
Abstract
Objective
To investigate dental caries prevalence amongst adults in Central Norway and assess changes over the last 45 years.
Materials and methods
The cross-sectional HUNT4 Oral Health Study was conducted in 2017-2019. A random sample of 4913 participants aged ≥19 years answered questionnaires and underwent clinical and radiographic examinations. Data were compared to findings from previous studies in the same region conducted from 1973 to 2006.
Results
Mean number of decayed, missing and filled teeth (D3-5MFT) was 14.9 (95% CI 14.7, 15.1), 56% of adults had one or more carious teeth (D3-5T) and 11.8% had ≥4 D3-5T, with the mean number of 1.4 (95% CI 1.32, 1.42). For initial caries, mean D1-2S was 3.8 (95% CI 3.7, 3.9), being the highest for 19-24-year-olds at 8.6 (95% CI 7.9, 9.3). Comparisons with earlier studies showed a decline in mean D3-5MFT for 35-44-year-olds from 26.5 in 1973 to 10.8 in 2019. In 1973, 4.8% of 35-44-year-olds were edentulous, while in present study edentulousness was found only in individuals >65 years.
Conclusions
Despite a substantial reduction in caries experience over the last 45 years, untreated dentine caries was common, evenly distributed across all age groups. Initial caries particularly affected younger individuals, indicating a need to evaluate prevention strategies and access to dental services.
Introduction
Untreated caries in permanent teeth is the most prevalent health condition globally [Citation1], estimated to affect ∼35% of the worldwide population in 2017 [Citation2]. In high-income countries, including the Scandinavian countries, the prevalence of caries and number of missing teeth, in both children and adults, has declined over the past decades [Citation1,Citation3–8]. Studies from Norway from the period 1968-2006 indicate a marked reduction in adult caries experience [Citation9–14]. However, data from a recent epidemiological study in Northern Norway imply that caries is still prevalent among adults, and that higher levels of disease are associated with living in rural areas and lower socio-economic status [Citation15]. More recent data on caries prevalence and distribution from other parts of Norway are lacking and to what level the trend of decline in caries experience still prevails is uncertain.
It has been argued that initial caries should be included in epidemiological studies, especially in populations with lower caries prevalence, to gain a comprehensive picture of the present caries disease status [Citation15–18]. Such inclusion reflects the trend of non-operative interventions in dentistry, facilitates a preventive approach to oral health care, and encourages resource allocation for preventive efforts [Citation19]. Two epidemiological studies in Northern Norway, showed a high prevalence of initial caries both among adolescents and adults [Citation15,Citation18]. However, data on initial caries prevalence and distribution from the rest of the country are lacking.
There is international focus on universal oral health care, that is, essential services available for all segments of a population, and the integration of dental care with other health care services, particularly primary care [Citation20]. It has been argued that integrated, universal services are best suited for focussing on promoting oral health, also as part of general health, with the aim of achieving oral health equity and handling underlying causes of oral disease [Citation20]. In Norway, equal access to oral health care was stated as a political aim in the 2006/7 White Paper on oral health care [Citation21]. In the recent election campaign for the 2021 parliamentary election, considerable attention was given to the present organisation and delivery of oral health care. The Norwegian government has declared its intention to gradually expand the Public Dental Service, with the aim of equating it with other health services [Citation22]. This political focus has called attention to the need for epidemiological data on the present oral health situation in the country, particularly among adults, as systematic collection of oral health data currently only exists for young people, 18 years of age and below [Citation23].
The first survey on oral health in the region of Central Norway in 1973 was initiated as part of the WHO International Collaborative Study and followed up in 1983, 1994 and 2006. The Trøndelag Health Study (HUNT) in 2017-2019 in the same region, included a cross-sectional study on adult oral health (HUNT4 Oral Health Study), intended to map current prevalence and distribution of oral diseases and time trends. The aims of the present study were to describe caries prevalence and distribution, including initial caries and edentulousness, amongst adults (≥19 years) in Central Norway and to assess 45-year-period time trends in caries disease using available data from previous studies in the region.
Materials and methods
Population
Data for the present study were collected as part of a repeated population‐based health investigation in Central Norway, The Trøndelag Health Study (HUNT). HUNT was initiated in 1984 and constitutes a large database for medical and health-related research [Citation24]. The HUNT4 Survey, was a cross-sectional survey conducted in the period September 2017-February 2019, where all adult residents (19 years or older) in the designated area (a total of 103,734 individuals), were invited to participate. A random sample (20%) of HUNT4-participants in six municipalities (Levanger, Stjørdal, Steinkjer, Verdal, Naerøy and Namsos) were invited to an oral health examination, the HUNT4 Oral Health Study, consisting of a total of 7347 individuals.
Data from the HUNT4 Oral Health Study were compared to previously published data from oral health studies conducted in the same geographical region (The Trøndelag studies and the HUNT3 Dental Survey [Citation25–27]. The first Trøndelag study in 1973 started as part of the WHO International Collaborative Study and was followed up by repeated studies in the same geographical area in 1983, 1994 and 2006. Random samples of participants were drawn by Statistics Norway and, despite declining response rates, data were considered representative at the time. For assessment of trends over time, the group of 35-44-year-olds, the WHO standard age-group for surveillance of oral health conditions in adults, was selected. Data from 827 individuals in 1973; 769 individuals in 1983; 135 individuals in 1994; and 158 in 2006, examined using the WHO methodology [Citation28] were available for comparisons. More detailed descriptions of the sampling and data collection in the previous studies have been formerly published [Citation10,Citation11,Citation25,Citation26].
Ethics
The study was approved by Regional Ethics Committee South-East Norway (REK 2019/28506) and all participants signed a written informed consent. Previous studies from the same geographical area to which data from this study are compared, were also given approval by public authorities and the Regional Ethics Committee Central Norway.
This article was prepared in accordance with the STROBE guidelines.
Caries registration and questionnaire
Data collection included self-administered questionnaires, interviews, and clinical and radiographic examination of participants at the HUNT4 field stations. Oral examinations were conducted by trained and calibrated dentists (n = 12) and dental hygienists (n = 7) from the Public Dental Service, according to a standardized examination protocol. A mobile dental unit with a compressor-run, air-syringe for drying, and a separate mobile stand examination light (Dr. Mach LED 130 F − 70,000 lux) was used for the examinations.
Caries registration included primary, secondary, and root surface caries. Clinically, dental caries was registered on dry surfaces using a dental mirror, a blunted probe (WHO periodontal probe, Plandent LM 550BSI) and cotton rolls using a 5-grade scale [Citation19]. Caries lesions on the root surface were registered by applying the International Caries Detection and Assessment System (ICDAS) criteria [Citation29]. Secondary caries was registered only when involving dentine. No magnification for caries detection was used. All missing teeth, independent of the reason for not being present, were registered as missing. Registrations of restorations included all types of filling materials and crowns.
Four bitewing radiographs of each participant were taken using an intraoral imaging unit, Planmeca Intra/Prostyle Intra, with a rectangular collimator (length 35 cm) and an intraoral sensor, Planmeca ProSensor HD. Edentulous and pregnant (first trimester) participants were excluded from radiographic examinations. Radiographic caries registration for approximal surfaces of premolars and molars and distal surfaces of canines was carried out after the clinical examination by three trained and calibrated examiners (one dentist and two dental hygienists) using standardized conditions and were recorded using a 5-grade scale [Citation19]. These registrations supplemented the clinical registrations and final approximal D1-5S scores were computed for each approximal surface based on the most severe caries registration.
Decayed, missing (MS) and filled surfaces (FS) and teeth (DMFS and DMFT) were calculated using the clinical and radiographic caries registration of dental status. Third molars were not included.
For DMFS calculations, four surfaces were assigned to incisors and canines and five surfaces to premolars and molars. Calculated D1-2 component included caries grades 1-2 and root caries without cavitation. D3-5 component included caries grades 3-5, secondary caries, and root caries with cavitation. The F (filled) component comprised restorations without secondary caries including all types of filling materials and crowns.
All participants answered questionnaires regarding general and oral health, lifestyle, and socio-economic factors, and were interviewed regarding ethnicity/family background. In the present study, information on age, gender, family background, education, and income were included for examination of external validity. The study population was categorized into the following age groups: 19-24; 25-34; 35-44; 45-54; 55-64; 65-74 and 75+. Education was registered for the highest level of education and categorized into ‘basic’ (9-10 years compulsory school), ‘middle’ (secondary school or vocational training, started/completed) and ‘higher’ (college/university level). Yearly income was registered on the household level before taxation and categorized into ‘low’ (≤NOK450,000), ‘middle’ (NOK451,000-1,000,000) and ‘high’ (>NOK1,000,000). Family background was registered as the residence at one year of age for participants and the birthplace of their biological parents. These variables were dichotomized into ‘Norway’ or ‘Other’ (Europe, Africa, Asia, North and Central America, South America, Oceania).
Reliability
Training of the 19 examiners prior to data collection consisted of information meetings and clinical examination of volunteers, during which the criteria used in the dental examinations were discussed.
Calibration sessions for the dentists and dental hygienists (n = 19) were performed prior to and during the data collection period. Prior to data collection, examiners at each field station performed independent clinical examinations of nine volunteers. The Cohen’s kappa values for inter-examiner agreement based on these examinations were calculated for sound, decayed initial (grades 1-2), decayed dentine (grades 3-5) and filled surfaces (FSs). The score varied from 0.71 to 0.91.
In addition, the 19 examiners performed caries registrations on a set of clinical, intra-oral photographs. Kappa values for inter-examiner agreement reliability were 0.82 at the beginning of the data collection and 0.85 later in the period. Kappa values for intra-examiner agreement based on the same set of intra-oral photographs for sound, decayed initial (grades 1-2), decayed dentine (grades 3-5), and FSs ranged from 0.79 to 0.93.
For the radiographic caries registrations, the three examiners dedicated to this task performed independent repeated scorings on ten sets of bitewings. Kappa values for inter-examiner reliability were calculated for sound, decayed initial (grades 1-2), decayed dentine (grades 3-5) and FSs and were 0.87 and 0.84 for the first and second calibration sessions, respectively. The kappa values for intra-examiner reliability for the three examiners were between 0.84 and 0.87.
The time between repeated examinations varied between the field stations, with a minimum of three weeks. For radiographs registrations, repeated examinations were performed after a minimum of one month.
Statistical methods
The electronic dental record system (Opus Dental 7.1) was used for data collection at the HUNT4 field stations. At the Centre for Oral Health Services and Research, Mid-Norway, a script, developed by Garnes data, was applied to extract the dental status registrations. IBM®SPSS® Statistics 26 was used for the analyses.
In descriptive analyses, prevalence estimates and mean values were presented with 95% confidence intervals and median values with interquartile ranges (IQR). Socio-demographic characteristics of participants in the HUNT4 Oral Health Study were compared to the general population, county of Trøndelag, using data from Statistics Norway Microdata [Citation30], to assess the potential selection bias. DMFT and DT were shown as frequency distributions, while changes in DMFT and edentulousness over a 45-year-period were presented using estimates of prevalence from previous studies. Independent samples t-test with 5% significance level was used to compare means.
Results
Study population
Of 7347 individuals invited to participate in the HUNT4 Oral Health Survey, 4933 accepted and 4913 completed clinical and radiographic examination (response rate: 67%).
A comparison of the study participants with the general population in the region showed that among study participants, there was an underrepresentation of men, individuals with basic education, and high income ().
Table 1. Socio-demographic characteristics of participants in the HUNT4 Oral Health Study and general population, county of Trøndelag.
The study population was homogenous with regard to family background. Altogether, 4666 (94.9%) participants of the study population lived in Norway at one year of age. Of the 247 (5.1%) individuals who lived outside Norway at one year of age, 124 individuals (50.2%) lived in Europe. Most of the total study population had biological parents born in Norway (94% had a mother born in Norway; 93.1% had a father born in Norway). In the reference population, 16.5% are registered with a background other than Norway, either through their own birth or parents’ birth outside Norway, and individuals with such a background are thus under-represented in the study population.
Dental caries prevalence
Of 4913 participants, 33 were edentulous and therefore excluded from calculations regarding caries experience. Among dentate individuals (n = 4880), the mean number of present teeth was 25.5 (95% CI 25.4, 25.6) and 55.7% (95% CI 54.3, 57.0) of the examined individuals had one or more teeth with caries (D3-5T).
Caries experience in the present study is presented in . The overall mean number of teeth with dentine caries (D3-5T) was 1.4 (95% CI 1.3, 1.4), and there was little variation in relation to age, with a mean D3-5T between 1.2 and 1.5 in the different age-groups. The results showed that men had a significantly higher D3-5T score compared to women, 1.6 (95% CI 1.5, 1.7) versus 1.2 (95% CI 1.1, 1.3) teeth, p < .01.
Table 2. Caries experience in the HUNT4 Oral Health Study.
Supplementary Table S1 presents the median values (IQR) for caries experience.
Secondary caries comprised the largest part of the overall mean number of D3-5T component (0.7), followed by the mean number of dentine caries grade 3 (0.5) and the mean number of dentine caries grades 4-5 (0.1).
Cumulative distribution of caries in relation to age
The cumulative percentage distributions of D3-5MFT in show that caries experience was low for the three youngest age groups; while 11.5% (95% CI 8.3, 15.4) for the 19-24-year-olds; and 6.4% (95% CI 4.6, 8.6) for the 25-34 age-group had D3-5MFT = 0. The distributions for four age-groups over 45 years of age all have slightly s-shaped curves, indicating increasing proportion of individuals with a higher D3-5MFT-scores.
Figure 1. Cumulative frequency distributions of D3-5MFT according to age group, in the HUNT4 Oral Health Study.
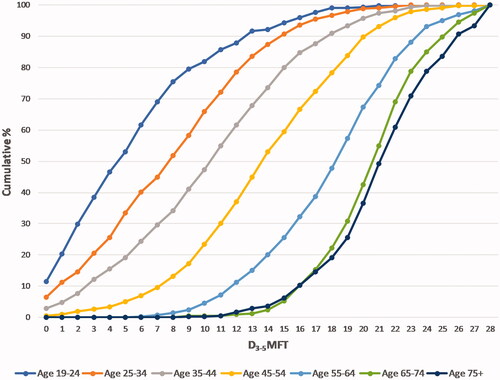
The distribution of untreated dentine caries followed a similar pattern in all age-groups (Supplementary Figure S1); 11.8% (95% CI 10.9, 12.7) of the study population had four or more teeth with untreated dentine caries, while 1.4% (95% CI 1.1, 1.8) had eight or more teeth with untreated dentine caries.
Initial caries
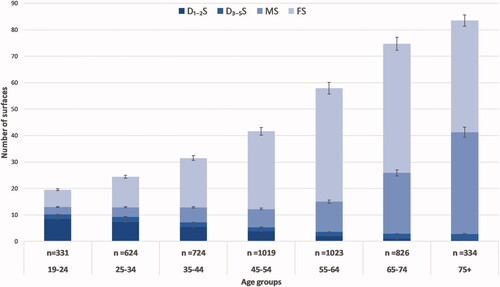
When both initial and dentine lesions (D1-5S) were considered, 85.8% (95% CI 84.8, 86.8) of the total study population had one or more carious surfaces. Initial caries was particularly prevalent in the younger age groups, with a mean number of D1-2T of 4.7 for 19-24-year-olds.
illustrates distribution of DMFS index components in relation to age. Despite low total caries experience in the youngest age groups, the mean number of surfaces with initial caries was highest among 19-44-year-olds. In the youngest age-group (19-24), 94.6% (95% CI 91.5, 96.8) had one or more surfaces with initial or dentine caries (D1-5S), compared to 48.3% (95% CI 42.8, 53.9) with one or more surfaces with dentine caries only (D3-5S) in the same age group.
Figure 2. Mean (95% CI) number of initial decay surfaces (D1-2S) and dentine (D3-5S), missing surfaces (MS) and filled surfaces (FS), in relation to age.
Trends in edentulousness and caries experience over time
Edentulousness was found in 0.7% (95% CI 0.69, 0.71) of the study population. All edentulous individuals were above the age of 65 years, with 21 individuals (63.6%) above the age of 75 years. The prevalence of edentulousness in the 65+ population was 3.3% (95% CI 2.0, 5.0) for women and 2.2% (95% CI 1.2, 3.8) for men.
shows a decrease in edentulousness in the age groups 35-44, 45-54, and 55-64 over a 45-year-period. In 1973, 40 individuals (4.8%) of the 35-44-year-olds population (n = 827) were edentulous [Citation26]. There were also registered edentulous individuals in this age group in 1983 and 1994 [Citation10,Citation25]. In the present study, edentulousness was absent in all these age groups.
Figure 3. Changes in caries experience (mean D3-5MFT) among dentate Norwegians aged 35-44 in 1973, 1983, 1994, 2006 and 2017-2019. Data from previous studies [Citation25–Citation27] and the present study. Numbers from 1973 are estimates based on weighted averages of urban and rural populations [Citation25].
![Figure 3. Changes in caries experience (mean D3-5MFT) among dentate Norwegians aged 35-44 in 1973, 1983, 1994, 2006 and 2017-2019. Data from previous studies [Citation25–Citation27] and the present study. Numbers from 1973 are estimates based on weighted averages of urban and rural populations [Citation25].](/cms/asset/0aa458e1-a3e1-40ef-b48d-ba20d4c3a2f3/iode_a_2117735_f0003_c.jpg)
Table 3. Changes in prevalence (95% CI) of edentulousness, by age 35-44, 45-54 and 55-64 in 1973, 1983, 1994 and 2017-2019.
There has been a substantial decline in mean D3-5MFT scores for 35-44-year-olds, indicating a decrease of 59% during this 45-year-period, from 26.6 to 10.8. illustrates how the relative distribution of the different D3-5MFT components has changed over time. The mean number of missing teeth (MT) has steadily declined from 11.9 in 1973 to 1.2 in the current study, a 90% decline during the period. Filled teeth (FT) peaked in 1994 at a mean value of 17.9, while in the present study it was down to 8.2. Mean figures for decayed teeth (D3-5T) show the least variation over time, with the lowest mean of 0.6 registered in 1994.
Discussion
More than half the population in the current study had untreated dentine caries, evenly distributed between the different age-groups. The distribution of caries was skewed, with about 12% of examined individuals having four or more teeth with untreated dentine caries, while ∼65% had one tooth with dentine caries or no caries registered. When initial caries was included in the calculations, the overall prevalence increased to 80%, with most of the initial caries found in the younger age-groups. At the same time, a substantial improvement in mean D3-5MFT numbers among 35-44-year-olds since 1973 was observed, when caries experience from the present study was compared to data from previous studies in the region. This was particularly evident in a gradual decrease in mean numbers of missing and filled teeth. There was also a considerable decline in the proportions of edentulous individuals.
Findings in the present study are in line with results from a recent epidemiological caries study in Northern Norway. Compared to the TOHNN study [Citation15], mean D3-5MFT for the two study populations is very similar, as are the gender differences in the D3-5MFT index. However, participants in the present study had higher mean numbers for both initial and dentine caries compared to both the TOHNN study and two other studies from Northern Norway, one in a Sami area [Citation31] and one in an elderly population [Citation16]. The observed differences may partly be explained by differences in caries registration methods and characteristics of the study populations. Secondary caries was not included in caries registrations in the TOHNN study [Citation15] and the population in our study was less urban. Moreover, further comparisons with the aforementioned studies are challenging due to the different age stratification of the study populations.
When initial caries was included in the DMF calculations, a marked increase in caries prevalence was observed, especially for the youngest age groups. In the present study, 95% of 19-25-year-olds had one or more surfaces with initial and dentine caries (D1-5S). This is in line with findings from another study from Northern Norway [Citation18], where in a sample of 16-year-olds, 34% had untreated dentine caries, and, when proximal initial caries lesions were included, the overall prevalence increased to 85%. There was no differentiation between inactive and active initial caries lesions in the present study, thus the number of lesions in need of non-operative treatment is probably to some extent overestimated. However, the findings indicate a continual need for preventive measures and non-operative treatment of caries disease.
Despite the reduction in the total caries experience, the prevalence of untreated dentine caries remained high: 56% of the study population had untreated dentine caries and one in ten had four or more dentine lesions. The prevalence of untreated dentine caries in the present study was higher compared to recent international studies in adults. In a Swedish study [Citation8] in a similar population, 33% were found to have at least one decayed surface, and recent findings in an Australian study [Citation32], identified 32% in an adult population to have untreated caries. Interestingly, a recent German study [Citation7], shows consistently both higher mean D3-5MFT and lower mean D3-5T numbers compared to the present study. The authors hypothesize that the low D component is explained by the standard of dental care and insurance coverage in Germany. It might be speculated that one of the reasons the prevalence of untreated dentine caries in the present study was higher, is because of the Nordic minimally invasive approach, that is, some of the dentine lesions in the present study may have been under observation and managed non-operatively at the time of data collection [Citation33]. This is further supported by the close examination of the dentine caries data in the present study, showing that ∼1/3 of the dentine caries were grade 3 lesions. Thus, the higher threshold for operative treatment may partly explain the increase in the D-component since 1994 observed in the present study. Still, there is a need for further investigation of the distribution and determinants of untreated dentine caries in the study population.
Findings from the present study indicate a continuation of the overall trend of decrease in total caries experience for 35-44-year-olds observed in earlier cross-sectional studies from the same region in Norway [Citation10,Citation25–27] and in studies on 35-year-old individuals in Oslo [Citation12–14]. A similar trend of caries decline is observed in several European countries, presented in a recent review [Citation34]. Data from repeated cross-sectional studies in 13 different European countries, the oldest study from 1985, displayed mean D3-5MFT for 35-44-year-olds ranging from 6.5 to 17.6 [Citation34]. With a mean D3-5MFT of 10.8 for this age-group, the present study is in line with the European figures [Citation34]. In 2003, WHO classified Norway at ‘high level dental caries’ for 35-44-year-olds [Citation35], while the present study would place Norway in the ‘moderate’ cluster for this age-group.
The present study is the largest oral health study performed in Norway and provides comprehensive information about the current oral health situation in the country, including data on initial caries, caries distribution, and epidemiological changes in caries. In addition, the study was part of a larger health survey, which allows for further studies of oral health in a broader perspective. The region in which the study was conducted is considered to be fairly representative of Norway, except for the lack of large cities and immigrant populations [Citation36].
However, there are some methodological limitations of the present study that must be considered when interpreting the results. The general decline in participation rates in health surveys is apparent also in this study; the participation rate for the first HUNT survey in 1986 was 89%, while in the HUNT4 Survey it was 54% [Citation36]. The randomly selected individuals in the HUNT4 Oral Health Study were invited from participants already included in the HUNT4 Survey, and thus selection bias may have occurred in the population studied and the external validity of this study must be considered with caution. A study from HUNT4 [Citation36] showed that non-participants had a less healthy lifestyle, lower self-reported health, and higher morbidity than participants. When the present study population was compared with the general population in the geographical area (), over-representation of participants with higher education and women was evident. As women had a lower mean number of decayed teeth and surfaces than men in the present study, there is a possibility that caries experience in the general population is underestimated. Comparisons of data from the six municipalities of the study population versus the reference population, show both lower levels of education and of household incomes in the area where the study was performed [Citation37]. Also, home nursing and nursing home residency were less common among participants [Citation36]. Institutionalized older adults have been found to be in reduced general and oral health in comparison to the general elderly population [Citation38]. As a result, it may be that caries prevalence and edentulousness is higher in the general population than estimated in the present study, particularly among older adults. Considering the mentioned aspects, the findings of the present study may be generalized to other non-urban populations in similar settings, however, due to ethnically homogeneous population, the generalisability of the findings to people of non-European origin is limited [Citation36].
When interpreting the findings, the methodological limitations of the DMF index and its different components require further discussion. The missing component (M) in the present study included teeth missing due to any reason, while in 1973 only teeth lost to caries were included. In the present study, including all tooth loss may have led to an overestimation of caries experience with regards to the M-component in the DMF index, as teeth lost to, for example orthodontic extractions or periodontal disease were included.
The filled component (F) comprised the largest proportion of the DMF index in the present study and the number of filled teeth/surfaces increased with age. The F-component is influenced by the dentists’ restorative treatment decisions. The clinical judgement of the dentist determines the choice of treatment, influenced by the prevailing philosophy of care. Fluoride-containing toothpaste became available over-the-counter in Norway in 1971 and since the 1980s there has been a gradual shift in treatment criteria, with an increased focus on preventive measures, delayed operative treatment, and minimally invasive approach using adhesive techniques [Citation39]. There has also been an estimated reduction in yearly sugar consumption per individual in Norway from 44 to 24 kg in the period from 1999 to 2019 [Citation40]. Availability of oral health care services has increased over time, and geographical access to dental care is for most areas good with a national average of nine dentists per 10,000 inhabitants [Citation23]. These factors have jointly over time contributed to a decreasing F-component and they are mirrored in the different age-groups in the present study. Especially the two oldest age-groups have had less benefit of fluorides and will have received restorative treatment in a period when treatment principles and dental materials resulted in more and larger preparations. It is apparent that the two oldest age-groups in the cumulative frequency distribution of DMFT in , have the largest proportions of individuals with high DMFT numbers compared to younger age groups.
The decline in total caries experience over time for 35-44-year-olds shown in this study, indicates an overall decreased need for operative dental treatment in the population, also in the years to come. It has been argued that the decline in caries seen globally over the past decades should bring about adjustments to the training of dental professionals and the setup of oral health care services with a less operative and more preventive practice [Citation34,Citation41]. The findings in this study support this approach. At the same time, the relatively high prevalence of untreated dentine caries in all age-groups and an uneven distribution of caries in the study population, suggest that despite the high availability of dental services, barriers to treatment for some individuals may exist and need to be further investigated. In Norway, the Public Dental Service offers free treatment for children and adolescents up to 19 years of age. Dental treatment for adults is provided by private practitioners and paid out of pocket with few exceptions. Although the number of dentists in relation to the population is higher in Norway than in most countries in the world [Citation42], a recent study in Norway found that approximately one fifth of adult participants had postponed dental visits during the past two years due to financial reasons [Citation43]. There is a need for more research on barriers and availability of services among different age groups. Determinants for caries in subgroups with reduced oral health also need further exploration. Currently, universal health coverage and integrating dentistry within general health services is suggested as an approach to reduce inequity in health and to promote prevention [Citation20]. Our findings regarding untreated caries, including initial caries, emphasize the importance of a preventive approach both at individual and population level. Younger age-groups in particular have high levels of initial caries and there is a potential for oral health gain in a lifelong perspective through preventive measures.
This study demonstrates a considerable reduction in caries disease over the past decades. At the same time, more than half the examined population had untreated dentine caries, with a skewed distribution of lesions in all age-groups. There was a high prevalence of initial caries, affecting younger individuals primarily. The findings suggest a need to reconsider both preventive measures and the access to oral health care services for subgroups of the adult population.
Supplementary_Figure_S1.tif
Download TIFF Image (601.7 KB)Acknowledgements
The Trøndelag Health Study (HUNT) is a collaboration between HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology NTNU), Trøndelag County Council, Central Norway Regional Health Authority, and the Norwegian Institute of Public Health. Dentists and dental hygienists from the Public Dental Service in the county of Trøndelag performed the clinical examinations. The authors also recognize the contribution of Elise Taylor Spets, Umar Sharif and Sakkina Pathmaharan for interpreting the radiographic images and of Line Cathrine Nymoen for her involvement in the data collection and quality control.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data are stored in HUNT databank and biological material in HUNT biobank. HUNT Research Centre has permission from the Norwegian Data Protection Authority to store and handle these data. The key identification in the data base is the personal identification number given to all Norwegians at birth or immigration, whilst de-identified data are sent to researchers upon approval of a research protocol by the Regional Ethical Committee and HUNT Research Centre. To protect participants’ privacy, HUNT Research Centre aims to limit storage of data outside HUNT databank and cannot deposit data in open repositories. HUNT databank holds precise information on all data exported to different projects and can reproduce these on request. There are no restrictions regarding data export given approval of applications to HUNT Research Centre. For more information see: www.ntnu.edu/hunt/data.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Related Research Data
References
- Peres MA, Macpherson LMD, Weyant RJ, et al. Oral diseases: a global public health challenge. Lancet. 2019;394(10194):249–260.
- Bernabe E, Marcenes W, Hernandez CR, GBD 2017 Oral Disorders Collaborators, et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. 2020;99(4):362–373.
- Hugoson A, Koch G, Göthberg C, et al. Oral health of individuals aged 3-80 years in Jönköping, Sweden during 30 years (1973–2003). II. Review of clinical and radiographic findings. Swed Dent J. 2005;29(4):139–155.
- Petersen PE, Kjøller M, Christensen LB, et al. Changing dentate status of adults, use of dental health services, and achievement of national dental health goals in Denmark by the year 2000. J Public Health Dent. 2004;64(3):127–135.
- Beltrán-Aguilar ED, Barker LK, Canto MT, Centers for Disease Control and Prevention (CDC), et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis–United States, 1988–1994 and 1999–2002. MMWR Surveill Summ. 2005;54(3):1–43.
- Nunn J, Morris J, Pine C, et al. The condition of teeth in the UK in 1998 and implications for the future. Br Dent J. 2000;189(12):639–644.
- Schmoeckel J, Haq JA, Samietz S, et al. Ten-year trends in DMF-S and DMF-T in a northeast German adult population. J Dent. 2021;111:1–7.
- Edman K, Öhrn K, Nordström B, et al. Prevalence of dental caries and influencing factors, time trends over a 30-year period in an adult population. Epidemiological studies between 1983 and 2013 in the county of Dalarna, Sweden. Acta Odontol Scand. 2016;74(5):385–392.
- Asmyhr O, Grytten L, Grytten J. Changing trends in caries experience among male military recruits in Norway. Community Dent Oral Epidemiol. 1994;22(3):206–207.
- Schuller AA, Holst D. Changes in the oral health of adults from Trøndelag, Norway, 1973–1983–1994. Community Dent Oral Epidemiol. 1998;26(3):201–208.
- Holst D, Schuller AA. Oral health in a life-course: birth-cohorts from 1929 to 2006 in Norway. Community Dent Health. 2012;29:134–143.
- Bjertness E, Eriksen HM, Hansen BF. Caries prevalence of 35-year-old Oslo citizens in 1973 and 1984. Community Dent Oral Epidemiol. 1986;14(5):277–282.
- Berset GP, Eriksen HM, Bjertness E, et al. Caries experience of 35-year-old Oslo residents and changes over a 20-year period. Community Dent Health. 1996;13:238–244.
- Skudutyte-Rysstad R, Eriksen HM. Changes in caries experience among 35-year-old Oslo citizens, 1973-2003. Acta Odontol Scand. 2007;65(2):72–77.
- Oscarson N, Espelid I, Jonsson B. Is caries equally distributed in adults? A population-based cross-sectional study in Norway – the TOHNN-study. Acta Odontol Scand. 2017;75(8):557–563.
- Mulic A, Tveit AB, Stenhagen KR, et al. The frequency of enamel and dentin caries lesions among elderly Norwegians. Acta Odontol Scand. 2020;78(1):6–12.
- Skeie MS, Klock KS. Scandinavian systems monitoring the oral health in children and adolescents; an evaluation of their quality and utility in the light of modern perspectives of caries management. BMC Oral Health. 2014;14:43.
- Jacobsen ID, Crossner CG, Eriksen HM, et al. Need of non-operative caries treatment in 16-year-olds from Northern Norway. Eur Arch Paediatr Dent. 2019;20(2):73–78.
- Amarante E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998;26(2):87–94.
- Watt RG, Daly B, Allison P, et al. Ending the neglect of global oral health: time for radical action. Lancet 2019;394(10194):261–272.
- Regjeringen. The Norwegian White Paper on oral health care 2006–2007 (in Norwegian) [Internet]. Regjeringen; 2007 [cited 2022 Jan 2]. Available from https://www.regjeringen.no/no/dokumenter/Stmeld-nr-35-2006-2007-/id475114/.
- Regjeringen. The platform of the Norwegian government 2021–2025 (in Norwegian) [Internet]. Regjeringen; 2021 [cited 2022 Jan 2]. Available from: https://www.regjeringen.no/no/dokumenter/hurdalsplattformen/id2877252/.
- Statistics Norway. Dental health (in Norwegian)[Internet]. SSB; 2021 [cited 2021 Dec 12]. Available from: https://www.ssb.no/.
- Krokstad S, Langhammer A, Hveem K, et al. Cohort profile: the HUNT study, Norway. Int J Epidemiol. 2013;42(4):968–977.
- Baerum P, Holst D, Rise J. Tannhelseutviklingen 1973–1983: en rapport fra Trøndelagsundersøkelsen. [Changes in dental health 1973–1983: the Trøndelag survey report] Oslo: Helsedirektoratet; 1984.
- Arnljot HA. Oral health care systems: an international collaborative study coordinated by World Health Organisation. London: Quintessence; 1985.
- Holst D, Schuller AA. Equality in adults’ oral health in Norway. Cohort and cross-sectional results over 33 years. Community Dent Oral Epidemiol. 2011;39(6):488–497.
- [WHO. Oral health surveys: basic methods. 5th ed. Geneva: WHO Library Cataloguing-in-Publication Data; 2013.
- Pitts N. Detection, assessment, diagnosis and monitoring of caries. Basel; New York: Karger; 2009. p. 15–41.
- Statistics Norway. Microdata (in Norwegian) [Internet]. SSB; 2021 [cited 2021 Sep 6]. Available from: https://microdata.no/.
- Bongo AKS, Brustad M, Jönsson B. Caries experience among adults in core Sámi areas of Northern Norway. Community Dent Oral Epidemiol. 2021;49(5):401–409.
- Peres KG, Ha DH, Christofis S. Trend and distribution of coronal dental caries in Australians adults. Australian Dental Journal 2020;65(1 Suppl):S32-S39
- Schwendicke F, Splieth C, Breschi L, et al. When to intervene in the caries process? An expert Delphi consensus statement. Clin Oral Investig. 2019;23(10):3691–3703.
- Carvalho JC, Schiffner U. Dental caries in European adults and senior citizens 1996–2016: ORCA saturday afternoon symposium in Greifswald, Germany – Part II. Caries Res. 2019;53(3):242–252.
- Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century: the approach of the WHO Global Oral Health Programme. Geneva: World Health Organization; 2003.
- Åsvold BO, Langhammer A, Rehn TA, et al. Cohort profile update: the HUNT study, Norway. Int J Epidemiol. 2022;0:1–12.
- NIPH. Public health profiles Norwegian muncipalities [Internet]. NIPH; 2019 [cited 2022 Feb 18]. Available from: https://www.fhi.no/en/hn/health-in-the-municipalities/hent-folkehelseprofil-for-kommune-fylke-eller-bydel/.
- Wong FMF, Ng YTY, Leung WK. Oral health and its associated factors among older institutionalized residents-a systematic review. Int J Environ Res Public Health. 2019;16:4132.
- Vidnes-Kopperud S, Tveit AB, Espelid I. Changes in the treatment concept for approximal caries from 1983 to 2009 in Norway. Caries Res. 2011;45(2):113–120.
- NIPH. Norwegian Institute of Public Health (in Norwegian) [Internet]. NIPH; 2022 [cited 2022 May 4]. Available from: https://www.fhi.no/nettpub/hin/levevaner/kosthald/.
- Fejerskov O, Escobar G, Jøssing M, et al. A functional natural dentition for all–and for life? The oral healthcare system needs revision. J Oral Rehabil. 2013;40(9):707–722.
- Grytten J, Listl S, Skau I. Do Norwegian private dental practitioners with too few patients compensate for their loss of income by providing more services or by raising their fees? Community Dent Oral Epidemiol. 2022;0:1–8.
- Hadler-Olsen E, Jönsson B. Oral health and use of dental services in different stages of adulthood in Norway: a cross sectional study. BMC Oral Health. 2021;21(1):257.