

Abstract
In heart failure, fluid overload is a major pathological mechanism leading to vascular congestion, pulmonary congestion and elevated jugular venous pressures. Diuretics play a significant role in the management of patients with congestive heart failure. It is used to relieve the congestive symptoms of heart failure. However, the appropriate use of diuretics remains challenging due to various complications like electrolyte abnormalities, worsening renal function and diuretic resistance. This has prompted towards the search of safer and effective alternatives. This review evaluates the use of diuretics in congestive heart failure and discusses the complications of different types of diuretics, which is essential for successful management of congestion in patients with heart failure and hence to optimise the outcome for the patients.
Introduction
According to the American Heart Association/American College of Cardiology guidelines (AHA/ACCF), heart failure (HF) can be defined as ‘a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ventricle to fill or eject blood’ [Citation1,Citation2]. Heart failure can be categorised into heart failure with reduced ejection fraction (HFrEF) defined by an ejection fraction ≤40% and heart failure with preserved ejection fraction (HFpEF) defined by an ejection fraction ≥50% [Citation3]. The prevalence of heart failure in the USA is over 5 million cases with a further 23 million cases worldwide [Citation4,Citation5]. HF is the most common cause for hospitalisation in patients over the age of 65 years old [Citation6]. HF is a significant public health issue reflected by the large burden it poses to the economy, costing $31 billion each year with a projected increase to $70 billion by 2030 [Citation7].
A failing heart that is unable to perfuse the kidneys appropriately causes a significant increase in the activation of renin angiotensin aldosterone system, ultimately leading to retention of sodium and water, resulting in fluid overload. This is compounded by arginine vasopressin (AVP) release, enhancing water retention and also increasing thirst [Citation8]. The congestion produced is responsible for a significant amount of symptoms associated with heart failure such as shortness of breath due to pulmonary oedema and pleural effusions [Citation9]. Furthermore, elevation of central venous pressure due to fluid overload is associated with renal dysfunction, hepatic dysfunction and upregulation of inflammatory cytokines, and a poor prognosis in advanced decompensated heart failure [Citation10–12].
Since mid-1990, the survival rates of those with HF have increased, leading to an increased prevalence of the disease. Our ability to increase survival time in those with HF can be partially attributed to a better and more appropriate use of pharmacological interventions [Citation13]. These interventions also include the utilisation of diuretics such as spironolactone or eplerenone which have been found to reduce all-cause mortality, sudden death and hospitalisations in HF patients with impaired left ventricular dysfunction [Citation14]. The influence of diuretics on the pathophysiology of heart failure as a chronic disease process is associated with the resulting fluid losses. Diuretic therapy decreases fluid volume of the intra-vascular space, allowing the mobilisation of oedema from the extravascular space. The primary mechanism underlying the action of diuretics is the creation of an environment of negative sodium (Na+) balance through increased Na + secretion. This is achieved by loop diuretics through inhibition of the sodium-potassium-chloride (Na+/K+/2Cl-) carrier, thiazide diuretics by inhibiting the Na+/Cl- cotransporter, and finally by potassium sparing diuretics, such as spironolactone, that act on the distal and collecting tubules by inhibiting Na + reabsorption along with K + and H + secretion [Citation15].
While diuretic therapy has reduced mortality rates in heart failure patients, they are not without their own complications that require implementation of effective monitoring strategies to mitigate the risks as successfully as possible. The prevalence of diuretic therapy complications in heart failure patients is difficult to determine due to the diversity among the populations being studied, different treatment strategies, existence of multiple co-morbidities among patients as well as the occurrence of various complications with each diuretic. The purpose of this review is to evaluate the use of diuretics in congestive heart failure (CHF) and to understand the complications of different classes of diuretics which is essential for successful management of pulmonary and venous congestion in patients with heart failure and hence to optimise the outcome for the patients.
Diagnosis and management of congestive heart failure
As heart failure is classed as a syndrome, specific criteria are required to achieve a diagnosis. Several criteria have been developed including the European Society of Cardiology criteria, the Framingham criteria, the Gothenburg criteria and the Boston criteria [Citation16–19]. Common signs and symptoms of heart failure include dyspnoea, paroxysmal nocturnal dyspnoea, edoema, orthopnoea, fatigue, abdominal pain and swelling [Citation20,Citation21]. Physical exam findings indicative of fluid retention includes peripheral edoema, jugular venous distension, ascites, bibasilar rales, S3 gallop [Citation3,Citation20].
Diagnosis of suspected HF is achieved using the following initial tests:
Chest X-ray
12-lead electrocardiogram (ECG)
Blood test (liver function tests, complete blood count, serum chemistries, fasting lipid profile and TSH
B-type natriuretic peptide (BNP)
Transthoracic echocardiography (TTE) [Citation3]
The American College of Cardiology/American Heart Association/Heart Failure Society of America (ACC/AHA/HFSA) guidelines provide strong recommendations for the use of diuretics in HFrEF patients with associated volume overload [Citation3]. gives the clinical context and class of indication for various diuretics. The NICE guidelines 2018 advise the routine use of diuretics for the treatment of congestive symptoms and the retention of fluid in HF patients [Citation22]. First line diuretics used in the treatment of congestive heart failure include loop diuretics which most commonly include furosemide, bumetanide and torsemide. Evidence consistently indicates that for the treatment of heart failure, bumetanide and torsemide are more effective than furosemide at reducing dyspnoea, weight loss, fatigue all-cause mortality and hospital readmissions [Citation23–26]. Thiazide and thiazide-like diuretics including metolazone, chlorothiazide, and hydrochlorothiazide are considered in hypertensive HF patients who are not adequately responsive to a single diuretic. Potassium sparing diuretics such as spironolactone and eplerenone are considered in the hypokalemic HF patient. ACC/AHA/HFSA guidelines give strong recommendations for the use of the aforementioned potassium sparing diuretics in those with a left ventricular ejection fraction (LVEF) ≤35% and who are categorised in Class III of the New York Heart Association Classification (NYHA). Arginine vasopressin receptor antagonists (vaptans), which inhibit the action of vasopressin, are considered in HF patients that are unresponsive to optimal loop diuretic medical intervention and have severe and persistent hypervolaemic hyponatraemia [Citation3,Citation27]. Dapaglifozin, a sodium – glucose cotransporter 2 (SGL2) inhibitor) has also been found to reduce the risk of hospitalisation and cardiovascular death and is approved for NYHA Class II – IV HFrEF patients [Citation28]. Management of HFrEF also includes strong recommendations for the use of angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB’s) and beta-blockers [Citation3].
Table 1. Clinical context and class of indication for diuretic treatments [Citation3, Citation13].
Complications of diuretic therapy
Complications of diuretic therapy in patients with heart failure is often specific to the type of diuretic and the dose required to achieve decongestion. The most common adverse effects of diuretics include electrolyte and fluid balance abnormalities, which can be seen across many of the drugs discussed in this review. Electrolyte and fluid imbalances due to diuretic utilisation include hypokalaemia [Citation29], hyponatraemia, hypovolaemia, metabolic acidosis and hypomagnesemia [Citation3]. An overview of the most common complications and management strategies are presented in .
Figure 1. Complications of potassium sparing diuretics, loop diuretics and thiazide diuretics with respective management strategies.
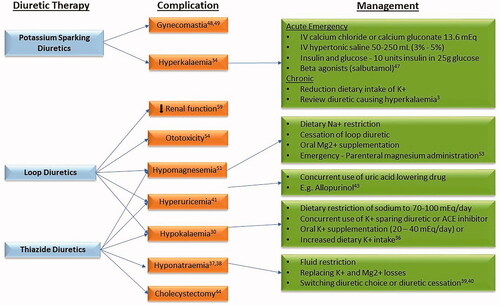
Thiazide diuretics
Thiazide diuretics have been shown to cause hypokalaemia, and therefore increase the risk of cardiac arrhythmias [Citation30,Citation31]. A large cohort study investigating over 350,000 adults over 3 years found that the prevalence of hypokalaemia defined as serum potassium <3.5 mEq/L in patients taking loop or thiazide diuretics was 13.6%. Factors associated with an increased risk of hypokalaemia included hypertension, female sex, thiazide or loop diuretic use, and treatment with blood pressure medications [Citation32]. Hypokalaemia prevalence and severity is dose dependent and it typically occurs within 2 weeks after diuretic commencement [Citation33]. There is an increased risk of hypokalaemia associated with thiazide and thiazide-like diuretics when compared with loop diuretics. This may be, in part, down to the significantly longer half-life of the former [Citation33]. Correction of decreased serum potassium levels is of great importance in order to avoid the increased risk of digoxin toxicity, ventricular arrhythmias, and glucose intolerance associated with hypokalaemia [Citation34]. In cases of mild hypokalaemia, dietary restriction of sodium may be sufficient to correct reduced levels of potassium [Citation35]. Further strategies used to restore a normal potassium level include concurrent use of a potassium sparing diuretic, ACE inhibitor or oral potassium supplementation [Citation36].
Hyponatraemia is also a serious complication of diuretic management, particularly with use of thiazide diuretics and occurs more commonly in elderly females within the first 2 weeks of diuretic initiation [Citation37,Citation38]. Management of mild hyponatraemia, classified as 125 − 135 mmol/L can be achieved with fluid restriction, replacing potassium losses and potentially switching to an alternative diuretic or diuretic cessation [Citation39,Citation40]. Thiazide and loop diuretics, alone or in combination, can also precipitate elevated serum uric acid levels known as hyperuricaemia [Citation41]. Thiazides and loop diuretics increase urate reabsorption in the proximal renal tubules and is an independent risk factor for the development of gout [Citation41,Citation42]. Management of HF patients with hyperuricaemia includes concurrent use of uric acid lowering drugs such as allopurinol with thiazide diuretics [Citation43]. Thiazide diuretics have also been shown to be associated with an increased risk of cholecystectomy in females. A prospective cohort study of 81,351 women in the United States between the ages of 30–55 years were followed for 20 years. 8, 607 of these subjects had a cholecystectomy. The multivariate risk of cholecystectomy in those using thiazide diuretics was 1.16 for past users and 1.39 for current users [Citation44]. Hypomagnesemia is also a complication associated with use of thiazide diuretics and will be discussed under loop diuretics [Citation45].
Potassium-sparing diuretics
A complication of potassium-sparing diuretics that must be monitored is hyperkalaemia. The prevalence of elevated serum potassium is approximately 9% in patients using spironolactone [Citation34]. Concurrent use of potassium sparing drugs with ACE inhibitors must be monitored due to an increased risk of hyperkalaemia. A 2003 study investigating combined use of spironolactone with ACE inhibitors or angiotensin receptor blockers in heart failure patients identified a significant risk of life-threatening hyperkalaemia. Predisposing factors identified for the occurrence of severe hyperkalaemia include age (mean age of 76), increased dose of spironolactone (mean dose 88 mg/day), diabetes type 2 and reduced renal function [Citation46]. Monitoring of potassium, dosing, and renal function with the use of potassium sparing diuretics is also essential due to the increased risk of hyperkalemia [Citation3].
Management of hyperkalaemia includes administration of IV calcium gluconate or chloride, IV hypertonic saline, insulin and glucose and a beta agonist such as salbutamol [Citation47]. In chronic hyperkalaemia reduction of dietary potassium or review of the diuretic causing hyperkalaemia is sufficient. In addition to hyperkalaemia, the aldosterone antagonist, spironolactone, has an increased risk of producing the adverse effect of gynaecomastia [Citation48,Citation49]. A study published by Hallizullah et al found that gynaecomastia and gastrointestinal were more pronounced when spironolactone was used concurrently with furosemide compared to when furosemide was coupled with amiloride [Citation50].
Loop diuretics
Loop diuretics, like thiazides, have also been found to increase the risk of hypokalaemia and hypomagnesemia [Citation51]. Heart failure patients are particularly susceptible to hypomagnesemia due to a higher loop diuretic dose requirement over a prolonged period of time [Citation52]. The most effective emergency intervention for hypomagnesemia is parenteral administration of magnesium. For a mild hypomagnesemic state, restriction of Na + and diuretic intake should be considered. Oral supplementation of magnesium can be taken in the form of Mg2+ gluconate [Citation53]. High doses of the IV loop diuretic furosemide (240 mg/hour) have been suggested to precipitate Loop diuretic induced ototoxicity [Citation54]. This ototoxicity can be transient, lasting between 30 mins to 24 h, or more serious permanent damage can occur leading to deafness. While high doses are generally required (240 mg/hour), acute/chronic renal impairment or concurrent use of ototoxic drugs such as aminoglycosides can precipitate ototoxicity at significant lower doses [Citation55]. The potential physiological mechanisms underpinning this complication is thought to be associated with interaction of loop diuretics with a secretory isoform of the Na+/K+/2Cl- transporter that plays a role in endolymph production [Citation56]. A Cochrane review in 2005 investigating infusion versus bolus injection of loop diuretics in CHF identified transient tinnitus and hearing loss in patients administered bolus injections. Interestingly, the presence of these symptoms did not necessitate cessation of the drug [Citation57]. Loop diuretics have also been found to have adverse haemodynamic effects such as decreasing pulmonary wedge pressure which may be explained by the enhanced prostaglandin synthesis associated with loop diuretic utilisation [Citation58]. Loop diuretics have also been associated with worsening renal function and increasing diuretic dose has shown to increase the risk of mortality at 6 months [Citation59]. Cotter et al. also examined the potential toxicities associated with high dose loop diuretics in a small group of 20 patients with refractory congestive heart failure. The study found that there was significant decrease in mean arterial pressure and deterioration in renal function in patients treated with intravenous furosemide [Citation60]. Further to these findings, continuous and repetitive administration of high dose loop diuretics such as furosemide can lead to the development of tolerance and ultimately diuretic resistance. One of the primary mechanisms responsible for resistance is due to compensatory sodium reabsorption in the kidneys [Citation61–64].
Diuretic resistance
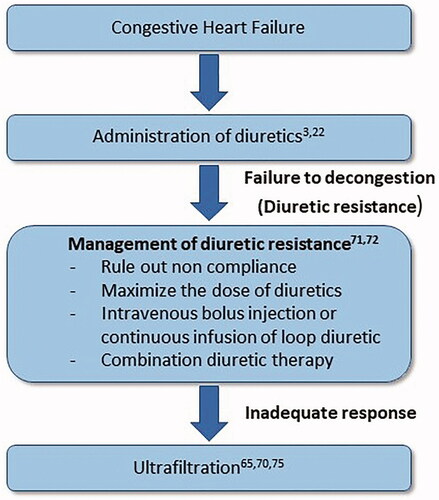
Diuretic resistance (DR) is a common problem in patients with heart failure. There is no single accepted definition for diuretic resistance, but the most commonly used definition is ‘failure to decongest despite adequate and escalating doses’ [Citation65]. The physiology underpinning DR along with predictors of such an outcome are important considerations for clinicians in the treatment of heart failure patients. With a decline in extracellular volume, secondary adaptations can manifest that impact diuretic response, often called the ‘braking phenomenon’. Adaptations can include activation of the renin-angiotensin-aldosterone system, sympathetic nervous system stimulation and nephron remodelling, all of which can contribute to DR development [Citation66]. A study done in a cohort of elderly patients with decompensated HF found that patients with DR had more comorbidities like diabetes mellitus, hypercholesterolaemia, valvular disease, chronic disease, and cancer. The prevalence of DR in this cohort of patients was 21% (435 out of 2037 patients) [Citation67]. Another study analysed DR in patients with a focus on insufficient symptom relief and loop diuretic dosing during the first 24 h after admission. This study analysed data from 51,013 patients from the ADHERE registry (Acute decompensated Heart Failure National Registry). Among these patients, 33% lost ≥2.27 kg and 16% actually gained weight during hospitalisation [Citation68]. Different studies use different parameters such as weight loss, urine output or natriuresis to diagnose DR [Citation65,Citation69]. Due to this lack of formal definition of DR, it is difficult to properly assess the prevalence of diuretic resistance [Citation67,Citation70]. Several strategies have been suggested for the management of diuretic resistance (), which include sodium intake restriction, changes in diuretic dose, combination diuretic therapy and intravenous diuretic administration [Citation71,Citation72]. Further investigation is still required in this area of study to determine the predictors of diuretic resistance in patients with heart failure and to explore the management strategies of diuretic resistance.
Figure 2. Management of diuretic resistance.
Alternative therapies
The existence of diuretic resistance and complication of diuretics in heart failure patients have prompted for the research into effective and safer alternatives. Ultrafiltration is considered an alternative approach to diuretic therapy for the treatment of patients with congestive heart failure. The process of ultrafiltration involves the production of plasma from a patient’s blood across a haemofilter or semipermeable membrane [Citation73]. A meta-analysis done to compare the efficacy and safety of high dose diuretics and ultrafiltration in the management of decompensated heart failure revealed that ultrafiltration was associated with significant reduction in the rate of re-hospitalisation. However, ultrafiltration did not produce any apparent beneficial effects for weights loss, length of hospitalisation for HF, mortality, change in serum creatinine, dialysis dependence and adverse outcomes [Citation74]. Some studies suggest that ultrafiltration can be useful in patients with refractory diuretic resistance [Citation65,Citation70,Citation75]. Vasopressin receptor inhibitors like tolvaptan have also been identified as alternative therapy to manage congestion in high-risk patients with acute heart failure. Tolvaptan alone in comparison to placebo and dual therapy of tolvaptan and furosemide in comparison to furosemide alone have shown to be associated with decrease in body weight and increased urine volume [Citation76]. The therapeutic potential of synthetic natriuretic peptides has also been investigated in the management of congestive heart failure based on their vasodilatory and diuretic properties and effective inhibition of renin-angiotensin aldosterone system. Nesiritide, a recombinant form of B-natriuretic peptide is associated with dyspnoea relief and improvements in haemodynamic functions in patients [Citation77,Citation78]. Low dose dopamine has also been explored as a therapy that may enhance decongestion and also preserve renal function in patients with refractory congestive heart failure [Citation60].
Conclusion
In heart failure patients, fluid overload is a major pathological mechanism leading to pulmonary and systemic congestion. Diuretics continue to play a central role in patients with heart failure to relieve the symptoms of congestion. However, different complications like electrolyte imbalances (hypokalaemia, hyponatraemia, hypomagnesemia) and worsening renal function may arise from the administration of diuretics. Thus, the use of diuretics in patients with congestive heart failure should be continuously monitored for the development of these adverse effects.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Disclosure statement
The authors declare that they have no conflict of interest.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
References
- Hunt SA. American College of C, American Heart Association Task Force on Practice G. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol. 2005;46(6):e1-82.
- Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):1977–2016.
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Card Fail. 2017;23(8):628–651.
- Braunwald E. Shattuck lecture-cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337(19):1360–1369.
- Go AS, Mozaffarian D, Roger VL, American Heart Association Statistics Committee and Stroke Statistics Subcommittee, et al. Executive summary: heart disease and stroke statistics-2014 update: a report from the American Heart Association. Circulation. 2014;129(3):399–410.
- Ryden-Bergsten T, Andersson F. The health care costs of heart failure in Sweden. J Intern Med. 1999;246(3):275–284.
- Heidenreich PA, Albert NM, Allen LA, Stroke Council, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606–619.
- Pellicori P, Kaur K, Clark AL. Fluid management in patients with chronic heart failure. Card Fail Rev. 2015;1(2):90–95.
- de Silva R, Rigby AS, Witte KK, et al. Anemia, renal dysfunction, and their interaction in patients with chronic heart failure. Am J Cardiol. 2006;98(3):391–398.
- Mullens W, Abrahams Z, Francis GS, et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol. 2009;53(7):589–596.
- Damman K, van Deursen VM, Navis G, et al. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol. 2009;53(7):582–588.
- Colombo PC, Onat D, Harxhi A, et al. Peripheral venous congestion causes inflammation, neurohormonal, and endothelial cell activation. Eur Heart J. 2014;35(7):448–454.
- Ponikowski P, Voors AA, Anker SD, Bueno H, Document Reviewers, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975.
- Dynamed. Diuretics for Heart Failure. [Internet] Ipswich (MA): EBSCO Information Services 1995 – Record No T901136. 2018.
- Brater C. Mechanism of action of diuretics. Waltham, MA: UpToDate; 2020.
- Swedberg K, Cleland J, Dargie H, Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology, et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26(11):1115–1140.
- McKee PA, Castelli WP, McNamara PM, et al. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285(26):1441–1446.
- Eriksson H, Caidahl K, Larsson B, et al. Cardiac and pulmonary causes of dyspnoea-validation of a scoring test for clinical-epidemiological use: the Study of Men Born in 1913. Eur Heart J. 1987;8(9):1007–1014.
- Carlson KJ, Lee DC, Goroll AH, et al. An analysis of physicians' reasons for prescribing long-term digitalis therapy in outpatients. J Chronic Dis. 1985;38(9):733–739.
- Lindenfeld JAnn, Albert NM, Boehmer JP, Heart Failure Society of America, et al. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail. 2010;16(6):e1–194. Commentary can be found in J Card Fail 2011;17(1):1.
- Thibodeau JT, Drazner MH. The role of the clinical examination in patients with heart failure. JACC Heart Fail. 2018;6(7):543–551.
- NICE. Diagnosis and management of adults with chronic heart failure: summary of updated NICE guidance. BMJ. 2018;362:k4080.
- Wargo KA, Banta WM. A comprehensive review of the loop diuretics: should furosemide be first line? Ann Pharmacother. 2009;43(11):1836–1847.
- DiNicolantonio JJ. Should torsemide be the loop diuretic of choice in systolic heart failure? Future Cardiol. 2012;8(5):707–728.
- Murray MD, Deer MM, Ferguson JA, et al. Open-label randomized trial of torsemide compared with furosemide therapy for patients with heart failure. Am J Med. 2001;111(7):513–520.
- Cosin J, Diez J, Investigators T. Torasemide in chronic heart failure: results of the TORIC study. Eur J Heart Fail. 2002;4(4):507–513.
- Lapsia V, Kazory A. Loop diuretics for heart failure-associated hyponatremia. Am J Med. 2010;123(8):e5–e6.
- McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008.
- Kardalas E, Paschou SA, Anagnostis P, et al. Hypokalemia: a clinical update. Endocr Connect. 2018;7(4):R135–R46.
- Velazquez H, Wright FS. Control by drugs of renal potassium handling. Annu Rev Pharmacol Toxicol. 1986;26:293–309.
- Siegel D, Hulley SB, Black DM, et al. Diuretics, serum and intracellular electrolyte levels, and ventricular arrhythmias in hypertensive men. JAMA. 1992;267(8):1083–1089.
- Nilsson E, Gasparini A, Arnlov J, et al. Incidence and determinants of hyperkalemia and hypokalemia in a large healthcare system. Int J Cardiol. 2017;245:277–284.
- Palmer BF. Metabolic complications associated with use of diuretics. Semin Nephrol. 2011;31(6):542–552.
- Sarafidis PA, Georgianos PI, Lasaridis AN. Diuretics in clinical practice. Part II: electrolyte and acid-base disorders complicating diuretic therapy. Expert Opin Drug Saf. 2010;9(2):259–273.
- Blanning A, Westfall JM, Shaughnessy AF. Clinical inquiries. How soon should serum potassium levels be monitored for patients started on diuretics? J Fam Pract. 2001;50(3):207–208.
- Cohn JN, Kowey PR, Whelton PK, et al. New guidelines for potassium replacement in clinical practice: a contemporary review by the National Council on Potassium in Clinical Practice. Arch Intern Med. 2000;160(16):2429–2436.
- Ayus JC. Diuretic-induced hyponatremia. Arch Intern Med. 1986;146(7):1295–1296.
- Ashraf N, Locksley R, Arieff AI. Thiazide-induced hyponatremia associated with death or neurologic damage in outpatients. Am J Med. 1981;70(6):1163–1168.
- Szatalowicz VL, Miller PD, Lacher JW, et al. Comparative effect of diuretics on renal water excretion in hyponatraemic oedematous disorders. Clin Sci (Lond). 1982;62(2):235–238.
- Sonnenblick M, Friedlander Y, Rosin AJ. Diuretic-induced severe hyponatremia. Review and analysis of 129 reported patients. Chest. 1993;103(2):601–606.
- Bruderer S, Bodmer M, Jick SS, et al. Use of diuretics and risk of incident gout: a population-based case-control study. Arthritis Rheumatol. 2014;66(1):185–196.
- McAdams DeMarco MA, Maynard JW, Baer AN, et al. Diuretic use, increased serum urate levels, and risk of incident gout in a population-based study of adults with hypertension: the Atherosclerosis Risk in Communities cohort study. Arthritis Rheum. 2012;64(1):121–129.
- Sica DA, Carter B, Cushman W, et al. Thiazide and loop diuretics. J Clin Hypertens (Greenwich). 2011;13(9):639–643.
- Leitzmann MF, Tsai CJ, Stampfer MJ, et al. Thiazide diuretics and the risk of gallbladder disease requiring surgery in women. Arch Intern Med. 2005;165(5):567–573.
- Casu G, Merella P. Diuretic therapy in heart failure - current approaches. Eur Cardiol. 2015;10(1):42–47.
- Wrenger E, Muller R, Moesenthin M, et al. Interaction of spironolactone with ACE inhibitors or angiotensin receptor blockers: analysis of 44 cases. BMJ. 2003;327(7407):147–149.
- Sidhu K, Sanjanwala R, Zieroth S. Hyperkalemia in heart failure. Curr Opin Cardiol. 2020;35(2):150–155.
- Brater DC. Diuretic therapy. N Engl J Med. 1998;339(6):387–395.
- Brater DC. Update in diuretic therapy: clinical pharmacology. Semin Nephrol. 2011;31(6):483–494.
- Hafizullah M. Comparative efficacy and tolerability of lasoride and spiromide in congestive cardiac failure. J Postgrad Med Inst. 2011;14(1):36–42.
- Cooper HA, Dries DL, Davis CE, et al. Diuretics and risk of arrhythmic death in patients with left ventricular dysfunction. Circulation. 1999;100(12):1311–1315.
- Petri M, Cumber P, Grimes L, et al. The metabolic effects of thiazide therapy in the elderly: a population study. Age Ageing. 1986;15(3):151–155.
- Dyckner T, Wester PO. Effects of magnesium infusions in diuretic induced hyponatraemia. Lancet. 1981;1(8220 Pt 1):585–586.
- Cook DJ, Tudball CF. Potentiators and bolus intravenous furosemide. Lancet. 2001;358(9290):1373–1374.
- Gallagher KL, Jones JK. Furosemide-induced ototoxicity. Ann Intern Med. 1979;91(5):744–745.
- Delpire E, Lu J, England R, et al. Deafness and imbalance associated with inactivation of the secretory Na-K-2Cl co-transporter. Nat Genet. 1999;22(2):192–195.
- Salvador DR, Rey NR, Ramos GC, Punzalan FE. Continuous infusion versus bolus injection of loop diuretics in congestive heart failure. Cochrane Database Syst Rev. 2004;(3):CD003178. DOI:https://doi.org/10.1002/14651858.CD003178.pub3
- Raftery EB. Haemodynamic effects of diuretics in heart failure. Br Heart J. 1994;72(2 Suppl):S44–S7.
- Hasselblad V, Gattis Stough W, Shah MR, et al. Relation between dose of loop diuretics and outcomes in a heart failure population: results of the ESCAPE trial. Eur J Heart Fail. 2007;9(10):1064–1069.
- Cotter G, Weissgarten J, Metzkor E, et al. Increased toxicity of high-dose furosemide versus low-dose dopamine in the treatment of refractory congestive heart failure. Clin Pharmacol Ther. 1997;62(2):187–193.
- Wilcox CS, Mitch WE, Kelly RA, et al. Response of the kidney to furosemide. I. Effects of salt intake and renal compensation. J Lab Clin Med. 1983;102(3):450–458.
- Hammarlund MM, Odlind B, Paalzow LK. Acute tolerance to furosemide diuresis in humans. Pharmacokinetic-pharmacodynamic modeling. J Pharmacol Exp Ther. 1985;233(2):447–453.
- Cook JA, Smith DE. Development of acute tolerance to bumetanide: bolus injection studies. Pharm Res. 1987;4(5):379–384.
- Cook JA, Smith DE. Development of acute tolerance to bumetanide: constant-rate infusion studies. Pharm Res. 1988;5(2):86–91.
- ter Maaten JM, Valente MA, Damman K, et al. Diuretic response in acute heart failure-pathophysiology, evaluation, and therapy. Nat Rev Cardiol. 2015;12(3):184–192.
- Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Ann Intern Med. 1991;114(10):886–894.
- Trullas JC, Casado J, Morales-Rull JL, et al. Prevalence and outcome of diuretic resistance in heart failure. Intern Emerg Med. 2019;14(4):529–537.
- Gheorghiade M, Filippatos G. Reassessing treatment of acute heart failure syndromes: the ADHERE Registry. Eur Heart J Suppl. 2005;7(suppl_B):B13–B19.
- Jardim SI, Ramos Dos Santos L, Araujo I, et al. A 2018 overview of diuretic resistance in heart failure. Rev Port Cardiol. 2018;37(11):935–945.
- Iqbal J, Javaid MM. Diuretic resistance and its management. Br J Hosp Med (Lond). 2014;75(7):C103–7.
- Shah N, Madanieh R, Alkan M, et al. A perspective on diuretic resistance in chronic congestive heart failure. Ther Adv Cardiovasc Dis. 2017;11(10):271–278.
- De Bruyne LK. Mechanisms and management of diuretic resistance in congestive heart failure. Postgrad Med J. 2003;79(931):268–271.
- Ronco C, Ricci Z, Bellomo R, et al. Extracorporeal ultrafiltration for the treatment of overhydration and congestive heart failure. Cardiology. 2001;96(3-4):155–168.
- Shi X, Bao J, Zhang H, et al. Patients with high-dose diuretics should get ultrafiltration in the management of decompensated heart failure: a meta-analysis. Heart Fail Rev. 2019;24(6):927–940.
- Verbrugge FH, Mullens W, Tang WH. Management of cardio-renal syndrome and diuretic resistance. Curr Treat Options Cardiovasc Med. 2016;18(2):11.
- Udelson JE, Bilsker M, Hauptman PJ, et al. A multicenter, randomized, double-blind, placebo-controlled study of tolvaptan monotherapy compared to furosemide and the combination of tolvaptan and furosemide in patients with heart failure and systolic dysfunction. J Card Fail. 2011;17(12):973–981.
- Mills RM, LeJemtel TH, Horton DP, et al. Sustained hemodynamic effects of an infusion of nesiritide (human b-type natriuretic peptide) in heart failure: a randomized, double-blind, placebo-controlled clinical trial. Natrecor Study Group. J Am Coll Cardiol. 1999;34(1):155–162.
- Publication Committee for the VI. Intravenous nesiritide vs nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial. JAMA. 2002;287(12):1531–1540.

