
Abstract
Objective
The Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) is an instrument developed for assessment of orthodontic aspects of oral health-related quality of life (OHRQoL). This study aimed to translate and validate the Swedish version of PIDAQ for use in Swedish adolescents 12–19 years of age.
Material and methods
The translation was made according to the process described in ‘Guidelines for Establishing Cultural Equivalency of Instruments’ by Ohrbach et al. Field testing was performed in a group of consecutive patients who were about to start orthodontic treatment (untreated group) and a group of consecutive patients who had recently finished orthodontic treatment (treated group).
Results
During the translation procedure, a Swedish version of PIDAQ was formed. In the field testing, a total of 144 questionnaires, 72 from untreated patients (mean age 14.6 years) and 72 from treated patients (mean age 17.3 years) were collected. The exploratory factor analysis detected two factors, which differs from the factor structure in the original questionnaire. The mean total PIDAQ score was significantly higher (p < .001) in the untreated group, 40.6 (20.3), than in the treated group, 9.4 (10.5), implying a high discriminant validity. Reliability was excellent, with internal consistency Cronbach’s alpha values varying from 0.94 to 0.97.
Conclusion
The Swedish version of PIDAQ demonstrates good validity and excellent reliability and is suitable for future research on the effect of malocclusion on OHRQoL in Swedish 12- to 19-year-olds.
Introduction
Dental malocclusions are highly prevalent in children and adolescents. Approximately two-thirds of the adolescent population displays a malocclusion, and 30–40% of children are in need of orthodontic treatment [Citation1–3]. A malocclusion is not a disease, but rather a variation from a societal norm [Citation4]. The presence of a malocclusion occasionally leads to functional difficulties (chewing, biting) or damage to teeth, and sometimes leads to pain or discomfort. More frequently, malocclusions have psychological and/or social consequences – a negative affect on oral health-related quality of life (OHRQoL) [Citation5].
Patients opting to undertake orthodontic treatment expect improvement in appearance, self-image, and social functioning [Citation6]. There has been a growing acceptance that psychosocial benefits from orthodontic treatment in many cases are the most important treatment outcomes [Citation7,Citation8]. Still, most outcomes reported in orthodontic research do not reflect these values; rather, they seem to be focused more on the clinician’s view than on the patient’s view [Citation9]. In a systematic review published in 2014, it was concluded that OHRQoL was a reported outcome in only 9% of scientific orthodontic articles published between 2008 and 2013 [Citation10]. However, patient-reported outcome measures (PROM) such as OHRQoL are a growing research field.
The Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ) is an instrument specifically aimed at assessing orthodontic aspects of OHRQoL [Citation11]. The development of PIDAQ was based on a sample of university students 18–33 years of age and was first published in English in 2006 [Citation11]. Although PIDAQ was originally developed for young adults, it has been shown to be applicable also for adolescents aged 11–17 years after partial reformulation of items [Citation12].
PIDAQ has been translated into several languages and validated for use on adult populations [Citation13–21]. The original adult version of PIDAQ has also been translated and validated on children and adolescents [Citation22–26].
Translating and using existing foreign instruments has the advantage of making international comparisons possible. Translation procedures need to be rigorous to ensure not only a good translation but also a cross-cultural adaptation of the instrument. Until now, no Swedish translation of PIDAQ has been published. Since most orthodontic patients are adolescents, it seems reasonable to focus on this age group. Therefore, this study aimed to translate and validate the Swedish version of PIDAQ for use in Swedish adolescents 12- to 19-years of age.
Material and methods
Description of PIDAQ
The original version of PIDAQ has 23 items subdivided into four subscales: Dental Self-Confidence (6 items, questions 1–6), Social Impact (8 items, questions 7–14), Psychological Impact (6 items, questions 15–20), and Aesthetic Concern (3 items, questions 21–23). A five-point Likert scale ranging from 0 to 4 is provided. The response options are 0 = not at all, 1 = a little, 2 = somewhat, 3 = strongly, and 4 = very strongly. Since the first subscale (questions 1–6) is positively worded and subscales 2–4 (questions 7–23) negatively worded, the items of the first subscale are reversely scored to provide a consistent measure of the impacts [Citation11].
Formation of the Swedish version of PIDAQ
When applying a foreign instrument, it needs to be carefully translated, cross-culturally adapted, and validated. According to the COSMIN methodology, the three types of validity that needs to be evaluated in patient reported outcome measures, such as PIDAQ, are content validity, criterion validity, and construct validity [Citation27]. These measures are to be evaluated during different steps of the translation and validation process.
The translation of PIDAQ was performed according to the ‘Guidelines for Establishing Cultural Equivalency of Instruments’ [Citation28], which represent a synthesis of available literature and recommendations across multiple disciplines. The translation procedure was led by a team leader (E. G.). The translation followed the following stages.
Forward translation
PIDAQ was translated into Swedish by two translators who were fluent in English but whose first language was Swedish. After discussions with both translators, the team leader synthesized the two forward translations into a first draft.
Back translation
PIDAQ was back translated into English by two translators who were fluent in Swedish but whose first language was English. After discussions with both translators, the team leader synthesized the two back translations into one.
Independent review
The back translation was independently reviewed against the original source by a professional translator. When discrepancies between back translation and source were identified, recommendations for corrections were provided to the team leader. This process of review, recommendations, and evaluation by the team leader was followed by another cycle of translation and review until agreement was reached.
Expert panel review
An expert panel consisting of the team leader, two orthodontists, one researcher, one Swedish language teacher, and an adolescent reviewed the instrument with respect to the four types of equivalences: semantic, idiomatic, experiential, and conceptual. Content validity was assessed. The panel made recommendations for revision of the translation.
Pre-testing
Pre-testing was performed on a clinical sample of nine individuals 12–19 years of age with Swedish as their native language. Following administration of the instrument, the adolescents were interviewed individually regarding the intended meaning of the items versus their own understanding of the items. Possible translation alternatives were explored. Problematic items were identified. Content validity was assessed.
Instrument review
Items deemed problematic in the pre-test were reviewed by the team leader and further revised by members of the expert panel. To improve understandability of the questionnaire, it was agreed upon to add a brief instruction (two sentences) on how to fill in the questionnaire. Thereafter, the final version of the Swedish PIDAQ was developed.
Field testing
In the field-testing process, the Swedish version of PIDAQ was administered to 72 consecutive patients who were about to start orthodontic treatment (untreated group) and 72 consecutive patients who had recently finished orthodontic treatment (treated group). The samples were chosen to ensure two groups with the largest possible differences in the prevalence of malocclusion to allow for analysis of discriminant validity. All 144 participants were registered at the Center for Orthodontics and Pediatric Dentistry, County Council of Östergötland, Sweden. To reach 144 completed questionnaires, a total of 162 questionnaires were gathered. The 18 incomplete questionnaires were excluded from further analyses.
Exclusion criteria were intellectual and/or physical inability to answer the questionnaire; missing, fractured or severely discolored upper central incisors; cleft lip and palate; and ASA class III or higher [Citation29]. All individuals read and signed the terms of informed consent prior to participation. The study was approved by the Regional Ethical Board in Linköping, Sweden, 3 January 2017 (Dnr 2017/352-32). The questionnaires were collected May 2017–January 2018. The participants completed the questionnaire in a calm and silent environment in their orthodontic clinic. For test–retest analysis, 31 participants responded to the questionnaire a second time, within 2–8 weeks after the first time.
Intraoral photographs and radiographs were used when calculating objective orthodontic treatment need with the Index of Complexity Outcome and Need (ICON). ICON is an index ranging from 7 to 128. An ICON value ≥43 indicates orthodontic treatment need [Citation30]. Since the subjects were all registered patients at an orthodontic clinic, necessary photographs and radiographs to perform the ICON assessment already existed. Examinations were conducted by one investigator (EG), who had been previously trained and assessed in the use of the index. The ICON assessment was repeated on 49 subjects one month or more after the first assessment for intra-examiner calibration.
Statistics
SPSS® version 25 (SPSS® Inc., Chicago, IL) was used for statistical analysis.
Descriptive analyses – mean, median, standard deviation, PIDAQ scores for subscales and total scale scores – were calculated. The sample size calculation was based on the assumption that a difference of 2 PIDAQ scale scores between the two independent groups would be clinically relevant. The standard deviation of PIDAQ was assumed to be 4 scale scores. The level of significance was set to 5% and the power to 80%. The calculation resulted in a sample size of 63 patients in each group. To compensate for dropouts, at least 70 patients were planned to be enrolled in each group, giving a goal of a total of 140 subjects. Structural validity, an aspect of construct validity, was described by an exploratory factor analysis with principal components analysis and varimax rotation. Factor loadings of 0.5 were minimally accepted and the number of extracted dimensions was based on an Eigenvalue above 1 [Citation31]. Discriminant validity, being a dimension of construct validity, was evaluated by comparing PIDAQ differences between the untreated and treated groups as well as groups with and without orthodontic treatment need using T-test equal variances not assumed.
Criterion validity cannot be reported since no gold standard exists for PROM (Patient Related Outcome Measures) [Citation32]. Internal consistency was tested using Cronbach’s alpha coefficient. Alpha values of ≥0.70 were considered adequate [Citation33]. Cronbach ‘alpha if item deleted’ was performed to further test internal consistency. Test–retest reliability of the PIDAQ questionnaire was assessed using the Intraclass correlation coefficient (ICC) with a two-way random effects and consistency model for the PIDAQ score. An ICC > 0.75 represented excellent reliability, an ICC between 0.60 and 0.75 good, 0.40–0.59 fair, and < 0.40 poor reliability [Citation34]. Test–retest of the ICON assignments 1 and 2 was assessed using Spearman’s rho. A value of ≥0.8 indicates very strong agreement, ≥0.6 up to <0.8 moderately strong, ≥0.3 up to<0.6 fair and <0.3 fair agreement [Citation35]. Spearman’s rho showed a correlation of 0.92 between ICON assignment one and two of the 49 individuals who were judged twice to calculate for intra-examiner reliability, indicating a very strong agreement. The level of significance was set to 5%.
Results
Cross-cultural adaptation
In the content validity assessment, all items of the original instruments were deemed relevant and pertinent to the Swedish context. During the rigorous translation procedure, a Swedish version of PIDAQ was formed.
Descriptive data
The mean (SD) age of all the 144 (57 male, 87 female) participants was 16.0 (2.1) years. The untreated group consisted of 72 (28 male, 44 female) adolescents aged 16.6 (1.7) years. The treated group of 72 (29 M, 43 F) individuals was significantly (p ˂ .001) older with a mean age of 17.3 (1.5) years. The mean (SD) ICON score was 55.3 (16.5) in the untreated group and 12.2 (5.2) in the treated group (p ˂ .001).
Validity
Structural validity is a dimension of construct validity and refers to how items are related to one another. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.94, and the Bartlett’s test of sphericity was significant (p ˂ .001). The exploratory factor analysis detected two factors with an Eigen value of greater than 1.0; Dental Aesthetic Self-Confidence (12 items, Q 1–7, 18, and 20–23) and Psychosocial Impact (11 items, Q 8–17 and 19) (). These two domains explained 72% of the total variance.
Table 1. Factor loadings of items after exploratory factor analysis and Cronbach α if item deleted from assigned factor.
Another subscale of construct validity is discriminant validity. It was described by the mean (SD) PIDAQ scores being 40.6 (20.3) in the untreated group and 9.4 (10.5) in the treated group (p ˂ .001) (). The differences in PIDAQ scores between the two groups were significant for the subscales and for the total scale, indicating a high discriminant validity (). illustrates the distribution of PIDAQ scores in the untreated and treated groups.
Figure 1. Box plot of individual PIDAQ scores of the 72 individuals in the untreated group and the 72 individuals in the treated group. Min score 0, max score 92.
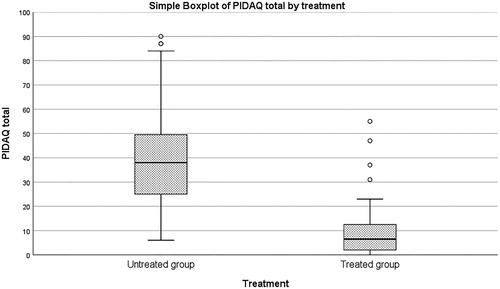
Table 2. Discriminant validity – difference between untreated and treated groups – for subscales and total scale.
When differences between sexes in the untreated group were analyzed, the 44 females had significantly (p ˂ .001) higher PIDAQ total scores of 48.5 (20.3) than the 28.1 (12.8) found among the 28 males. In the treated group, differences in PIDAQ scores between sexes were not significant.
The participants were also subdivided into groups with and without orthodontic treatment need, respectively. Fifty-six individuals had ICON ≥43, indicating orthodontic treatment need. Eighty-eight individuals had ICON <43, indicating no orthodontic treatment need. All of the individuals with treatment need were in the untreated group. A total of 16 of the individuals in the untreated group had ICON <43, despite being on a waiting list to begin orthodontic treatment. The mean (SD) PIDAQ scores was 40.1 (19.4) in the treatment need group and 15.4 (18.7) in the no treatment need group, which was significantly different (p ˂ .001) indicating a high discriminant validity ().
Table 3. Discriminant validity – difference between individuals with and without orthodontic treatment need – for subscales and total scale.
Reliability
Internal consistency was excellent, with Cronbach’s alpha values of 0.94 and 0.97 for the subscales and 0.97 for the total scale (). The ‘Alpha if item deleted’ showed that when an item was removed from PIDAQ analysis, the Cronbach Alpha did not significantly increase (), also indicating a good internal consistency.
Table 4. Reliability statistics.
Test–retest analysis was based on 31 individuals responding a second time to the questionnaire. The ICC value for the test–retest reliability analysis was 0.95 for the total scale, indicating excellent reliability ().
Table 5. Reliability statistics.
Discussion
In the translation process, guidelines published by the International Research Diagnostic Criteria for Temporomandibular Disorders RCD/TMD Consortium Network, ‘Guidelines for Establishing Cultural Equivalency of Instruments’, were used. These guidelines are based on standards for valid document translation. The guidelines were originally developed to translate the RDC/TMD questionnaire, but since they represents a synthesis of available literature and recommendations across multiple disciplines, they can be applied to any instrument used across linguistic or cultural boundaries [Citation28].
In this study, the original version of PIDAQ [Citation11] was translated. The original version was developed based on a sample of young adults 18–30 years of age of which 70% had already had orthodontic treatment [Citation11]. A few years later the same research group published results on PIDAQ validity and reliability across three age groups (11–12, 13–14, and 15–17 year–olds) [Citation12]. In that study, the children and adolescents answered the same 23 items as were present in the original PIDAQ version; however, some of the items were partially reformulated. The reformulation took place after an expert panel consisting of one school psychologist and three orthodontists ‘experienced in children’s talk about their teeth’ evaluated the items and suggested changes. Thereafter, the modified items were tested on 36 orthodontic patients 11–15 years of age. The results of the study were that PIDAQ demonstrated good psychometric properties in adolescents across age groups [Citation12]. In the present study, the original PIDAQ was used as the source, even though the target population was adolescents, not young adults. The reasons for this were that (1) the original PIDAQ version is the one that has been used internationally as the source in previous translation procedures; (2) the applied changes in the youth version of PIDAQ were minor; and (3) in the translation procedure care was taken to adapt the Swedish language to be suitable for use on children and adolescents, even though the adult PIDAQ version was used as source. However, the fact that PIDAQ was developed on young adults of which 70% had already had orthodontic treatment [Citation11] is a potential weakness when PIDAQ is used on adolescents with malocclusions. Future research on the instrument may contain cognitive interviews to confirm applicability of the instrument.
It was decided to keep the original items, since they all were deemed valid for use in a Swedish population. However, a brief written instruction on how to fill in the questionnaire was added to the PIDAQ questionnaire to assist the patients. The brief instruction is in Swedish. Translated into English, the instruction is worded, ‘Below are statements on what you think about your teeth and how that affects how you feel. Please mark with an (x) how much you agree with the statements, from “0 = not at all” to “4 = very strongly”’.
The exploratory factor analysis showed that the Swedish version consists of two dimensions with an Eigen value of greater than 1 (). We named the two dimensions ‘Dental Aesthetic Self-Confidence’ (12 items, Q1–7, 18, and 20–23) and ‘Psychosocial Impact’ (11 items, Q 8–17 and 19). The original PIDAQ version consisted of four dimensions [Citation11], just as the majority of the other translations [Citation12,Citation14,Citation19–22,Citation24]. However, several other translations also have shown a different factor structure than the original PIDAQ version. Two translations have found that the instrument has three dimensions [Citation17,Citation23], and one translation revealed five dimensions [Citation15]. Finally, there are a few translations which have not included factor analysis in their validation [Citation13,Citation16,Citation25]. It can be concluded that PIDAQ seems to display different factor structures in different translations and populations. However, a flaw of the current study is that the sample size was rather small for exploratory as well as confirmatory factor analysis. Further studies with new and bigger samples would make a confirmatory factor analysis possible. No confirmatory factor analysis was performed in the present study since the sample size was rather small and the same data set should not be used for exploratory and confirmatory factor analysis [Citation36] .
Worth to consider is that two items 15 and 21 loaded almost equally high in both factor 1 and 2. Item 15 (‘I envy the nice teeth of other people’) was included in factor 2, and item 21 (‘I don’t like to see my teeth in the mirror’) was included in factor 1. The reason for this was that the items loaded slightly higher in the mentioned dimensions.
An aspect of reliability is the correlation among items called internal consistency. This measure is aimed at reflecting whether included items measure the same phenomenon. The Cronbach’s alpha of the subscales were 0.97 and 0.94, and the value for the total scale was 0.97, indicating excellent reliability. In the original PIDAQ study, Cronbach’s alpha values ranged between 0.85 and 0.91 for the different subscales [Citation11].
Another reliability aspect is the temporal stability measure test–retest reliability. The value ranged between 0.86 and 0.88 for the subscales and was 0.90 for the total scale. ICC values are considered excellent if greater than 0.74 [Citation37]. In the original PIDAQ article, no test–retest analysis was performed. For comparison, test–retest values presented in the Brazilian version of PIDAQ ranged between 0.89 and 0.99 between their four subscales [Citation16], and between 0.93 and 0.97 in the Italian adolescent version [Citation23]. However, in the present study, we had a smaller sample size (142 individuals) and a smaller test–retest sample (31 individuals) than in the other two studies, which must be kept in mind when interpreting the results.
In the present study, ICON was used for measuring severity of malocclusion/orthodontic treatment need. In the original PIDAQ study [Citation11], self-reported aesthetic component (IOTN AC) and perception of occlusion as well as interviewer-rated aesthetic component (IOTN AC) [Citation38] and a modified version of Dental Aesthetic Index (DAIM) [Citation39] were instead used [Citation11]. The reason for our choice of ICON were that it is possible to judge ICON based on clinical photographs and radiographs, which is the method used in this study. Also, the ICON index subdivides individuals in two groups; ICON value ≥43 indicates orthodontic treatment need and 42 or less no need for treatment [Citation30]. This subdivision was useful since we wanted to see if PIDAQ values differed in groups with and without orthodontic treatment need. Yet another reason for our choice of the ICON index was that with ICON, it is possible to calculate the treatment results by measurements before and after orthodontic treatment [Citation30]. We are planning to use this tool in future studies.
Orthodontic treatment during childhood or adolescence has been shown to improve OHRQoL, but the evidence is of low and moderate quality [Citation40]. Therefore, more high-quality, longitudinal, and prospective studies are needed. Our present study cannot show that orthodontic treatment improves OHRQoL, as the study was not longitudinal. Also, the treated and untreated groups differed significantly in age which makes conclusions on differences between groups based on the prevalence of malocclusion more problematic. Further, the responsiveness of PIDAQ – it’s ability to detect changes over time [Citation27] – has not been evaluated. However, our newly developed Swedish version of the PIDAQ can be used in future research such as longitudinal and prospective studies assessing OHRQoL before and after orthodontic treatment. This could improve our knowledge of the responsiveness of the instrument, as well as our knowledge of the effect of malocclusions and orthodontic treatment on OHRQoL.
Conclusions
The Swedish version of PIDAQ demonstrates good validity and excellent reliability and is suitable for future research on the effect of malocclusion on OHRQoL in Swedish 12- to 19-year-olds.
Acknowledgments
Preliminary results of this study were presented as a poster and published as a conference abstract at the 94th European Orthodontic Society (EOS) Congress in Edinburgh. The authors gratefully acknowledge the contribution of the orthodontic patients, orthodontic assistants, and orthodontists who took part in this study.
Disclosure statement
No conflict of interest to declare.
References
- Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81(1):12–21.
- Helm S. Malocclusion in Danish children with adolescent dentition: an epidemiologic study. Am J Orthod. 1968;54(5):352–366.
- Helm S, Kreiborg S, Barlebo J, et al. Estimates of orthodontic treatment need in Danish schoolchildren. Commun Dent Oral Epidemiol. 1975;3(3):136–142.
- Shaw WC, O'Brien KD, Richmond S, et al. Quality control in orthodontics: risk/benefit considerations. Br Dent J. 1991;170(1):33–37.
- Dimberg L, Arnrup K, Bondemark L. The impact of malocclusion on the quality of life among children and adolescents: a systematic review of quantitative studies. Eur J Orthod. 2015;37(3):238–247.
- Trulsson U, Strandmark M, Mohlin B, et al. A qualitative study of teenagers' decisions to undergo orthodontic treatment with fixed appliance. J Orthod. 2002;29(3):197–204.
- Cunningham SJ, Hunt NP. Quality of life and its importance in orthodontics. J Orthod. 2001;28(2):152–158.
- Hunt O, Hepper P, Johnston C, et al. Professional perceptions of the benefits of orthodontic treatment. Eur J Orthod. 2001;23(3):315–323.
- ÓBrien K. Orthodontic research: If we know the answers, are we asking the right questions?. Semin Orthod. 2013;19:137–141.
- Tsichlaki A, O'Brien K. Do orthodontic research outcomes reflect patient values? A systematic review of randomized controlled trials involving children. Am J Orthod Dentofacial Orthop. 2014;146(3):279–285.
- Klages U, Claus N, Wehrbein H, et al. Development of a questionnaire for assessment of the psychosocial impact of dental aesthetics in young adults. Eur J Orthod. 2006;28(2):103–111.
- Klages U, Erbe C, Sandru SD, et al. Psychosocial impact of dental aesthetics in adolescence: validity and reliability of a questionnaire across age-groups. Qual Life Res. 2015;24(2):379–390.
- Bourzgui F, Serhier Z, Sebbar M, et al. Adaptation and validation of the Moroccan Arabic version of the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ). Saudi Dent J. 2015;27(4):180–186.
- Bucci R, Rongo R, Zito E, et al. Cross-cultural adaptation and validation of the Italian Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ). Qual Life Res. 2015;24(3):747–752.
- Singh VP, Singh R. Translation and validation of a Nepalese version of the Psychosocial Impact of Dental Aesthetic Questionnaire (PIDAQ). J Orthod. 2014;41(1):6–12.
- Sardenberg F, Oliveira AC, Paiva SM, et al. Validity and reliability of the Brazilian version of the psychosocial impact of dental aesthetics questionnaire. Eur J Orthod. 2011;33(3):270–275.
- Lin H, Quan C, Guo C, et al. Translation and validation of the Chinese version of the psychosocial impact of dental aesthetics questionnaire. Eur J Orthod. 2013;35(3):354–360.
- Ngom PI, Attebi P, Diouf JS, et al. Translation and cultural adaptation of a French version of the psychosocial impact of dental aesthetics questionnaire: PIDAQ. Orthod Fr. 2013;84(4):319–331.
- Spalj S, Lajnert V, Ivankovic L. The psychosocial impact of dental aesthetics questionnaire – translation and cross-cultural validation in Croatia. Qual Life Res. 2014;23(4):1267–1271.
- Aglarci C, Baysal A, Demirci K, et al. Translation and validation of the Turkish version of the Psychosocial Impact of Dental Aesthetics Questionnaire. Korean J Orthod. 2016;46(4):220–227.
- Naseri N, Baherimoghadam T, Rasooli R, et al. Validity and reliability of the Persian version of the psychosocial impact of dental aesthetics questionnaire. Health Qual Life Outcomes. 2019;17(1):126
- Montiel-Company J-M, Bellot-Arcís C, Almerich-Silla J-M. Validation of the psychosocial impact of dental aesthetics questionnaire (Pidaq) in Spanish adolescents. Med Oral Patol Oral Cir Bucal. 2013;18(1):e168–e173.
- Bucci R, Rongo R, Zito E, et al. V. Translation and validation of the italian version of the Psychosocial Impact of Dental Aesthetics Questionnaire (pidaq) among adolescents. Eur J Paediatr Dent. 2017;18:158–162.
- Wan Hassan WN, Yusof ZY, Makhbul MZ, et al. Validation and reliability of the Malaysian English version of the psychosocial impact of dental aesthetics questionnaire for adolescents. Health Qual Life Outcomes. 2017;15(1):54.
- Santos PM, Goncalves AR, Marega T. Validity of the Psychosocial Impact of Dental Aesthetics Questionnaire for use on Brazilian adolescents. Dental Press J Orthod. 2016;21(3):67–72.
- Ilijazi-Shahiqi D, Mehmeti B, Kelmendi J, et al. Validity and reliability of the Psychosocial Impact of Dental Aesthetics Questionnaire in Kosovar adolescents. Int J Adolesc Med Health. 2020. DOI:10.1515/ijamh-2019-0038
- Terwee CB, Prinsen CAC, Chiarotto A, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27(5):1159–1170.
- Ohrbach Rb J, Jezewski M, John MT, et al. Guidelines for Establishing Cultural Equivalency of Instruments. 2013 [cited 2020 Jun 25]. Available from: URL. http://www.rdc-tmdinternational.org
- Anesthesiologists ASo. ASA Physical Status Classification System; 2014.
- Daniels C, Richmond S. The development of the index of complexity, outcome and need (ICON). J Orthod. 2000;27(2):149–162.
- Hair JF, William CB, Jr, Babin BJ, et al. Multivariated data analysis, 4th ed. London: Pearson Education Limited; 2014.
- Mokkink LB, Prinsen CAC, Patrick DL, et al. COSMIN Study Design checklist for Patient-reported outcome measurement instruments; 2019; [cited 2020 Jun 25]. Available from: www.cosmin.nl
- Streiner DL. Starting at the beginning: an introduction to coefficient alpha and internal consistency. J Pers Assess. 2003;80(1):99–103.
- Fleiss J. The design and analysis of clinical experiments. New York (NY): Wiley & Sons; 1986.
- Chan YH. Biostatistics 104: Correlational analysis. Singapore Med J. 2003;44(12):614–619.
- Harrington D. Confirmatory Factor Analysis; Pocket Guide to Social Work Research Methods. New York: Oxford University Press; 2008.
- Nunnally JCB, IR. Psychometric theory. New York: McGraw-Hill; 1994.
- Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11(3):309–320.
- Cons NC, Jenny J, Kohout FJ. DAI: The Dental Aesthetic Index. Iowa City: Iowa City College of Dentistry, University of Iowa; 1986.
- Javidi H, Vettore M, Benson PE. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis . Am J Orthod Dentofacial Orthop. 2017;151(4):644–655.