
Abstract
Objectives
To assess if and to what extent public dental health personnel (PDHP) receive inquiries from child welfare services (CWS), and to assess whether PDHP’s experience of receiving inquiries is associated with PDHP’s characteristics and whether the associations are influenced by PDHP’s experience of reporting to CWS.
Material and methods
Questionnaires were distributed to 1542 PDHP in Norway. Descriptive statistics were used for analysis. Negative-binominal-regression analyses with incidence rate ratios (IRRs) and confidence intervals (CIs) were used to estimate the association between received inquiries from CWS and PDHP characteristics.
Results
From a total of 1074 respondents, 52.4% had received inquiries from CWS (2012–2014) with a mean number of 3.9 (SD = 4.5). PDHP’s likelihood of receiving inquiries was significantly associated with having many patients, working in small municipalities, working in eastern Norway, having good knowledge of the Health Personnel Act, and having experience reporting to CWS. Regional differences were the only association that varied according to PDHP reporting activity.
Conclusions
PDHP receive inquiries from the CWS. The likelihood of receiving inquiries is associated with several characteristics of PDHP. To increase PDHP’s likelihood of receiving inquiries, it is important to establish contact between the CWS and PDHS and ensure that the PDHP has good knowledge of the Health Personnel Act.
Introduction
Child maltreatment can have severe and lifelong impacts on a child’s physical and mental development [Citation1,Citation2]. In Norway, child welfare services (CWSs) are obliged to help and safeguard children at risk [Citation3]. Hence, decisions made by child welfare professionals can have a major impact on a child, the child’s family, and society, both in the short and long terms [Citation4,Citation5]. To be well-founded and correct, each decision made by CWS must be built upon relevant and available documentation.
According to the Norwegian Child Welfare Act [Citation3], when the CWS receives a report of concern, they are obliged to screen the report and decide whether it is reasonable to start an investigation. If an investigation is warranted, CWS can gather additional information concerning the child under investigation [Citation3]. Such information can be acquired from different instances that can hold information relevant to the investigation, such as the child’s educational institutions and/or health services [Citation6]. A report from Norway indicated that CWS in Norway inquired information from different services, with a mean of 2.6 inquiries per investigation [Citation6]. If public dental health personnel (PDHP) receive an inquiry from the CWS regarding one of their patients, they are mandated by the Health Personnel Act and the Child Welfare Act to provide the requested information to the CWS [Citation3,Citation7].
Children’s oral health status, together with their dental attendance history, might indicate the child’s overall care situation. This is especially true in countries such as Norway, Sweden, Finland, and Denmark, where all children receive free dental services regularly at public dental health services [Citation8,Citation9]. All children are dependent on their caregivers to maintain good oral health. This dependency relates to both oral hygiene habits, diet, and being taken to dental appointments when they are summoned or if they need oral treatment due to pain [Citation10–13]. Research has shown that abused and neglected children have an increased risk of having untreated caries, a reluctance to seek dental treatment when needed, and a history of missed dental appointments [Citation10,Citation14–16]. Furthermore, victims of neglect and physical or sexual abuse (in particular abuse involving the oral cavity) have an increased likelihood of experiencing fear or anxiety related to receiving oral treatment [Citation17–21]. Hence, poor oral health, severe untreated caries, and/or a history of not showing up to dental appointments can indicate child maltreatment. This is conditioned on no medical, financial, or other known reason for the child’s impaired oral situation [Citation14,Citation15,Citation22]. Children’s dental health records can be important for CWS, as they can hold important information regarding children’s health and living conditions.
Altogether, CWS must be aware of the association between child abuse and neglect and oral health [Citation16]. There is reason to believe that sharing relevant information between the CWS and the public dental health service (PDHS) can be of great importance for at-risk children, both in terms of detecting abuse or neglect and identifying and treating children with oral health needs [Citation16]. Hence, it is central that CWS are aware that a child’s dental records can be of importance and utilize their right to gather additional information from the PDHS. Several studies worldwide have assessed whether dental health personnel reports their concern to CWS and why they report or fail to report [Citation16,Citation19,Citation23–25]. In contrast, there is a lack of studies assessing whether and to what extent dental health personnel receives inquiries from CWS in terms of being asked to provide information from the dental records of children under their investigation [Citation25].
The aim of this study was two fold:
Investigate if and to what extent PDHP receives inquiries from the CWS.
Investigate whether PDHP’s experience of receiving inquiries is associated with personal, behavioural, organizational, and external characteristics and whether those associations are influenced by PDHP’s experience of reporting to CWS.
Material and methods
Survey
This article is one of several published papers based on a national, cross-sectional study conducted in 2014, including a census of dentists and dental hygienists employed in the PDHS in Norway [Citation23,Citation24,Citation26,Citation27]. In the survey, the PDHP in 18 out of 19 counties in Norway was included. The excluded county was used to pilot the survey. The Regional Ethics Committee (REK) concluded that approval for the study from REK was not needed. The Norwegian Centre for Research Data (NSD) registered and ratified the study in 2014. Furthermore, the NSD distributed the survey and collected the data. A total of 1542 public dentists and dental hygienists received a cover letter and an electronic self-administered questionnaire containing an informed consent form. The questionnaire was distributed in November 2014. Non-responders received up to three reminders. The questionnaire had an estimated completion time of 30–40 min. Dental personnel were given permission to answer the questionnaire during their working hours. For additional information, see Brattabø et al. [Citation23].
Dependent variable
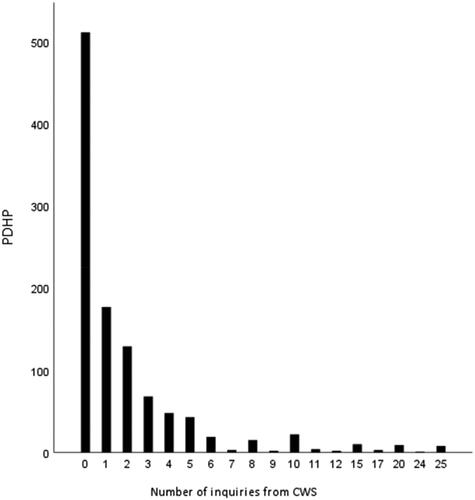
The respondents were asked whether they had received inquiries from the CWS within three years (2012–2014) and to list the number of inquiries they had received. Respondents who had not received inquiries were registered with 0 inquiries. The reported number of inquiries from the CWS regarding patients under investigation was set as the dependent variable (see ).
Figure 1. Distribution of inquiries received by public dental health personnel (PDHP) from child welfare services (CWS) in the 3-year period 2012–2014.
Independent variables
The independent variables pertained to the PDHP’s personal, organizational, external, and behavioural characteristics. For ease of readability, several independent variables were recoded into fewer categories. Personal characteristics included gender (male or female), age (20–39 or 40+ years; recoded from 20 to 29, 30–39, 40–49, 50–59, 60–69, and 70 + years), education (dentist or dental hygienist), and work experience (0–10 or 11+ years; recoded from being numerical). Organizational characteristics consisted of the number of patients examined during the last 12 months (0–500 or 501+ patients; recoded from 0–250, 251–500, 501–750, 751–1000, 1001–1250, 1251–1500, and 1501 + patients). External characteristics were measured in terms of the size of the municipality where the dental clinic is located (0–10,000, 10,001–40,000, or 40,001+ inhabitants; recoded from 0–5000, 5001–10,000, 10,001–15,000, 15,001–20,000, 20,001–40,000, 40,001–80,000, and 80,001 + inhabitants) and geographical region (north, central, west, south, or east; recoded from the 18 counties). Behavioural characteristics were measured in terms of knowledge of the Health Personnel Act and which information should be given to CWS upon inquiry (sure, neither/nor, and unsure; recoded from very unsure, unsure, neither unsure/nor sure, sure, very sure) and the respondent’s own experience with sending a report of concern to CWS (experienced or unexperienced reporter).
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0, IBM Corp., Armonk, NY), and descriptive statistics were calculated in terms of frequencies for categorical variables and mean (with standard deviations, SD) for continuous variables. To identify how the PDHP’s experience of receiving inquiries from CWS varies according to the characteristics of the PDHP, each independent variable was compared with the dependent variable using negative binomial regression analysis (with a log-link function). The results are presented as incidence rate ratios (IRRs) with 95% confidence intervals (CIs). To assess whether the association of each independent variable with PDHP’s experience of receiving inquiries from CWS varied according to the PDHP’s reporting experience, the analysis was stratified based on reporting experience (no experience versus >0 experience). A joint model with an interaction term for each of the independent variables and reporting experience was used to test if there was a significant difference in the associations between experienced and non-experienced PDHP. For all analyses, p < .05, were considered statistically significant. Cases with missing data were excluded from analyses.
Results
Of the 1542 dentists and dental hygienists who received the electronic questionnaire, 1200 (77.8%) responded. However, due to missing responses on variables, 1074 replied to the questions on inquiries from the CWS within 3 years 2011–2014.
Of the 1074 respondents, 52.4% (563/1074) had received an inquiry in the previous 3 years (>0), with a mean of 3.9 (SD = 4.5) while 47.6% (511/1074) did not receive an inquiry (=0) (not tabulated). The number of inquiries from the CWS ranged from 0 to 25 ().
displays the distribution of the respondents’ characteristics in total, the mean number of inquiries from CWS according to PDHP characteristics, organized by PDHP personal, organizational, external, and behavioural characteristics. Owing to missing data, N differs between 1074 and 1067 for different characteristics. The characteristics of the respondents are in accordance with the distribution in the PDHS in Norway: 80.2% were females, 46.3% were 40 years of age or older, and 69.9% were dentists. The mean number of inquiries for all 1074 respondents was 2.06 (SD = 3.8) ().
Table 1. Distribution of PDHP and mean (SD) number of inquiries by characteristics.
Concerning PDHP's knowledge of the Health Personnel Act and which information should be given to CWS upon an inquiry from CWS, 55.8% reported that they were sure, 16.0% reported that they were neither sure nor unsure, and 28.2% reported that they were unsure. Those who were sure had a mean of 2.76 (SD = 4.3) inquiries from CWS. The corresponding number for those who were neither sure nor unsure was 1.53 (SD = 3.7), while for the unsure, the mean was 0.98 (SD = 2.1). The majority of respondents were experienced reporters, with 59.1% had reported suspicion of child abuse or neglect to CWS ().
The adjusted analyses in indicate that the PDHP’s experiences with receiving inquiries from the CWS during 2012–2014 were associated with PDHP’s personal, organizational, external, and behavioural characteristics. Females in the PDHS had an increased likelihood (IRR = 1.38, 95% CI: 1.05–1.82) of receiving inquiries from CWS compared to males. PDHP working in municipalities with 10,000 or fewer inhabitants had an increased likelihood of receiving inquiries from CWS (IRR = 1.42, 95% CI: 1.10–1.84) compared to PDHP working in municipalities with more than 40,000 inhabitants. The likelihood of receiving an inquiry from CWS increased in line with the PDHP’s level of knowledge of the Health Personnel Act and the kind of information that could be shared with CWS. Compared to those who reported being unsure of the Health Personnel Act, both those who reported being neither sure nor unsure (IRR = 1.64, 95% CI: 1.19–2.26) and those who were sure (IRR = 2.63, 95% CI: 2.06–3.37) had an increased likelihood of receiving an inquiry. Moreover, compared to non-experienced reporters, PDHP who had experienced reporting suspected child abuse or neglect to CWS had an increased likelihood of receiving an inquiry from CWS (IRR = 1.32, 95% CI: 1.07–1.61) ().
Table 2. Negative binominal regression analysis.
depicts the unadjusted and adjusted negative binomial regression analysis for IRRs receiving inquiries from CWS by PDHP characteristics, separately for experienced and non-experienced reporters, and a joint model for differences between experienced and non-experienced reporters. As shown in , the unadjusted analysis and the joint model showed significant differences between experienced and non-experienced reporters in the IRRs for receiving inquiries according to PDHP’s age, working experience, number of patients in the last 12 months, and region. The corresponding IRRs were (IRR = 1.90 95% CI: 1.25–2.90), (IRR = 1.61 95% CI: 1.05–2.4), (IRR = 1.53 95% CI: 1.00–2.36) and (IRR = 2.62 95% CI: 1.34–5.13). For the adjusted analysis, the joint model showed a significant difference between the experienced and non-experienced reporters regarding region only, with an IRR of 2.08 (95% CI 1.06–4.06.)
Table 3. Negative binominal regression analysis stratified by DPHP reporting experience and a joint model testing difference in number of inquiries from CWS.
Discussion
There is a dearth of research assessing whether and to what extent dental health personnel receives inquiries from CWS asking for information from children’s dental records. The findings of the present study show that the PDHP in Norway is used as informants by the CWS. About half of the respondents working in all regions of Norway reported having received inquiries from CWS in 2012–2014. This suggests that the CWS in Norway is aware that children’s dental records can contribute to the understanding of a child’s health and living conditions. Our findings indicate that the likelihood of receiving inquiries from CWS is significantly associated with PDHP’s personnel characteristics in terms of gender, behavioural characteristics in terms of knowledge of the Health Personnel Act and previous reporting experience, organizational characteristics in terms of the number of patients, and external characteristics in terms of size of the municipality and region. In addition, regional inequality in PDHP receipts of inquiries varies according to their reporting experience.
This study had several strengths and limitations. The study is national and includes a census of public dentists and dental hygienists in Norway. This, together with the high response rate and the fact that the demographic distribution of the respondents was in line with the corresponding distribution of the census of PDHS in Norway, implies that the study has high external validity. For self-report studies, there is always a risk of bias due to recall and social desirability. Nevertheless, receiving inquiries from CWS entails an important job for the PDHP, which is relatively easy to recall. The present findings show that the majority of PDHPs have not received frequent inquiries from CWS. Hence, it is reasonable to assume that remembering the number of inquiries during the past three years is less demanding. In the present study, the respondents were asked about their knowledge of the Health Personnel Act [Citation7] and information they may give CWS when an inquiry is received. PDHPs should be familiar with the Act; therefore, admitting uncertainty or lack of knowledge might be challenging. Hence, there is a risk that some of the responses to this question are influenced by social desirability. However, 28.2% of the respondents reported being unsure of the act and 16.0% reported being neither sure nor unsure shows that respondents admitted their uncertainty.
It is evident that the PDHPs in Norway are experienced reporters of CWS and suspect different forms of child maltreatment, including neglect, physical, psychological, and sexual abuse [Citation26]. The present findings reveal that more than half of the investigated PDHP received inquiries from the CWS, with a mean number of close to four inquiries. The PDHP who are experienced reporters to the CWS themselves were more likely to receive inquiries from CWS than non-experienced reporters. This finding indicates that contact between the CWS and PDHP increases the likelihood of further collaboration. Perhaps CWS awareness and understanding concerning the importance of children’s oral health increases according to the number of received reports of concern from the PDHP.
Previous research from Norway has shown that PDHPs working in large municipalities are more likely to send reports of concern to CWS than those working in smaller municipalities [Citation23]. Hence, it is interesting that the present findings show the opposite trend in terms of PDHP receiving inquiries from the CWS. Thus, the likelihood of receiving inquires was higher for PDHP working in smaller municipalities than for PDHP working in larger municipalities. One reason for this finding can be that different services are more familiar with one another in smaller municipalities than in larger municipalities. Hence, it might be easier for CWS to inquire about information in small municipalities, as it is easier to know which public dental health clinics need to be addressed. Another reason might be that CWS in small municipalities has closer collaboration with PDHS, are familiar with people working there, and are perhaps more aware of which information can be found in a child’s dental records. To conclude, further research is needed.
While PDHP from all parts of Norway received inquiries from the CWS, there were regional differences. Participants from the central, western, southern, and northern regions in Norway were all less likely to receive inquiries from the CWS than their counterparts in the eastern region. When testing for differences between PDHP with and without reporting experience, it was only the characteristic region that showed significant differences between the two groups. Compared to the eastern region, the northern region was less likely to receive inquiries independent of the PDHP as an experienced reporter. However, this relationship was significantly weaker among non-experienced than experienced PDHPs. These findings may be influenced by the demographics in the northern region, which differs from the rest of Norway by having many rural and sparsely populated areas with large distances in between. To our knowledge, only one previous study has assessed whether dental health personnel receives inquiries from the CWS [Citation25]. A study conducted among PDHPs working in Norway’s capital Oslo found that 90% of the dental health personnel investigated had been requested to send information to the CWS during a 5-year period [Citation25]. Our findings with PDHP in the eastern region (including Oslo), which has the highest likelihood of receiving inquiries, support the results of that study. The increased likelihood of receiving inquiries in the eastern region might reflect the challenges associated with socioeconomic and cultural diversity in a big city like Oslo. According to a study among Norwegian youth, there are more challenges with crime, cannabis abuse, school skipping, and violence among youth in Oslo than youths living in other parts of Norway [Citation28].
The present findings indicate that the Health Personnel Act can be challenging for PDHP [Citation7], with about half of the participants being neither sure nor unsure about its content. PDHPs who were sure of the act were more likely to receive inquiries from CWS than their counterparts who were unsure or very unsure. These findings were consistent for both experienced and inexperienced reporters, indicating the importance of securing PDHP’s knowledgeability and confidence of the Health Personnel Act. Alternatively, it might also be that the PDHP’s knowledge of the Health Personnel Act [Citation7] is influenced by their experience of receiving inquiries from the CWS. Further research is needed to understand these mechanisms.
Previous research from our research group has revealed that PDHP does detect child maltreatment, as one-fourth of the reports of concern from the PDHS in Norway have led to measures by CWS [Citation26]. In addition, empirical evidence shows an associative relationship between child maltreatment and poor oral health [Citation16]. It is reasonable to assume that by inquiring information from the PDHS, CWS can increase their ability to make decisions based on relevant information. The current study shows that, to some extent, there is an interagency collaboration, information regarding the oral health of children under investigation by CWS is being inquired and shared between the PDHS and CWS in Norway. The finding that PDHPs who have received inquiries report to have received several inquiries from CWS might support the assumption that CWS finds the information from PDHS relevant. Moreover, there is reason to believe that an inquiry from CWS can increase the PDHP’s awareness of the child under investigation, making them better positioned to facilitate dental treatment according to the child’s needs [Citation14].
Previous studies have addressed a need for a closer collaboration between PDHS and CWS[Citation16], the PDHP in Norway report to lack feedback from CWS in one fourth of their reported cases [Citation23,Citation26]. The findings in the present study, with close to half of the PDHP not having received an inquiry from CWS and close to one-third being unsure of the Health Personnel Act also imply that the services can benefit from increased knowledge and closer collaboration. A report from Norway revealed that CWS most often inquired about information from schools, public health clinics, general practitioners, medical doctors, police, and kindergartens in descending order [Citation6]. The PDHS is not mentioned but is most likely included in the category ‘other public health services’, which is rarely inquired by CWS [Citation6]. This might indicate that there is a need to raise awareness of what kind of information a child’s dental record can provide, that poor oral health can indicate that a child is at risk of abuse or neglect and that victims of abuse and neglect have an increased likelihood of having oral health needs, some of which can be complex [Citation16].
There is reason to believe that CWS and PDHS that succeed in sharing information when relevant might be better positioned to detect, support, and treat at-risk children. By inquiring information from children’s dental records, CWS might become better positioned to make well-founded decisions and PDHS becomes aware of children that might need a close and facilitated dental treatment. The present study presents some obstacles that should be addressed to enable good information flow between the PDHS and CWS. However, further research is needed. Future research should focus on employees in the CWS, assessing when and what information CWS inquires from PDHS and to what extent the inquired information from the children’s dental records contributes to new and relevant information for the CWS. This study is based on data represents the situation in 2012–2014, it would be interesting to see if the situation has changed over time. This study has implications for PDHS, CWS, and educational institutions.
In conclusion, the findings of this study show that the PDHP in Norway is being used as informants by the CWS. Slightly more than half of the responding PDHP received inquiries from the CWS within 3 years (2012–2014), with the majority having received multiple inquiries. Compared to their counterparts, PDHP’s likelihood of receiving inquiries from CWS seems to be significantly associated with being female, having more than 500 patients, working in municipalities with 10,000 or fewer inhabitants, working in eastern Norway, having good knowledge of the Health Personnel Act, and having experience reporting to CWS. Except for regional differences, the association between received inquiries from CWS and PDHP characteristics did not vary according to the PDHP’s previous reporting activity. Furthermore, a large portion of PDHP is uncertain about the Health Personnel Act [Citation7] and the information they can provide to the CWS. This indicates that measures should be taken to improve their knowledge and confidence regarding these issues.
Taken together, the present findings suggest that in order to increase PDHP’s likelihood of receiving inquiries, it is important to secure a good knowledge of the Health Personnel Act by the PDHPs [Citation7] and which information they can provide to the CWS when receiving an inquiry. In addition, it is important to establish contact between the CWS and PDHS and to familiarize themselves with one another.
Acknowledgements
The authors acknowledge and thank the dental hygienists and dentists working in the Public Dental Health Service in Norway for participating in this study.
Disclosure statement
The authors report no conflict of interest.
References
- Teicher MH, Samson JA, Anderson CM, et al. The effects of childhood maltreatment on brain structure, function and connectivity. Nat Rev Neurosci. 2016;17(10):652–666.
- Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356–e366.
- The child welfare act. Available from: https://lovdata.no/dokument/NL/lov/1992-07-17-100?q=barnevernloven. Accessed: 01/12/2019.
- Bellis MA, Hughes K, Leckenby N, et al. Measuring mortality and the burden of adult disease associated with adverse childhood experiences in England: a national survey. J Public Health. 2015;37(3):445–454.
- Peterson C, Florence C, Klevens J. The economic burden of child maltreatment in the United States, 2015. Child Abuse Negl. 2018;86:178–183.
- Christiansen Ø, Havnen K, Iversen AC, et al. Når barnevernet undersøker - Barnevernets undersøkelsesarbeid - delrapport 4. RKBU Nord; 2019. p. 259.
- The health personnel act. Available from: https://lovdata.no/dokument/NL/lov/1999-07-02-64?q=helsepersonell%20loven. Accessed: 09/01/2020.
- Widström E, Augustdottir H, Byrkeflot LI, et al. Systems for provision of oral health care in the Nordic countries. Tandlaegebladet. 2015;119(9):702–711.
- Gustafsson A, Persson C, Källestål C. Factors associated to non-attendance to dental care among adolescents—suggesting a model. PSYCH. 2018;09(13):2731–2751.
- Bhatia SK, Maguire SA, Chadwick BL, et al. Characteristics of child dental neglect: a systematic review. J Dent. 2014;42(3):229–239.
- Fisher-Owens S, Gansky S, Platt L, et al. Influences on children’s oral health: A. Conceptual model Evanston. Am Acad Pediatr. 2007;120(3):e510–e520.
- Hooley M, Skouteris H, Boganin C, et al. Parental influence and the development of dental caries in children aged 0–6 years: a systematic review of the literature. J Dent. 2012;40(11):873–885.
- Powell C, Appleton JV. Children and young people’s missed health care appointments: reconceptualising ‘did not attend’ to ‘was not brought’ – a review of the evidence for practice. J Res Nurs. 2012;17(2):181–192.
- Kvist T, Annerbäck EM, Dahllöf G. Oral health in children investigated by social services on suspicion of child abuse and neglect. Child Abuse Negl. 2018;76:515–523.
- Sillevis Smitt H, de Leeuw J, de Vries T. Association between severe dental caries and child abuse and neglect. J Oral Maxillofac Surg. 2017;75(11):2304–2306.
- Bradbury-Jones C, Isham L, Morris AJ, et al. The "Neglected" relationship between child maltreatment and oral health? An international scoping review of research. Trauma Violence Abuse. 2021;22(2):265–276.
- Dougall A, Fiske J. Surviving child sexual abuse: the relevance to dental practice. Dent Update. 2009;36(5):294–296, 298.
- Humphris G, King K. The prevalence of dental anxiety across previous distressing experiences. J Anxiety Disord. 2011;25(2):232–236.
- Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatrics, Section on Oral Health. Oral and dental aspects of child abuse and neglect. Pediatrics. 2017;140(2):e20171487.
- Søftestad S, Kranstad V, Fredriksen TV, et al. Invading deeply into self and everyday life: how oral health-related problems affect the lives of child sexual abuse survivors. J Child Sex Abus. 2020;29(1):62–78.
- Kranstad V, Søftestad S, Fredriksen TV, et al. Being considerate every step of the way: a qualitative study analysing trauma-sensitive dental treatment for childhood sexual abuse survivors . Eur J Oral Sci. 2019;127(6):539–546.
- Bright MA, Alford SM, Hinojosa MS, et al. Adverse childhood experiences and dental health in children and adolescents. Community Dent Oral Epidemiol. 2015;43(3):193–199.
- Brattabø IV, Iversen AC, Åstrøm AN, et al. Experience with suspecting child maltreatment in the Norwegian public dental health services, a national survey. Acta Odontol Scand. 2016;74(8):626–632.
- Bjørknes R, Iversen AC, Nordrehaug Åstrøm A, et al. Why are they reluctant to report? A study of the barriers to reporting to child welfare services among public dental healthcare personnel. Health Soc Care Community. 2019;27(4):871–879.
- Rønneberg A, Nordgarden H, Skaare AB, et al. Barriers and factors influencing communication between dental professionals and child welfare services in their everyday work. Int J Paediatr Dent. 2019;29(6):684–691.
- Brattabø IV, Bjørknes R, Åstrøm AN. Reasons for reported suspicion of child maltreatment and responses from the child welfare – a cross-sectional study of Norwegian public dental health personnel. BMC Oral Health. 2018;18(1):29.
- Brattabø IV, Bjørknes R, Breivik K, et al. Explaining the intention of dental health personnel to report suspected child maltreatment using a reasoned action approach. BMC Health Serv Res. 2019;19(1):1–14.
- Bakken A. Ungdata. Nasjonale resultater. Oslo: NOVA OsloMet; 2019. (NOVA Rapport 9/19).