e′ ratio, BMI and aortic insufficiency. This is in concordance with data already present in the literature, showing that diastolic function of the left ventricle is the main predictor of elevated PAP in severe AS [Citation12]. The role of COPD severity is obvious, especially in this elderly population in whom chronic pulmonary disease is not rare. The fact that BMI was not significant in the univariate analysis, but very significant in the multivariate cannot be explained by our statistical model, but the result is consistent with previous findings [Citation19]. It could be due to the influence of the BMI on the prevalence of hypertension, diabetes and coronary artery disease (factors that were not entered in the multivariable analysis due to their lack of impact in the univariate model). Numerous publications address the prognostic role of the postprocedural paravalvular leak [Citation20], but there is very little recent data on the impact of pre-procedural native valve aortic insufficiency associated to AS [Citation21].
In our study, there was an overall statistically significant improvement in PAP, but only 59% really improved, and only 21% normalised the PAP. The value of the PAP was unchanged or even worsened in 41%. This may explain the little overall variation of the mean PAP. There was also a significant improvement in transaortic gradient without significant changes in the ejection fraction and the overall degree of mitral and aortic insufficiency. The effect of TAVI on the ejection fraction has indeed been reported as either neutral or positive [Citation22–24]. In a recent meta-analysis, a non-significant trend towards a reduction in mitral regurgitation was reported [Citation25], consistent with our findings. The change in aortic regurgitation is of course, very variable, depending on the baseline characteristics of each patient as well as numerous technical factors [Citation26].
It has already been noted that PAP improves after successful TAVI intervention (according to VARC 2 criteria [Citation20]). This is most likely due to the removal of the valvular obstacle and the possible improvement in left ventricular systolic and diastolic function or valvular regurgitation. The persistence of PHT is considered to impact long-term prognosis in patients with severe AS [Citation11]. The improvement in PAP was related to the initial value of the PAP and the E/e′ ratio. Very few studies investigated this particular matter, and only in the setting of surgical valvular replacement, but the results are similar [Citation5,Citation27]. Higher values of PAP and E/e′ may suggest a more advanced disease in which the beneficial effects after TAVI may be less important. The only independent dynamic variable predicting a change in PAP after TAVI proved to be the change in the E/e′ ratio.
The general clinical improvement, demonstrated by a significant decrease of the NYHA class, was reflected in echocardiography by a decrease in tricuspid regurgitation peak velocity and mean transaortic gradient (). This improvement was correlated with a similar evolution of the biomarkers of elevated intracardiac pressure, as observed in heart failure in general [Citation28] and in elderly patients with AS [Citation13].
After TAVI, the mitral inflow E and A waves had significantly higher amplitudes, but the E/e′ ratio did not change considerably. The E/e′ ratio has a paradoxical evolution: although it was a significant determinant of the baseline PAP and of the improvement in PAP, its mean value did not change significantly. There could be several explanations to the paradoxical behaviour of this parameter, that does not change in spite of the significant change in PAP. One explanation may reside in an early and sustained increase in cardiac output after relieving the aortic obstacle (as reflected by the rise in E and A velocities through an unchanged mitral valve). Also, improvement of the septal e′ velocity could be limited in the presence of a prosthetic valve very close to the mitral septal point. However, the role of the diastolic function as measured by the E/e′ ratio is reinforced by the fact that the other main potential factors influencing the PAP (left heart valvular regurgitation, LV ejection fraction, severity of the pulmonary disease and right ventricular function) did not show any significant correlations in this study.
The debate on the optimal site of e′ measurement is still going on but the septal site seems to correlate best to direct and indirect measurements of LV filling pressures [Citation13,Citation29,Citation30].
A new-onset LBBB or the implantation of a new pacemaker did not demonstrate a significant effect on the PAP in our patients, in univariate and multivariate analysis.
Clinical implications
PAP evaluation by echocardiography needs to be a part of the prognostic estimation of potential TAVI candidates [Citation20, Citation31], along with the filling pressures of the left ventricle, the two elements being interconnected. COPD and obesity remain clinical features to be considered when estimating the role of AS in the rise of PAP. The improvement in the filling pressures of the left ventricle after relieving the valvular obstacle, although insignificant on the population level, seems to be the main factor contributing to the reduction in PAP.
Study limitations
This is a retrospective cross-sectional study, but the quality of the data was not compromised because data acquisition has been done according to a very strict prospectively defined TAVI protocol. The limited number of patients is also a potential problem in interpreting statistical models, especially when the number of variables is important. However, the level of statistical significance was sufficient to sustain our conclusions. The evaluation of PAP by echocardiography has several known limitations [Citation32,Citation33] but was preferred due to its lack of risk for the patient, as compared to invasive measurements. Finally, in AS patients, the evaluation of the aortic regurgitation is already difficult [Citation17]. Estimating its change can be even more so, since it is a comparison of valvular regurgitation with a paraprosthetic leak.
Conclusions
Independent predictors for baseline PAP in elderly patients with symptomatic AS were the BMI, GOLD class and left ventricular filling pressure reflected by the E/e′ ratio. The baseline variables related to a change in PAP 6 months after TAVI were the baseline PAP and E/e′, with only the change in the E/e′ ratio being correlated to the change in PAP.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24(13):1231–1243.
- Cam A, Goel SS, Agarwal S, et al. Prognostic implications of pulmonary hypertension in patients with severe aortic stenosis. J Thorac Cardiovasc Surg. 2011;142(4):800–808.
- Zlotnick DM, Ouellette ML, Malenka DJ, et al. Effect of preoperative pulmonary hypertension on outcomes in patients with severe aortic stenosis following surgical aortic valve replacement. Am J Cardiol. 2013;112(10):1635–1640.
- Luçon A, Oger E, Bedossa M, et al. Prognostic implications of pulmonary hypertension in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation: study from the FRANCE 2 registry. Circ Cardiovasc Interv. 2014;7(2):240–247.
- Tracy GP, Proctor MS, Hizny CS. Reversibility of pulmonary artery hypertension in aortic stenosis after aortic valve replacement. Ann Thorac Surg. 1990;50(1):89–93.
- Schewel D, Schewel J, Martin J, et al. Impact of transcatheter aortic valve implantation (TAVI) on pulmonary hyper-tension and clinical outcome in patients with severe aortic valvular stenosis. Clin Res Cardiol. 2015;104(2):164–174.
- Ben-Dor I, Goldstein SA, Pichard AD, et al. Clinical profile, prognostic implication, and response to treatment of pulmonary hypertension in patients with severe aortic stenosis. Am J Cardiol. 2011;107(7):1046–1051.
- Aragam JR, Folland ED, Lapsley D, et al. Cause and impact of pulmonary hypertension in isolated aortic stenosis on operative mortality for aortic valve replacement in men. Am J Cardiol. 1992;69(16):1365–1367.
- Faggiano P, Antonini-Canterin F, Ribichini F, et al. Pulmonary artery hypertension in adult patients with symptomatic valvular aortic stenosis. Am J Cardiol. 2000;85(2):204–208.
- Ahn HS, Chang SA, Kim HK, et al. Determinants of pulmonary hypertension development in moderate or severe aortic stenosis. Int J Cardiovasc Imaging. 2014;30(8):1519–1528.
- D'Ascenzo F, Conrotto F, Salizzoni S, et al. Incidence, predictors, and impact on prognosis of systolic pulmonary artery pressure and its improvement after transcatheter aortic valve implantation: a multicenter registry. J Invasive Cardiol. 2015;27(2):114–119.
- Casaclang-Verzosa G, Nkomo VT, Sarano ME, et al. E/Ea is the major determinant of pulmonary artery pressure in moderate to severe aortic stenosis. J Am Soc Echocardiogr. 2008;21(7):824–827.
- Strachinaru M, van Dalen BM, Van Mieghem N, et al. Relation between E/e′ ratio and NT-proBNP levels in elderly patients with symptomatic severe aortic stenosis. Cardiovasc Ultrasound. 2015;13(1):29.
- WHO. Obesity: preventing and managing the global epidemic. Report of a WHO Consultation. WHO Technical Report Series 894. Geneva: World Health Organization; 2000.
- GOLD. Global Strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2019. Available from: http://www.goldcopd.org/
- Levin A, Stevens PE. Summary of KDIGO 2012 CKD Guideline: behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014;85(1):49–61.
- Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33(19):2451–2496.
- Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685–713.
- Weyman AE, Davidoff R, Gardin J, et al. Echocardiographic evaluation of pulmonary artery pressure with clinical correlates in predominantly obese adults. J Am Soc Echocardiogr. 2002;15(5):454–462.
- Kappetein AP, Head SJ, Généreux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 Consensus Document. J Am Coll Cardiol. 2012;60(15):1438–1454.
- Honda S, Kitai T, Okada Y, et al. Impact of aortic regurgitation on the prognosis of severe aortic stenosis. Heart. 2012;98(21):1591–1594.
- Kamperidis V, Joyce E, Debonnaire P, et al. Left ventricular functional recovery and remodeling in low-flow low-gradient severe aortic stenosis after transcatheter aortic valve implantation. J Am Soc Echocardiogr. 2014;27(8):817–825.
- Kempny A, Diller GP, Kaleschke G, et al. Longitudinal left ventricular 2D strain is superior to ejection fraction in predicting myocardial recovery and symptomatic improvement after aortic valve implantation. Int J Cardiol. 2013;167(5):2239–2243.
- D'Andrea A, Padalino R, Cocchia R, et al. Effects of transcatheter aortic valve implantation on left ventricular and left atrial morphology and function. Echocardiography. 2015;32(6):928–936.
- Sannino A, Losi MA, Schiattarella GG, et al. Meta-analysis of mortality outcomes and mitral regurgitation evolution in 4,839 patients having transcatheter aortic valve implantation for severe aortic stenosis. Am J Cardiol. 2014;114(6):875–882.
- O'Sullivan KE, Gough A, Segurado R, et al. Is valve choice a significant determinant of paravalvular leak post-transcatheter aortic valve implantation? A systematic review and meta-analysis. Eur J Cardiothorac Surg. 2014;45(5):826–833.
- Tassan-Mangina S, Metz D, Nazeyllas P, et al. Factors determining early improvement in mitral regurgitation after aortic valve replacement for aortic valve stenosis: a transthoracic and transesophageal prospective study. Clin Cardiol. 2003;26(3):127–131.
- Klimczak-Tomaniak D, van den Berg VJ, Strachinaru M, et al. Longitudinal patterns of NT-proBNP, troponin T and CRP in relation to the dynamics of echocardiographic parameters in heart failure patients. Eur Heart J Cardiovasc Imaging. 2019. DOI:10.1093/ehjci/jez242
- Srivastava PM, Burrell LM, Calafiore P. Lateral vs medial mitral annular tissue Doppler in the echocardiographic assessment of diastolic function and filling pressures: which should we use? Eur J Echocardiogr. 2005;6(2):97–106.
- Nagueh SF, Middleton KJ, Kopelen HA, et al. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30(6):1527–1533.
- Barbash IM, Escarcega RO, Minha S, et al. Prevalence and impact of pulmonary hypertension on patients with aortic stenosis who underwent transcatheter aortic valve replacement. Am J Cardiol. 2015;115(10):1435–1442.
- Firstenberg MS, Levine BD, Garcia MJ, et al. Relationship of echocardiographic indices to pulmonary capillary wedge pressures in healthy volunteers. J Am Coll Cardiol. 2000;36(5):1664–1669.
- Naeije R, D'Alto M, Forfia PR. Clinical and research measurement techniques of the pulmonary circulation: the present and the future. Prog Cardiovasc Dis. 2015;57(5):463–472.

