
Abstract
Objective
To estimate the prevalence of dental erosive wear among five-year-olds in Bergen, Norway, and to investigate associations between background factors and the condition.
Methods
A total of 387 children received a dental examination in five Public Dental Service clinics in Bergen, Norway. The parents responded to items about the children’s dental hygiene and drinking habits, type of beverage container, diet, and other habits, and about their own age, educational level and country of origin. We explored background variables for possible associations with the outcome status as worst affected by erosive wear (19.4%, n = 75). Chi-squared statistics and logistic regression (Odds Ratios (OR): 95% Confidence Intervals (CI), served as statistical tools).
Results
Approximately 80% showed erosive wear (by SEPRS and by adopted diagnostic instrument (78.5% vs 79.8%)). The condition affected maxillary anterior teeth in 13.9% (n = 54), and cuppings in molars in 79.3% (n = 307) of cases. Grinding teeth during the day and/or night (OR: 1.87, CI: 1.07–3.25) and male sex (OR: 1.76, CI: 1.05–2.96) significantly related to outcome status as worst affected by erosive wear, respectively.
Conclusion
Dental erosive wear was widespread. Grinding teeth and male sex associated with outcome status as worst affected by erosive wear.
Introduction
The collective term ‘erosive tooth wear’ is defined as ‘a chemical-mechanical process resulting in a cumulative loss of hard dental tissue not caused by bacteria’ [Citation1]. Among children and adolescents in developed countries, this type of tooth structure loss has become a common dental condition and a source of concern. Making an acceptable diagnosis can be challenging, especially in primary teeth. Distinguishing dental erosion from mechanical forces such as attrition and abrasion is difficult. One reason for this is that erosive tissue loss may also account for physiological tooth wear [Citation2]. Acid exposure in the dental erosion process can soften the enamel surface, thereby exacerbating the physical wear process. This process may be faster in the primary dentition due to thinner enamel and lower mineralization levels than in permanent teeth [Citation3].
The multifactorial aetiology of erosive tooth wear [Citation4] may result from intrinsic factors, such as gastro-oesophageal reflux and vomiting [Citation5], extrinsic factors, such as acidic food or drinks or medication, or occupational environmental factors [Citation6]. Diet plays an important and complex role, as the erosive potential of dietary factors depends not only on pH, but also on the type of acid, the buffering capacity and the chelation effect of diet [Citation7]. Futhermore, the intake frequency of carbonated drinks, natural fruit juices, acidic snacks or sweets increases the risk of dental erosive wear [Citation8]. The impact of sex on dental erosive wear, however, shows divergent results [Citation9,Citation10].
The prevalence of dental erosive wear reaching into the dentine layer increases with age [Citation10,Citation11] and, since the dentine is softer than enamel, the destructive process might be faster from that stage on. It is important for clinicians to bear in mind that erosive wear in the primary dentition increases fourfold the risk for erosive tooth loss in the permanent dentition [Citation12]. This knowledge should be especially emphasized when implementing preventive strategies in children [Citation13]. A prerequisite for successful prevention is to diagnose both risk factors and potential interactions between them.
Although the enamel layer in primary teeth is thinner and less mineralized than in permanent teeth [Citation3,Citation14], whether this layer is more susceptible to erosive wear remains a matter of dispute. Some in vitro studies show that the enamel in primary teeth is more susceptible [Citation15,Citation16], whereas others report no differences in susceptibility [Citation17–19]. As in permanent teeth, epidemiological studies focussing on dental erosion in primary teeth show wide-ranging prevalence [Citation20]. Figures from Europe among five-year-olds vary from 30% to 98% [Citation21–25], and it is commonly accepted that this condition is prevalent in pre-school children [Citation20]. This variability may stem from the diagnostic indices used, the number of subjects in the different studies examined, the socio-economic groups targeted, and a lack of information on the age groups involved. Thus, comparing studies is difficult.
A previous study in Norway reported on dental erosive wear in primary teeth in a group of five-year-olds with congenital heart defect [Citation26], but no studies in the general population exist. Among adolescents, studies have reported a prevalence of 38%–59% for dental erosive wear involving enamel [Citation27–29] and 15%–20% for dental erosive wear involving dentine [Citation28,Citation29].
This study aimed to estimate the prevalence of dental erosive wear in the primary dentition of five-year-olds in Bergen, Norway, and to investigate whether background factors associated with the condition.
Materials and methods
Study design
We conducted this cross-sectional clinical study in the Public Dental Service (PDS) in the municipality of Bergen, Norway, from January to mid-June 2018. Clinical examinations and parental surveys provided the data on dental erosive wear among five-year-olds.
Sample size
We calculated the sample size based on the prevalence of dental erosion in a Swedish study that used the same diagnostic tool as in the present study [Citation30]. The Swedish study found the prevalence of erosion extending into the dentine on one or more maxillary anterior teeth/molars to be 13% in a group of five- to six-year-olds. The prevalence in the current, slightly younger group was presumed to be 10%. The total population of five-year-olds in the municipality of Bergen at the time of the study was 3127 (children born in 2013). With the precision for the 95% confidence intervals (CI) set to 3%, we calculated a sample size of 343 children. After taking into account a drop-out rate of 15–16%, we set the final sample size to 408 participants.
Study participants
As in a previous study performed in the same region [Citation31] and to reflect background social gradients, the average number of decayed, missing and filled teeth (d3–5mft-index) served as a proxy for socioeconomic status [Citation32]. We ranked all the PDS clinics (n = 13) from highest to lowest according to their respective d3–5mft score for five-year-olds. We then selected from this list the clinics to be included, from the second highest to the lowest d3–5mft score. Between these first two selected clinics, we included every second clinic on the list, resulting in a total of five clinics from both rural and urban backgrounds. The inclusion criterion for participation was being a healthy five-year-old scheduled for a regular dental check-up at one of the chosen clinics. We excluded children with severe systemic diseases, involving substantive functional limitations, syndromes or rare medical conditions, or children born very prematurely (born before the 28th week of pregnancy). shows a flow chart of the participants.
Figure 1. A flow chart of participants.
The diagnostic tools used included modified versions of a dental erosion scale for index teeth () and a scale for cuppings on molars (), developed by Johansson et al. and by Hasselkvist et al., respectively [Citation30,Citation33]. We examined the same index teeth/surfaces in the present study as in the original versions: buccal and palatal surfaces of the maxillary central and lateral incisors and canines (n = 12) and all occlusal surfaces of the primary molars (n = 8).
Table 1. Ordinal scale used for grading severity of dental erosion on buccal and lingual surfaces of maxillary anterior teeth [33].
Table 2. Ordinal scale used for grading cuppings on occlusal surfaces of first permanent molars and primary molars [Citation30].
Calibration
Before the calibration of the examiners, three experienced paediatric dentists (MSS, AMG, AB) developed a ‘Golden standard’ for the ‘calibration material’. The diagnostic results achieved by consensus among the three. The material consisted of plaster models of primary teeth from 22 children (300 surfaces), including both affected and unaffected surfaces, and of five clinical photos of each child. Afterwards, but prior to the study, six experienced dental hygienists completed a one-day calibration course consisting of educational lessons and exercises. The lessons included discussions based on various cases of dental erosive wear represented with plaster models and photographs. The trainee examiners obtained specific feedback for each diagnosis that deviated from the correct grading. Prior to the first calibration exercise, the examiners received instructions by mail with a request to use previous lecture handouts with emphasis on the dental erosion diagnostic scale. During the calibration session (Timepoint 1) held at each examiner’s local office, the selected dental hygienists diagnosed the ‘calibration material’ previously having been scored by ‘Golden standard’. We then compared each examiner’s scores (Test I) to the ‘Golden standard’ (inter-examiner agreement). A second calibration session followed the same procedure (Timepoint 2) on the ‘calibration material’ approximately three weeks later (mean: 3.5 weeks after Timepoint 1). Intra-examiner agreement analysis (Test II) compared each examiner’s calibration results at Timepoint 1 with those obtained at Timepoint 2. We merged as seen in and some grades due to inconsistencies in the examiners’ ability to distinguish all the different grades in the diagnostic instruments used.
The questionnaire
The questionnaire contained 23 questions for parents to answer on their children’s dental hygiene and drinking habits, type of beverage container, diet, and other habits (bruxism, reflux or snoring). Parents also provided personal information on their age, educational level and country of origin.
Statistical methods
The statistical software package IBM SPSS version 25 (IBM, Armonk, NY) served in processing and analysing the data. The percentage of agreement served as the basis for evaluating inter- and intra-examiner reliability. In addition to the prevalence from the scale for erosion and cuppings, we used the simplified erosion partial recording system (SEPRS) by Hasselkvist et al. [Citation30]. We calculated the prevalence of SEPRS by combining erosion and cuppings at the palatal surfaces of central incisors and the occlusal surfaces of all first primary molars (six surfaces). Chi-squared statistics served to measure differences between groups. In logistic regression models, we categorized the dependent variable ‘Dental Erosive Wear’ into ‘Worst affected by erosive wear’ (1), which included all children in Erosion groups 2 and 3; grade 2 or more, according to original indices on maxillary anterior surfaces (), or belonging to Cupping group 3; grades 3 and 4, according to original indices (), and ‘Mildly/Not affected’ (0). To explore any possible relationship between various independent background variables and the dependent variable, odds ratios (OR) with 95% CIs served as the statistic measurement tool for performing bivariate and multivariate regression analyses. The level of statistical significance was set at five per cent.
Ethical approval
The Regional Committees for Medical and Health Research Ethics (REK) (nr: 2017/1181) and the Norwegian Centre for Research Data (NSD) approved the study. The head of the Hordaland County Dental Health Authorities and the research leader at the Oral Health Centre of Expertise in Western Norway – Hordaland County (TKVest/H) granted permission to conduct the study. In addition, all parents provided their written informed consent prior to participation.
Results
The participation rate of children undergoing examination was 94.9%, while the percentage of parents completing the questionnaire was 93.1%. Most of the parents (65.5%, n = 249) who completed the questionnaire were mothers. The mean age of the children (48% boys) was 4.8 years (SD: 0.27).
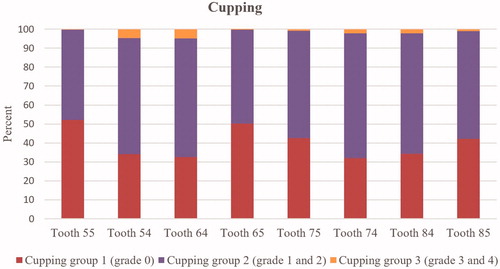
The percentage of agreement for the inter-examiner reliability (Test I) of anterior wear was 64%, and 70% for cuppings. The corresponding values for the intra-examiner test (Test II) were 69% and 80%, respectively. The prevalence of anterior dental erosive wear (Erosion group 2: originally grades 2 and 3) in the maxillary anterior teeth (53–63) was 13.9% (n = 54). Erosion group 3 (originally grade 4) was evident palatinally on teeth 51 and 61 in one girl only. Regarding cuppings, 79.3% (n = 307) of the participants belonged to Cupping groups 2 and 3 (originally grades 1–4). The number of primary molars affected by cuppings varied from 1 molar in 18 children to 8 molars in 152 children. The percentage distribution of cuppings in the first and second primary molars shows that they occurred most frequently in the four first primary molars. In these molars cuppings were evenly distributed (65.8–68.8%) (), but they were more widely distributed in the second primary molars (47.7–57.9%). Cupping group 3 (originally grades 3 and 4) was registered in 8.3% (n = 32) of the children.
Figure 2. Percentage distribution of cupping groups (groups 1, 2, 3)/individuals on first molars (teeth 54, 64, 74, 84) and second primary molars (teeth 55, 65, 75, 85) in all examined children (n = 387).
A majority of the participants (79.8%, n = 309) had at least one tooth with dental erosive wear (palatal grades 2–4 and cupping grades 1–4) with no significant differences between boys and girls (79.8% vs 79.9%, respectively). Altogether 4.7% (n = 18) had one affected tooth, 29.5% (n = 114) had eight affected teeth, and 7.2% (n = 28) had all 14 index teeth affected. Only two children had anterior erosive wear with no cupping in their molars. SEPRS showed a prevalence of 78.5%.
The constructed group ‘Worst affected by erosive wear’ comprised 19.4% (n = 75) of all the children. We investigated various independent variables based on socio-economic background, dental health-related habits, diet and other relevant information for potential allocation into this group. shows the ORs with 95% CIs resulting from the bivariate logistic regression analyses while presents the beforehand dichotomization of the independent variables. Supplementary Tables S1–S3 provide additional detailed background information. The bivariate regression analyses revealed a significant association between two background variables and inclusion in the ‘Worst affected by erosive wear’ group: the habit of grinding the teeth during the day and/or night (OR: 1.82, 95% CI: 1.05–3.15) and male sex (OR: 1.78, 95% CI: 1.06–2.95). These two variables were also the only variables left in the model after the final multivariate regression analysis, which included four background variables: Sex, Grinding the teeth during the night and/or day, Bottle-feeding with acid, Snoring ( or Supplementary Table S3). Grinding the teeth during the day and/or night and male sex showed OR values of 1.87 (95% CI: 1.07–3.25) and 1.76 (95% CI: 1.05–2.96), respectively.
Table 3. Results of both bivariate and multiple logistic regression (ORs with CIs) of possible relationship between various independent background variables and allocation into the group ‘Worst affected by erosive wear’ (n = 75).
Table 4. Various independent variables dichotomized and used in the regression analyses.
Altogether 14.2% (n = 53/372) and 13.8% (n = 51/368) of the subjects consumed juice concentrate and fruit juice, respectively, at least daily. Drinking frequency showed no difference between sexes (Supplementary Table S2). Reports indicated that only two boys drank soft drinks daily. A total of 17.7% (n = 67) of the parents who responded to this question bottle fed their children with acid drinks in their early years, but only nine children on a daily basis.
Ten children reported having reflux, of which eight had at least one tooth with erosive wear. Only one of these eight children received medication for the condition. Fifty-four children (14%) received medication, mostly for asthma (n = 44 (n = 19 when needed, n = 1 previously used, n = 24 on regular medication)). Among these, 86.4% showed dental erosive wear.
Discussion
To the best of our knowledge, this is the first Norwegian study to examine dental erosive wear in the primary dentition of the general Norwegian population. Dental erosive wear was widespread among Norwegian five-year-old children. The worst affected group included significantly more boys than girls. Diet showed no association with the group worst affected. Evidence of a relationship between dental erosive wear in the primary teeth and in the permanent teeth later in life [Citation12] may help to identify children at risk for developing erosive wear in the permanent dentition and target them for preventive strategies at an early stage.
The observed prevalence of dental erosive wear was nearly 80%. Although comparison between studies is challenging due to variability of the diagnostic tools used, our finding was in accordance with two studies of five-year-olds: one from Greece (79%) and another from Malta (81%) [Citation23,Citation24]. SEPRS or the original defined partial recording system showed only a negligible difference in findings. This consolidated the SEPRS finding of a Swedish study, from which the current study adopted the diagnostic instrument [Citation30]. SEPRS is a quick way to determine the need for further and more extensive investigations of dental erosive wear [Citation30]. Including SEPRS in all regular check-ups should be recommended to identify children in need of extended examination, closer follow-up and advice about diagnosed dental erosive wear.
The Swedish study [Citation30] found that dental erosion affected all the children. Compared to the present study, the children in the Swedish study were approximately one year older, and in that study also grade 1 on maxillary anterior teeth were recorded. The fact that tooth wear increases with age [Citation10] suggests that the prevalence in our study was comparable to that in the Swedish study. Recent decades have seen a steadily rising trend in dental erosive wear in many countries. One study reported an increase in prevalence from 30.5% to 58.8% among children in Germany who attended kindergarten during 2004–2014 [Citation25].
In this study a group was constructed which constituted approximately 20% of the children most heavily affected by erosive wear. One background variable, the habit of grinding the teeth during the day and/or night, significantly associated with erosive wear. The odds ratio in this study was 1.87, whereas a three-year longitudinal study conducted in the Netherlands among individuals (mean age: 11.9 years) found an odds ratio of 4.03 between this habit and the incidence of erosive wear in children [Citation34]. The other variable found to associate with teeth most heavily affected by erosive wear was male sex. Our finding of an association between male sex and teeth mostly affected by dental erosive wear was consistent with the finding in a study of participants of comparable age [Citation25], but not with other studies [Citation23,Citation30]. In older age groups, boys were more often affected [Citation29,Citation30].
Although many studies have focussed on the association between various background variables and dental erosive wear, the link between socio-economic status and dental erosive wear remains somewhat divergent. Whereas one study from Greece of five- to seven-year-olds found no association between socio-economic status and dental erosive wear [Citation22], another of five-year-olds showed that high family income and low maternal education associated with Basic Erosive Wear Examination (ΒΕWE) cumulative scores [Citation23]. A study from Malta found lower dental erosion among five-year-olds of parents with higher education [Citation24]. Other studies of older children and adolescents that investigated whether background origin associates with dental erosive wear have found inconsistent results [Citation27,Citation35–38]. The present study found no association between either parental education or parental background origin and dental erosive wear.
Many researchers consider diet and the intake of acidic food/drinks to be important aetiological factors in the development of dental erosive wear. The lack of identification of this relationship in our study, however, may stem from the relatively young age of our participants, as their teeth had not been exposed long enough to be affected. Furthermore, the responses to the questionnaire revealed that only 14% of the children drank juice concentrate or fruit juice daily. In line with our results, a German study of two- to seven-year-olds found that their intake of citrus fruits or acidic drinks (fruit drinks, lemonade, cola) was not associated with the presence of erosion [Citation21]. However, one study from Greece of five- to seven-year-olds found that soft drinks associated with dental erosive wear and that each additional year of exposure and several servings of soft drinks per week resulted in more dental wear [Citation22]. Another study of pre-school children in Germany found the regular (more than once a week) intake of fruit juices or lemonade/coke to increase dental erosive wear [Citation25].
In this study, consumption of acidic beverages showed no difference between sexes. This result is in line with the results of the Swedish study of five- to six-year-olds referred to previously [Citation30], but contrasts with those found among adolescents, reporting a markedly higher consumption of soft drinks among boys.
In addition, the use of a feeding bottle with acidic contents is reported to be associated with later development of dental erosion [Citation39]. As did another study [Citation21], the present study found no such an association. Furthermore, another study has reported less dental erosive wear among those with prolonged use of feeding bottle [Citation22], suggesting that this practice could indicate low masticatory activity and thus decreased occlusal wear.
While asthma in some studies has not shown any association with erosive wear [Citation22,Citation40,Citation41], one study from Birmingham found that asthma and gastro-oesophageal reflux disease (GERD) in adolescents associated with a higher prevalence of dental erosive wear than in a control group [Citation42]. Children and adolescents diagnosed with GERD also showed a higher prevalence of asthma [Citation43]. Likewise, GERD was reportedly more prevalent (75%) in patients diagnosed with asthma than in controls [Citation44]. So, if a patient is diagnosed with asthma and dental erosive wear, the dentist should investigate the aetiology of the dental erosive wear while keeping GERD in mind as a possible condition.
The literature contains discussions of whether tooth brushing associates with erosive wear, as those without plaque also show more erosive wear [Citation45]. On the other hand, some studies have reported less erosive wear among those who brush their teeth twice or more daily [Citation46,Citation47], though others have found no such association [Citation21,Citation23,Citation25,Citation37]. This study found no association between tooth brushing as an oral hygiene behaviour and dental erosive wear.
Strengths and limitations
One strength of the present study was its inclusion of both rural and urban areas as well as participants from varied socio-economic backgrounds. The participation rate in the study was high, and because nearly all children and adolescents in Norway (98.4% in 2018) visit PDS clinics [Citation48], readers can consider the study’s representativeness for this age group in the Bergen population (though not for all of Norway) optimal.
The high number of examiners could be a limitation. Despite a proper calibration programme, misclassifications may have occurred, especially when diagnosing challenging initial erosive wear [Citation49,Citation50]. We avoided using grade 1 when diagnosing maxillary anterior teeth in order to take this issue into account.
Another limitation was our use of a questionnaire which had not been validated and piloted. In addition, self-reporting bias may have occurred, as caregivers in the present cross-sectional study answered questions from the past at the risk of remembering imperfectly. Parents may also have answered according to known social norms [Citation51], such as reportedly brushing their children’s teeth more frequently than they actually did or that their child did not eat candy or consume soft drinks as often as they did.
Conclusion
Approximately 80% of five-year-olds in Bergen, Norway presented with dental erosive wear. The habit of grinding teeth during the day and/or night and male sex significantly associated with those worst affected by dental erosive wear.
Supplementary_Table_S3.docx
Download MS Word (25.9 KB)Supplementary_Table_S2.docx
Download MS Word (22.7 KB)Supplementary_Table_S1.docx
Download MS Word (21 KB)Acknowledgements
The authors thank all dental hygienists who contributed as clinical examiners. The authors sincerely thank all the caregivers for their and their children’s participation in the study.
Disclosure statement
The authors report no conflict of interest.
References
- Carvalho TS, Colon P, Ganss C, et al. Consensus report of the European Federation of Conservative Dentistry: erosive tooth wear diagnosis and management. Swiss Dent J. 2016;126:342–346.
- Ganss C. Definition of erosion and links to tooth wear. Monogr Oral Sci. 2006;20:9–16.
- De Menezes Oliveira MA, Torres CP, Gomes-Silva JM, et al. Microstructure and mineral composition of dental enamel of permanent and deciduous teeth. Microsc Res Tech. 2010;73:572–577.
- Lussi A, Carvalho TS. Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2014;25:1–15.
- Scheutzel P. Etiology of dental erosion-intrinsic factors. Eur J Oral Sci. 1996;104:178–190.
- Zero DT. Etiology of dental erosion-extrinsic factors. Eur J Oral Sci. 1996;104:162–177.
- Barbour ME, Lussi A. Erosion in relation to nutrition and the environment. Monogr Oral Sci. 2014;25:143–154.
- Salas MM, Nascimento GG, Vargas-Ferreira F, et al. Diet influenced tooth erosion prevalence in children and adolescents: Results of a meta-analysis and meta-regression. J Dent. 2015;43:865–875.
- Schlueter N, Luka B. Erosive tooth wear - a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018;224:364–370.
- Kreulen CM, Van 't Spijker A, Rodriguez JM, et al. Systematic review of the prevalence of tooth wear in children and adolescents. Caries Res. 2010;44:151–159.
- Corica A, Caprioglio A. Meta-analysis of the prevalence of tooth wear in primary dentition. Eur J Paediatr Dent. 2014;15:385–388.
- Ganss C, Klimek J, Giese K. Dental erosion in children and adolescents–a cross-sectional and longitudinal investigation using study models. Commun Dent Oral Epidemiol. 2001;29:264–271.
- Carvalho TS, Lussi A, Jaeggi T, et al. Erosive tooth wear in children. Monogr Oral Sci. 2014;25:262–278.
- Grine FE. Enamel thickness of deciduous and permanent molars in modern Homo sapiens. Am J Phys Anthropol. 2005;126:14–31.
- Johansson AK, Sorvari R, Birkhed D, et al. Dental erosion in deciduous teeth-an in vivo and in vitro study. J Dent. 2001;29:333–340.
- Assuncao CM, Lussi A, Almeida Rodrigues J, et al. Efficacy of toothpastes in the prevention of erosive tooth wear in permanent and deciduous teeth. Clin Oral Invest. 2019;23:273–284.
- Hunter ML, West NX, Hughes JA, et al. Relative susceptibility of deciduous and permanent dental hard tissues to erosion by a low pH fruit drink in vitro. J Dent. 2000;28:265–270.
- Lippert F, Parker DM, Jandt KD. Susceptibility of deciduous and permanent enamel to dietary acid-induced erosion studied with atomic force microscopy nanoindentation. Eur J Oral Sci. 2004;112:61–66.
- Lussi A, Kohler N, Zero D, et al. A comparison of the erosive potential of different beverages in primary and permanent teeth using an in vitro model. Eur J Oral Sci. 2000;108:110–114.
- Jaeggi T, Lussi A. Prevalence, incidence and distribution of erosion. Monogr Oral Sci. 2014;25:55–73.
- Wiegand A, Muller J, Werner C, et al. Prevalence of erosive tooth wear and associated risk factors in 2-7-year-old German kindergarten children. Oral Dis. 2006;12:117–124.
- Gatou T, Mamai-Homata E. Tooth wear in the deciduous dentition of 5-7-year-old children: risk factors. Clin Oral Invest. 2012;16:923–933.
- Mantonanaki M, Koletsi-Kounari H, Mamai-Homata E, et al. Dental erosion prevalence and associated risk indicators among preschool children in Athens, Greece. Clin Oral Investig. 2013;17:585–593.
- Gatt G, Attard N. Erosive wear of the primary dentition: who is aware of it? Eur Arch Paediatr Dent. 2019;20:285–294.
- Tschammler C, Muller-Pflanz C, Attin T, et al. Prevalence and risk factors of erosive tooth wear in 3-6 year old German kindergarten children-A comparison between 2004/05 and 2014/15. J Dent. 2016;52:45–49.
- Sivertsen TB, Aßmus J, Greve G, et al. Oral health among children with congenital heart defects in Western Norway. Eur Arch Paediatr Dent. 2016;17:397–406.
- Mulic A, Tveit AB, Skaare AB. Prevalence and severity of dental erosive wear among a group of Norwegian 18-year-olds. Acta Odontol Scand. 2013;71:475–481.
- Mulic A, Fredriksen O, Jacobsen ID, et al. Dental erosion: Prevalence and severity among 16-year-old adolescents in Troms, Norway. Eur J Paediatr Dent. 2016;17:197–201.
- Sovik JB, Tveit AB, Storesund T, et al. Dental erosion: a widespread condition nowadays? A cross-sectional study among a group of adolescents in Norway. Acta Odontol Scand. 2014;72:523–529.
- Hasselkvist A, Johansson A, Johansson AK. Dental erosion and soft drink consumption in Swedish children and adolescents and the development of a simplified erosion partial recording system. Swed Dent J. 2010;34:187–195.
- Graue AM, Jokstad A, Assmus J, et al. Prevalence among adolescents in Bergen, Western Norway, of temporomandibular disorders according to the DC/TMD criteria and examination protocol. Acta Odontol Scand. 2016;74:449–455.
- Baggio S, Abarca M, Bodenmann P, et al. Early childhood caries in Switzerland: a marker of social inequalities. BMC Oral Health. 2015;15:82.
- Johansson AK, Johansson A, Birkhed D, et al. Dental erosion, soft-drink intake, and oral health in young Saudi men, and the development of a system for assessing erosive anterior tooth wear. Acta Odontol Scand. 1996;54:369–378.
- El Aidi H, Bronkhorst EM, Huysmans MC, et al. Multifactorial analysis of factors associated with the incidence and progression of erosive tooth wear. Caries Res. 2011;45:303–312.
- Dugmore CR, Rock WP. The progression of tooth erosion in a cohort of adolescents of mixed ethnicity. Int J Paediatr Dent. 2003;13:295–303.
- Dugmore CR, Rock WP. The prevalence of tooth erosion in 12-year-old children. Br Dent J. 2004;196:279–282.
- Truin GJ, van Rijkom HM, Mulder J, et al. Caries trends 1996-2002 among 6- and 12-year-old children and erosive wear prevalence among 12-year-old children in The Hague. Caries Res. 2005;39:2–8.
- Arnadottir IB, Holbrook WP, Eggertsson H, et al. Prevalence of dental erosion in children: a national survey. Community Dent Oral Epidemiol. 2010;38:521–526.
- Huang LL, Leishman S, Newman B, et al. Association of erosion with timing of detection and selected risk factors in primary dentition: a longitudinal study. Int J Paediatr Dent. 2015;25:165–173.
- Gurgel CV, Rios D, de Oliveira TM, et al. Risk factors for dental erosion in a group of 12- and 16-year-old Brazilian schoolchildren. Int J Paediatr Dent. 2011;21:50–57.
- Dugmore CR, Rock WP. Asthma and tooth erosion. Is there an association? Int J Paediatr Dent. 2003;13:417–424.
- Al-Dlaigan YH, Shaw L, Smith AJ. Is there a relationship between asthma and dental erosion? A case control study. Int J Paediatr Dent. 2002;12:189–200.
- Tolia V, Vandenplas Y. Systematic review: the extra-oesophageal symptoms of gastro-oesophageal reflux disease in children. Aliment Pharmacol Ther. 2009;29:258–272.
- Harding SM. Gastroesophageal reflux and asthma: insight into the association. J Allergy Clin Immunol. 1999;104:251–259.
- Johansson AK, Lingstrom P, Birkhed D. Comparison of factors potentially related to the occurrence of dental erosion in high- and low-erosion groups. Eur J Oral Sci. 2002;110:204–211.
- Mulic A, Skudutyte-Rysstad R, Tveit AB, et al. Risk indicators for dental erosive wear among 18-yr-old subjects in Oslo, Norway. Eur J Oral Sci. 2012;120:531–538.
- Sovik JB, Skudutyte-Rysstad R, Tveit AB, et al. Sour sweets and acidic beverage consumption are risk indicators for dental erosion. Caries Res. 2015;49:243–250.
- Statistics Norway [Internet]. Dental Health Care. Oslo (Norway): Statistics Norway; 2015–2019 [cited 2020 May 18]. Available from: https://www.ssb.no/statbank/sq/10035412
- Mulic A, Tveit AB, Wang NJ, et al. Reliability of two clinical scoring systems for dental erosive wear. Caries Res. 2010;44:294–299.
- Larsen MJ, Poulsen S, Hansen I. Erosion of the teeth: prevalence and distribution in a group of Danish school children. Eur J Paediatr Dent. 2005;6:44–47.
- Sjostrom O, Holst D. Validity of a questionnaire survey: response patterns in different subgroups and the effect of social desirability. Acta Odontol Scand. 2002;60:136–140.