Abstract
Background We examined histological changes in the undersurface of the acromion in patients with symptoms of subacromial impingement, in order to clarify whether or not these changes are the main cause of rotator cuff tear.
Methods We studied 39 shoulders. The undersurface of the acromion and the coracoacromial ligament were examined by light microscopy and transmission electron microscopy.
Results The distinct four-layer structure seen in the undersurface of the acromion of normal subjects was not found in any of our patients. In patients with full-thickness cuff tear, the extent of the tear had a greater association with the degree of degeneration in the undersurface of the acromion than age or the duration of illness. There was little association between structural changes in the coracoacromial ligament and the extent of or the presence of full-thickness cuff tear, or the duration of illness, but there was a strong association with patient age.
Interpretation The histological changes in the undersurface of the acromion in patients without cuff tear were merely minute changes compared to those in patients with full-thickness cuff tear. We conclude that the advanced degenerative changes in the undersurface of the acromion result from full-thickness cuff tear.
The undersurface of the acromion, including the coracoacromial ligament, plays a critical role as the subacromial arch in the functional movement of the shoulder. Codman (Citation1934) ascribed the pathogenesis of cuff tear to degeneration of the cuff itself, while Neer (Citation1972) attributed it to wear and tear of the cuff due to subacromial impingement, and suggested that qualitative changes in the undersurface of the acromion were associated with cuff tear. Bigliani (Citation1991) classified morphological features of the acromion into 3 types, demonstrating that acromial morphology was closely connected to the pathogenesis of cuff tear. There have, however, been no definitive conclusions to date as to whether morphological changes in the acromion are the main cause of cuff tear, or whether they are secondary changes caused by the tear.
The purpose of our study was (1) to clarify whether or not the pathological changes in the undersurface of the acromion, which are observed in patients without cuff tear, show advanced degenerative changes to be the cause of cuff tear, and (2) to investigate any association between the pathological changes in the coracoacromial ligament and aging, the presence or absence of cuff tear, and the extent of cuff tear.
Patients
The subjects consisted of 39 patients (30 men) who had symptoms of subacromial impingement. The mean age at the time of surgery was 60 (22–80) years, and the mean duration of symptoms was 14 (3–84) months. Based on the intraoperative findings, the cases were classified as 11 shoulders without cuff tear and 28 shoulders with full-thickness cuff tear. The former included 4 shoulders with a history of trauma and 7 shoulders with no trauma, and the latter included 19 shoulders with a history of trauma and 9 shoulders with no trauma.
Degenerative changes of the cuff such as fraying, which engaged less than one-third of the tendon thickness on intraoperative findings, were not classified as cuff tear. The size of full-thickness cuff tear was classified into 3 groups according to the Post (Citation1983) classification. We observed small tears in 4 shoulders, medium tears in 12 shoulders and large to massive tears in 12 shoulders.
Methods
To assess the radiographic findings of the acromion, scapulolateral views were obtained preoperatively in all patients. We evaluated the morphology of the acromion using Bigliani's criteria (Citation1991). We studied the relationship between the size of full-thickness cuff tear and age, the duration of symptoms, and the history of trauma.
During surgery, the undersurface of the acromion was dissected en bloc along with the coracoacromial ligament. The bone was then sliced in half along the course of the coracoacromial ligament. Directly along the incision, one side was fixed in 10% formalin and was embedded in paraffin. After staining this side with hematoxylineosin (HE), pH 4.1 toluidine blue (TB), and Elastica van Gieson (E-V; Weigert method), the region to which the coracoacromial ligament was attached on the undersurface of the acromion, and the coracoacromial ligament, were examined by light microscopy. The undersurface of the acromion with the coracoacromial ligament was divided in two pices. One piece was fixed in 10% formalin. The other piece was prefixed in 4% paraformaldehyde and 1% glutaraldehyde for 24 h, decalcified with 8% EDTA, and slivered along the course of the coracoacromial ligament. Subsequently, the strip was postfixed in 2% osmium tetroxide for 2 h. The specimen was dehydrated with ascending grades of ethanol, which was substituted by propylene oxide, and it was then embedded in Epon 812. Using a Reichert-type microtome, ultra-thin sections approximately 60 nm thick were prepared and double-stained with uranium acetate and lead acetate. Finally, the coracoacromial ligament and fibrocartilage layer in the region of ligament attachment were examined under a transmission electron microscope (TEM; H-600A, Hitachi) at an accelerating voltage of 75 kV and direct magnification of 1,800–60,000.
Statistics
Differences for any parameters were assessed with the Student t test. The relationships between all parameters were measured using Pearson correlation coefficients if the variable fitted a normal distribution curve; otherwise we used Spearman correlation coefficients. The correlations between parameters were calculated by linear regression analysis.
Results
Radiographic evaluation
Regarding the morphology of the acromion, there were 18 type II shoulders, and 21 type III shoulders. There was no difference in frequency between type II and type III, and there was no difference in the presence or absence of cuff tear (p = 0.2) ().
Table 1. Morphology of the acromion according to the Bigliani classification
Macroscopic examination
All patients without cuff tear had mild fibrillation of the cuff on the subacromial bursal side. On the other hand, among patients with full-thickness cuff tear (n = 28), small and medium tears were noted in every age group, while about four-fifths of large tears were observed in patients aged 60 or older. But there was no correlation between the size of cuff tear and the duration of symptoms (p = 0.2), or the history of trauma (p = 0.7).
Light microscopic examination
The coracoacromial ligament. In all patients without cuff tear, the synovial membrane on the inferior surface of the coracoacromial ligament was stratified, but it disappeared in areas closer to the region of ligament attachment on the undersurface of the acromion. The fiber architecture of the ligament showed a dense and regular arrangement in a uniform direction in young patients, while in elderly patients, gaps appeared between fibers, which showed a coarse arrangement. The intensity of E-V staining of elastic fiber was reduced with aging. In patients with full-thickness cuff tear, changes in the synovial membrane and the fiber architecture of the ligament, and decreased intensity of E-V staining, were similar to those in patients without cuff tear. However, these changes were little affected by the size of or the presence of cuff tear, or the history of trauma, but were mainly affected by age.
Undersurface of the acromion (region of ligament attachment). All patients without cuff tear had breakdown of the four-layer structure (composed of the synovial membrane, collagenous fiber layer, fibrocartilage layer, and osseous layer) on the undersurface of the acromion, which can also be seen in normal subjects. The synovial membrane had disappeared, and fissures or wear and tear were noted in the collagenous fiber layer. These findings became more marked with aging. There were no abnormalities in the fibrocartilage layer in young patients. In elderly patients, the layer showed a tendency towards proliferation. There were no abnormal findings in the osseous layer, regardless of age. In full-thickness cuff tear, the diverse changes in the four-layer structure on the undersurface of the acromion could be classified into the following 4 types (): Type I (): changes up to the collagenous fiber layer (2 shoulders); type II (): appearance of reactive changes in the fibrocartilage layer (7 shoulders); type III (): disappearance of the collagenous fiber layer and remaining reactive changes in the fibrocartilage layer (6 shoulders); and type IV (): disappearance of the fibrocartilage layer and exposure of the osseous layer (11 shoulders). These changes were more markedly affected by the size of full-thickness cuff tear (p = 0.02) than the age of the patient (p = 0.5) or the duration of illness (p = 0.1) (). In patients without cuff tear, minute changes, not more than those corresponding to type II, were observed.
Figure 1. Type I:changes up to the collagenous fiber layer (fissures or wear and tear were only noted in this layer.×100).
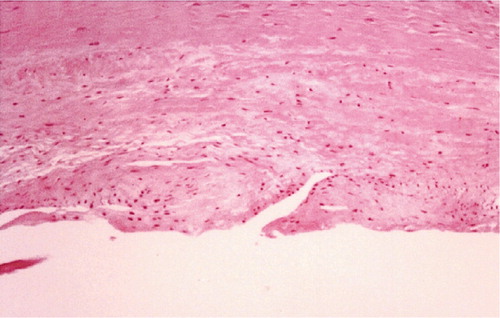
Figure 2. Type II:appearance of reactive changes in the fibrocartilage layer (enlargement of Type I and the fibocartilage layer showed proliferation. ×100).
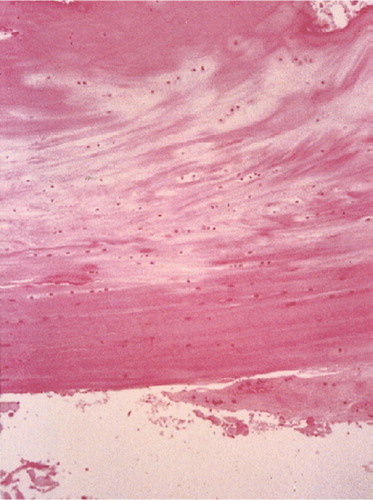
Figure 3. Type III:disappearance of the collagenous fiber layer and remaining reactive changes in the fibrocartilage layer (×100).
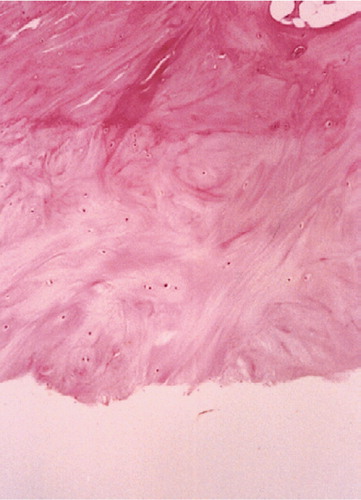
Figure 4. Type IV: disappearance of the fibrocartilage layer and exposure of the osseous layer (×100).
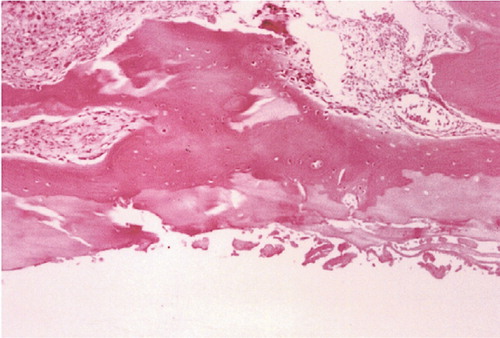
Figure 5. The relationship between the degree of degeneration on the undersurface of the acromion and the size of full-thickness cuff tear, or the history of trauma, or age. The degree of degeneration was associated with the size of full-thickness cuff tear (p < 0.05). There was no correlation between the degree of degeneration and the history of trauma (p = 0.535), or the patient's age (p = 0.123).
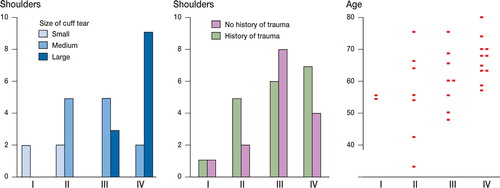
Table 2. Classification of degeneration based on pathological findings on the undersurface of the acromion.
Electron microscopic examination (TEM findings)
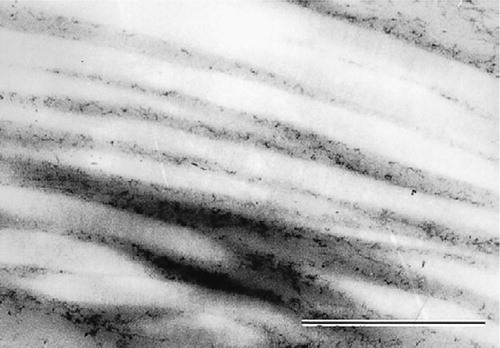
The coracoacromial ligament. In patients without cuff tear, the collagen fibers were similar to normal collagen fibers. However, the collagen fiber density decreased markedly with age, while the fiber diameter tended to be slightly increased with aging (). Similarly, in patients with full-thickness cuff tear, a reduction in fiber density and a tendency toward a slight increase in the fiber diameter with aging were noted, but there was almost no association with the size of the cuff tear.
Figure 6. The collagen fiber density was markedly reduced with aging and the fiber diameter tended to be increased slightly, but there was no change in the periodicity of banding (×36,000).
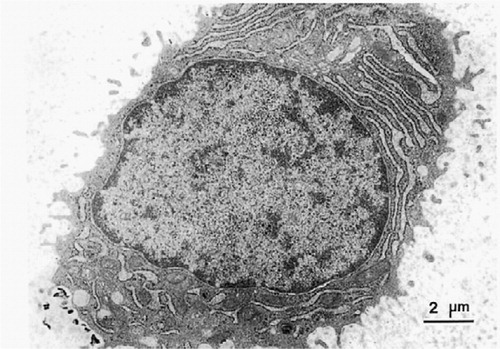
Undersurface of the acromion (fibrocartilage layer). Residual chondrocytes in the region of ligament attachment were circular, and the cytoplasm contained a fairly extensive rough endoplasmic reticulum, a moderate number of mitochondria, and a well-developed Golgi apparatus, indicating high cellular activity (). Similar findings were noted regardless of age and the presence or size of cuff tear.
Figure 7. Ultrastructure of a chondrocyte in the fibrocartilage layer showing the cytoplasm with a fairly extensive rough endoplasmic reticulum, a moderate number of mitochondria, and well-developed Golgi apparatus, indicating high metabolic activity (×4,800).
Discussion
The pathogenesis of cuff tear involves endogenous factors (Macnab Citation1973, Brewer Citation1979, Sarkar Citation1990) such as degeneration of the cuff itself and direct excessive stress on the tendon, and exogenous factors (Watson Citation1984, Gerber et al. Citation1985, Zuckerman Citation1992) such as compression of tissue surrounding the cuff. There have been few studies of the undersurface of the acromion.
Ozaki et al. (Citation1988) reported that changes in the undersurface of the acromion were secondary changes due to cuff tears. In contrast, Ogata et al. (Citation1990) stated that subacromial impingement itself induced cuff tear because pathological changes were also present in the undersurface of the acromion in patients without cuff tear. However, the findings of both studies were based on autopsy specimens. Santavirta et al. (Citation1992, Citation1993) suggested that the subacromial bursa is the source of algogenic and hyperalgesic substances that contribute to chronic shoulder pain. Soslowsky et al. (Citation1994) demonstrated changes in the coracoacromial ligament such as shortening, thickening, and reduced elasticity of the ligament in cases of cuff tear, and suggested narrowing of the subacromial space—but did not clarify whether this finding was the primary cause of the cuff tears or a secondary change resulting from cuff tears. Measurement of the pressure between the greater tuberosity of the humerus and the undersurface of the acromion by Wuelker (Citation1995) revealed that the effect of subacromial impingement was largest in the region of ligament attachment on the undersurface of the acromion. Nicholson et al. (Citation1996) demonstrated that spur formation of the anterior acromion was an age-related process; individuals younger than 50 years had less one quarter the prevalence of those older than 50 years.
We found that the synovial membrane had disappeared only in the vicinity of the region to which the coracoacromial ligament was attached, regardless of the presence or absence of cuff tear. Thus, we consider this region to undergo strong mechanical stress due to impingement. In addition, structural changes in the ligament and a decrease in the staining intensity of the elastic fibers were strongly associated with age, and we conclude that changes in the ligament were little affected by mechanical stress due to subacromial impingement. On the other hand, our TEM investigation of the coracoacromial ligament revealed that the striped bands of collagen fiber showed a periodicity similar to those observed in normal subjects (Bear Citation1944), but the diameter of the collagen fiber increased slightly with age. This observation suggests that the properties of the fiber itself may have changed.
In patients without cuff tear, type I or type II changes in the undersurface of the acromion were noted but these changes progressed with aging, suggesting the influence of degenerative changes in the undersurface of the acromion itself and the wear-and-tear (Meyer Citation1937) effect by the cuff during the symptom-free period. We believe that these changes are negligible and play a minor role in the development of cuff tear. In patients with full-thickness cuff tear, changes ranged from type I to type IV, and the influence of tear size on the degree of degeneration was more marked than the influence of age and duration of illness. Thus, we suggest that incongruity between the exposed area generated by full-thickness cuff tear and the undersurface of the acromion may facilitate degenerative changes in the undersurface of the acromion. It is unclear whether pathological changes in the acromion are the primary cause of cuff tear or whether they are a secondary change caused by a cuff tear, but we conclude that the advanced degenerative changes on the undersurface of the acromion result from a full-thickness cuff tear.
- Bear R S. X-ray diffraction studies on collagen fibers. I. The large fiber axis period ofcollagen. J Am Chem Soc 1944; 66: 1297–305
- Bigliani L U. The relationship of acromial architecture to rotator cuff disease. Clin Sports Med 1991; 10: 823–33
- Brewer B J. Aging of the rotatorcuff. Am J Sports Med 1979; 7: 102–10
- Codman E A. The shoulder. Rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. Boston 1934; 65–177, Privatery printed
- Gerber C, Terrier F, Ganz R. The role of the coracoid process in the chronic impingement syndrome. J Bone Joint Surg (Br) 1985; 67: 703–8
- Macnab I. Rotator cuff tendonitis. Ann R Coll Surg Engl 1973; 53: 271–87
- Meyer A W. Chronic functional lesions of the shoulder. Arch Surg 1937; 35: 646–74
- Neer C S. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. J Bone Joint Surg (Am) 1972; 54: 41–50
- Nicholson G P, Goodman D A, Flatow E A, Bigliani L U. The acromion: Morphologic condition and age-related changes. A study of 420 scapulas. J Shoulder Elbow Surg 1996; 5: 1–11
- Ogata S, Uhthoff H K. Acromial enthesopathy and rotator cuff tear. Clin Orthop 1990, 254: 39–48
- Ozaki J, Fujimoto S, Nakagawa Y, Masuhara K, Tamai S. Tears of rotator cuff of the shoulder associated with pathological changes in the acromion. J Bone Joint Surg (Am) 1988; 70: 1224–30
- Post M, Silver R, Sing M. Rotator cuff tear. Clin Orthop 1983, 173: 78–91
- Santavirta S, Konttinen Y T, Antti-Poika I, Nordström D. Inflamation of the subacromial bursa in chronic shoulder pain. Arch Orthop Trauma Surg 1992; 111: 336–40
- Santavirta S, Grönblad M, Antti-Poika I, Konttinen Y T, Polak J M. Protein gene product 9.5-, synaptophysin- and neuropeptide- immunoreactive nerves in human subacromial bursal tissue. Eur J Exp Musculoskel Res 1993; 2: 93–9
- Sarkar K. The ultrastructure of the coracoacromial ligament in patients with chronic impingement syndrome. Clin Orthop 1990, 254: 49–54
- Soslowsky L J, Johnston S P, Carpenter J E. Geometric and mechanical properties of the coracoacromial ligament and their relationship to rotator cuff disease. Clin Orthop 1994, 304: 10–7
- Watson M. The impingement syndrome in sportsman. Surgery of the shoulder, J E Bateman, R P Welsh. W. B. Saunders, Philadelphia 1984; 140–2
- Wuelker N. Coracoacromial pressure recordings in a cadaveric model. J Shoulder Elbow Surg 1995; 4: 462–7
- Zuckerman J D. The influence of coracoacromial arch anatomy on rotator cuff tears. J Shoulder Elbow Surg 1992; l: 4–14