
Abstract
Background
There is no report about the definition, classification and clinical epidemiological study of congenital ear malformation (CEM).
Aims/Objectives: To investigate the definition, clinical classification and distribution of a large number of CEM cases, along with the clinical and epidemiological characteristics associated with congenital malformation of the middle and outer ear (CMMOE).
Material and Methods
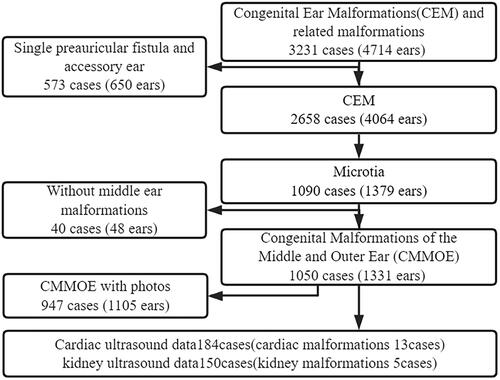
A total of 3231 cases (4714 ears) with CEM and related malformations were retrospectively analyzed, including 2,658 cases (4,064 ears) CEM and 573 cases (650 ears) preauricular fistulas and accessory ears, specifically related malformations to CEM.
Results
Among the 2,658 cases (4,064 ears) CEM, 64.9% cases were male and 35.1% were female. 52.9% cases with bilateral, 29.1% with right and 18.0% with left CEM. A subgroup of 1,050 cases (1,331 ears) was identified as CMMOE out of 1,090 cases (1,379 ears) microtia. In the CMMOE subgroup, 74.0% cases were male, 46.3% on the right side, 26.8% showed bilateral involvement. Out of the CMMOE with available images, there were 947 cases (1,105 ears). Additionally, related malformations including preauricular fistulas and accessory ears, were solely occured in 573 cases (650 ears), except for their occurrence simultaneously with CEM. The classification and distribution of CEM are as follows:
1. 2658 cases of CEM (1) 69.9% of them were confined to the ear, including: ① the outer ear 2.6%, the middle ear 17.0% and the inner ear 32.4%, ② two parts simultaneous malformations of the outer ear, the middle ear and the inner ear 17.2%, ③ three parts simultaneous malformations of the outer ear, the middle ear and the inner ear 0.6%, (2) Multiple malformations including in CEM 29.1%; (3) syndromes related to CEM 1.0%.
2. 1050 cases of CMMOE (1) 36.3% of them were confined to the middle and outer ears; (2) Multiple malformations associated with CMMOE 61.4%, including hemifacial microsomia 50.5%, accessory ears 9.8%, preauricular fistulas 9.2%, heart malformation 7.1%, and kidney malformation 2.0%; and (3) syndromes related to CMMOE 2.3%, (4) Complications of the ear 16.9%, mainly including otitis media 7.9%, outer ear canal cholesteatoma 6.3%, retroauricular abscess 1.1%, and nasal and pharyngeal complications 18.6%. The proportions of microcia grades I–Ⅴ based on the images of 1105 ears CMMOE were 5.2%, 10.5%, 74.1%, 6.9%, and 3.3%, respectively. Among the 1331 ears CMMOE, the incidence rates of outer ear canal atresia, stenosis, normal, and ossicles malformation were 86.5%, 9.9%, 3.6%, and 98.3%, respectively.
Conclusion and Significance: Approximately 69.9% of CEM cases were confined to the ear itself, with the highest proportion being inner ear malformation alone. Multiple malformations were predominantly associated with CMMOE. Syndromes related to CEM were relatively rare. Among cases of microtia, 96.3% were classified as CMMOE. These cases were predominantly observed in males, right ear and exhibited characteristics such as grade III microtia, atresia of the outer ear canal, ossicles malformation, and multiple malformations. The multiple malformations frequently included hemifacial microsomia, accessory ear, preauricular fistula, as well as heart and kidney deformities. CMMOE often coexisted with ear infections, cholesteatoma, and complications in the nasal and pharyngeal regions.
Chinese Abstract
背景:目前尚无先天性耳畸形(CEM)的分类、名称、定义及临床流行病学研究的报道。
目的:调查大量 CEM 的临床分类和分布病例以及与中耳和外耳先天性畸形(CMMOE)相关的临床和流行病学特征。
材料与方法:共对 3231 例(4714 耳)患有 CEM 及相关畸形的患者进行了回顾性分析。
结果:在 2,658 例 CEM 病例(4,064 耳)中, 观察到男性占 64.9%, 女性占 35.1%。 双耳畸形占52.9%, 右耳畸形占29.1%, 左耳畸形占18.0% 。在 1,090 例(1,379 只耳朵)诊断为小耳症的病例中, 鉴定出 1,050 个病例的亚群(涉及 1,331 只耳朵)患有 CMMOE。 在 CMMOE 亚群中, 74.0%的病例为男性。 此外, 在这些病例中, 46.3%的人出现了畸形右侧, 而 26.8% 表现为双侧受累。 在涉及 CMMOE 的具有影像的病例中, 共有947个病例(涉及1,105只耳朵)观察到相关畸形如耳前瘘管及副耳瘘。573个病例(涉及650耳)表现出这些畸形, 除非它们与 CEM 同时存在。CEM的分类及分布如下:1. 2658 个CEM病例: (1) 69.9%局限于耳部, 其中:①外耳2.6%, 中耳17.0%, 内耳32.4%, ②外耳两部分同时畸形, 中耳和内耳17.2%, ③外耳、中耳和内耳三部分同时畸形, 0.6%;(2)多种畸形, 其中CEM 29.1%; (3) 与CEM相关的综合征1.0%。2. 1050例CMMOE: (1) 36.3%局限于中耳和外耳; (2) 多个
与 CMMOE 相关的畸形 61.4%, 包括半面部短小症 50.5%, 副耳9.8%, 耳前瘘管9.2%, 心脏畸形7.1%, 肾脏畸形2.0%; 和(3)与CMMOE相关的综合征2.3%, (4)耳部并发症16.9%, 主要包括中耳炎7.9%, 外耳道胆脂瘤6.3%, 耳后脓肿1.1%, 以及鼻咽部并发症18.6%。 基于 1105 个CMMOE 耳的影像, I–V 级小耳比例分别为5.2%、10.5%、74.1%、6.9%和3.3%。 在1331个CMMOE耳中, 外耳道闭锁、外耳道狭窄、正常外耳道和听小骨畸形的发生率分别为 86.5%、9.9%、3.6% 和 98.3%。
结论和意义:大约 69.9% 的 CEM 病例局限于耳部本身, 其中单纯内耳畸形所占比例最高。 多发畸形主要是与 CEM 相关。 与 CEM 相关的综合征相对罕见。 在小耳症病例中, 96.3%被归类为CMMOE。 这些病例主要见于男性, 右耳, 并表现出III级小耳畸形、外耳道闭锁、小骨畸形和多发畸形等特征。 多发畸形常常包括半侧面部短小、耳朵附件、耳前瘘管以及心脏和肾脏畸形。这些畸形通常可观察到。CMMOE 常常与耳部感染、胆脂瘤以及鼻腔和咽部区域并发症并存。
Introduction
The ear is divided into three parts: the outer ear, middle ear, and inner ear. Congenital ear malformations (CEM) is a common birth defect. According to the latest Birth Defect Prevention and Control Report of China (2012) by National Health Commission, microtia (belongs to the outer ear) has been ranked in the top 10 among more than 8,000 birth defects for 16 consecutive years [Citation1]. In some locations, it has been reported that CEM ranked among the top 5 monitored birth defects [Citation2,Citation3]. Currently, there is a lack of comprehensive reports and standardized classification for CEM. The available data only provide partial categorization, and there is no unified nomenclature for all types of CEM. As a result, comparing literature data becomes challenging due to the lack of standardized criteria and terminology.
According to our clinical experience of more than 30 years, CEM can be divided into three categories: (1) Confined to the ear, including alone ① malformations of the outer ear, middle ear, or inner ear, ②two parts simultaneous malformations of the outer ear, the middle ear, and the inner ear, ③three parts simultaneous malformations of the outer ear, the middle ear and the inner ear. (2) Multiple malformations associated with CEM; and (3) syndromes related to CEM [Citation4]. Congenital malformations of the middle and outer ear (CMMOE) is a type of two parts simultaneous malformations of the middle ear and outer ear. It is defined as a condition characterized by a group of closely related phenotypes, primarily including microtia, outer ear canal malformation (OECM) (grading as atresia, stenosis and normal), and malformation of the middle ear. These malformations typically result in abnormalities of the ear’s appearance and hearing impairment. It may also be accompanied by multiple malformations or syndromes of other organ systems, as well as periear, nasal and pharyngeal complications. Microtia is often confused with CMMOE in the literature, and the difference between these two conditions can be clarified based on the above definitions. The treatment of CMMOE involves plastic surgery, hearing reconstruction, treatment of complications and multiple malformations (syndrome treatment is the same as multiple malformations) and psychological treatment, which covers all aspects of CEM treatment. Therefore, CMMOE is considered as a representative subtype of CEM for detailed analysis.
This paper utilizes a database comprising patients’ images, temporal bone computed tomography (CT) scans, ultrasound records, and surgical operation data from our hospital to analyze the clinical classification and distribution of CEM and the clinical epidemiological characteristics associated with CMMOE. The aim is to provide valuable insights and references for the clinical diagnosis and treatment of CEM.
Data and methods
Data
A total of 3,231 cases (4,714 ears) of CEM and associated malformations were retrospectively analyzed in our hospital from March 1993 to September 2022 for statistical analysis. Among these cases, 2,658 cases (4,064 ears) were CEM, related malformations including preauricular fistulas and accessory ears solely occured were 573 cases (650 ears), except for their occurrence simultaneously with CEM. The data of all samples are presented in .
Figure 1. Sample library combing diagram of congenital ear malformation (CEM).
Methods
A data collection table was prepared, and a sample database was established for the purpose of collecting data. The general information of patients, such as gender, age, place of birth, family history, contact number, etc, were collected. Case data included diagnosis, photos, CT of temporal bone, ultrasound, surgical information, as well as the outer, middle, and inner ear malformations, multiple malformations, syndromes, complications, et al. According to the statistical results, the clinical classification and distribution of CEM and the representative clinical epidemiological characteristics of CMMOE were analyzed.
Results
The clinical classification and distribution of CEM (percentage calculation is based on the cases)
Among the 2,658 cases of CEM (4,064 ears), it was observed that 64.9% were male and 35.1% were female, resulting in a male-to-female ratio of 1.8:1. In terms of ear involvement, bilateral ears were affected in 52.9% of the cases, while the right ear was affected in 29.1%, and the left ear in 18.0%. The distribution of the three types of ear malformations was as follows: (1) 69.9% confined to the ear, including alone in the inner ear 32.4%, the middle ear 17.0%, and the middle ear and outer ear 16.7%. (2) multiple malformations occurred in 29.1% CEM cases, among which 24.8% had malformations of both the middle ear and outer ear (including cases with CMMOE accounting for 24.3%), while 1.5% specifically had malformations limited to the middle ear, and 1.3% had malformations limited to the outer ear and (3) syndromes observed in 1.0% CEM cases. and show the overall distribution of CEM and the single, multiple malformations and syndromes.
Figure 2. The overall distribution of congenital ear malformation (CEM).
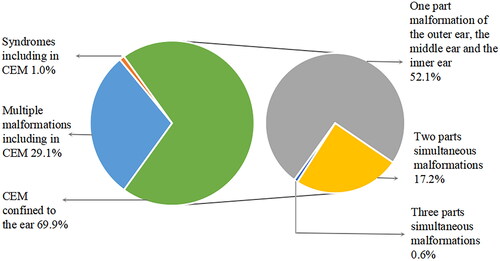
Figure 3. Classification and percentage of congenital ear malformation (CEM): confined to the ear and multiple malformations and syndromes.
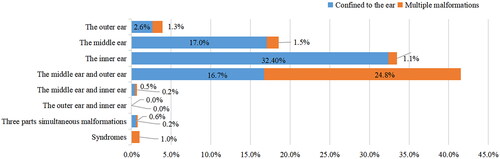
Statistical data of single, multiple malformations and syndromes, as well as the proportions of each CEM were as follows: outer ear malformations 3.9%, middle ear malformations 18.6%, inner ear malformations 33.6%, middle ear and outer ear malformations 42.4% (mainly CMMOE 39.5%), middle ear and inner ear malformations 0.7%, and outer, middle, and inner ear malformations 0.8%. Middle ear and outer ear malformations are mainly CMMOE, but also contain a few protruding ears or cup ears and middle ear malformations, and the outer ear canal and middle ear malformations.
Clinical epidemiological characteristics of CMMOE
General information
Middle ear malformations were not found among 40 cases (48 ears) out of 1090 cases (1379 ears) microtia by CT of the temporal bone, accounting for 3.7% (40/1090 cases). Out of the total 1,090 cases of microtia (1,379 ears), 1,050 cases (1,331 ears) were identified as CMMOE, accounting for 96.3% (1,050/1,090) of all microtia cases. Furthermore, these CMMOE cases accounted for 39.5% (1,050/2,658 cases) of the total CEM cases.
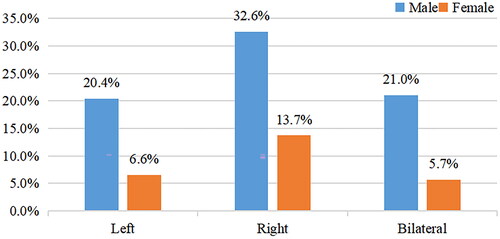
The distribution of CMMOE cases was as follows: 1) 36.3% (381/1,050 cases) were specifically confined to malformations of the middle and outer ear; 2) multiple malformations were observed in 61.4% (645/1,050 cases); 3) syndromes were present in 2.3% (24/1,050 cases), with 35.5% (372/1,050 cases) of complications. shows different lateral and gender distributions of CMMOE, it was found that 1.5% (16/1,050 cases) had a family history of the condition, 2.0% (21/1,050 cases) had a history of maternal drug use during pregnancy and 50.1% (526/1,050 cases) were between the ages of 6 and 14 years old. Furthermore, the geographical distribution of CMMOE cases was primarily concentrated in the surrounding area.
Figure 4. The distribution of general epidemiology of Congenital malformations of the middle and outer ear (CMMOE).
Main clinical manifestations (percentage calculated by the ears)
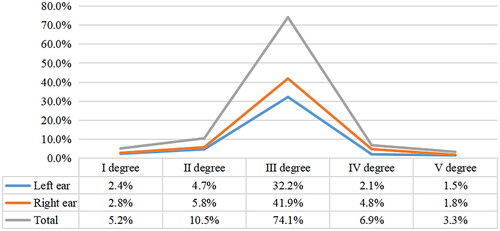
Microcia grades I–Ⅴ [Citation4] based on the images of 1105 ears CMMOE were 5.2%, 10.5%, 74.1%, 6.9%, and 3.3%, respectively (). According to the CT scan of temporal bone, surgical exploration or case description, outer ear canal abnormalities were identified in 1,050 cases (1,331 ears), with the following distribution: outer ear canal atresia 86.5%, stenosis 9.9%, and normal 3.6%, whereas ossicle malformation in the middle ear was 98.3% of CMMOE cases.
Figure 5. The distribution of microtia grades I–Ⅴ (total 1105 ears).
Multiple malformations
CMMOE accompanied by multiple malformations of other organ systems are shown in , mainly distributing around the ear, head, face, and neck. In clinical practice, it is essential to prioritize the identification and treatment of cardiac and kidney malformations as they are frequently encountered. These types of malformations require special attention and management due to their potential impact on overall health and well-being. Among the 184 cases of ultrasound examinations performed for cardiac evaluation, a 7.1% incidence rate of cardiac malformations was identified. Similarly, in the 150 cases of kidney ultrasound, a 2.0% incidence rate of kidney malformations was observed.
Table 1. CMMOE accompanied by multiple malformations of other organ systems.
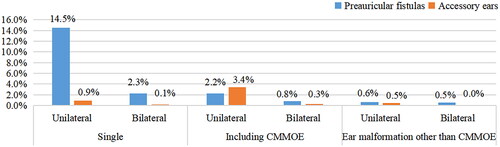
Preauricular fistulas and accessory ears are commonly found in association with CEM, but they can also occur independently. In order to analyze and compare their occurrence with CEM and when they occur alone, the cases were examined and the incidence rate was calculated based on the number of cases of CEM and related malformations (3,231 cases, 4,714 ears), as shown in .
Figure 6. The distribution of preauricular fistulas and accessory ears with/without congenital ear malformation (CEM).
Syndromes
Treacher-Collins syndrome (1.4%, 15/1050 cases) and Goldenhar syndrome (0.9%, 9/1050 cases) were the most common syndromes associated with CMMOE. Middle ear malformation was associated with one case of Alport syndrome, and inner ear malformation with two cases of Waardenburg syndrome.
Complications
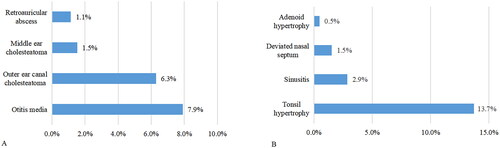
Among the cases of CMMOE (1,050 cases), complications of the ear were 16.9% (177/1,050 cases) as shown in . The incidence of specific complications is as follows: otitis media (7.9%, 83/1,050 cases), outer ear canal cholesteatoma (6.3%, 66/1,050 cases), middle ear cholesteatoma (1.5%, 16/1,050 cases) and retroauricular abscess (1.1%; 12/1,050 cases). Nasal and pharyngeal complications were 18.6% (195/1,050 cases) of CMMOE cases, as shown in . The incidence of specific complications is as follows: tonsil hypertrophy (13.7%, 144/1,050 cases), sinusitis (2.9%, 30/1,050 cases), deviated nasal septum (1.5%, 16/1,050 cases) and adenoid hypertrophy (0.5%, 5/1,050 cases).
Figure 7. Complications of congenital ear malformation (CEM).
A. Complications of the ear, B. Complications of the nasal and pharyngeal.
Discussion
The meanings of the nouns in this paper are as follows
Congenital ear malformation (CEM) alone: Refering to the malformations confined to the ear, including multiple structure abnormalities of one or more parts or single or more structures of the outer ear, middle ear, and inner ear. For example, the simultaneous auricle malformations and the outer ear canal stenosis belong to the single malformation of the outer ear [Citation4].
Multiple malformations and syndrome: Multiple malformations refer to those involving CEM and more than one other structures or organs malformation except for the ear, which can appear randomly or as some rules. Hence, different patients can have different phenotypes. Syndrome belongs to a kind of multiple malformations that appears as a specific rule and is distinguished from multiple malformations as a separate class. Therefore, the main phenotype of syndrome in different patients is similar, but the degree can be different [Citation4].
The syndromes being treated specifically in this paper: For large vestibular aqueduct syndrome, due to malformation is confined to the inner ear, we classified it as inner ear malformation in this paper. Hemifacial microsomia syndrome mainly involves maxillofacial and ear regions, which is treated as multiple malformations in the clinic currently. Therefore, the two syndromes were not counted as syndromes in this paper.
The difference between middle ear and outer ear malformations and congenital malformation of the middle and outer ear (CMMOE): The CMMOE is a kind of the former. The middle ear and outer ear malformation include in: ①CMMOE, the main symptoms are microtia, the outer ear canal malformation (grading as atresia, stenosis, and normal), and middle ear malformation. ② other auricle malformation instead of microtia in CMMOE, such as protruding ear or cup ear. ③ the outer ear canal and middle ear malformation, without auricle malformation.
Classification and distribution of CEM
In this paper, the classification and nomenclature of CEM are clearly defined, which improve uniformity and comparability within the field across international literature. Furthermore, this paper presents a comprehensive analysis of clinical and epidemiological data, providing a substantial sample size for studying the distribution of various CEM. The main clinical manifestations of CMMOE and the percentage of multiple malformations around the ear were calculated per ear. Meanwhile, the incidence of different types of CEM and other multiple malformations were computed per case, regardless of whether the disease affected one or both ears, treating unilateral and bilateral cases as a single instance.
This study shows the incidence distribution of different CEM types in a specific order, from the highest to the lowest. The most prevalent type within CEM is inner ear malformation, followed by multiple malformations associated with CEM, and then syndromes related to CEM. Among the specific types, the highest incidence is observed in middle ear and outer ear malformations, primarily classified as CMMOE. Syndromes, on the other hand, are relatively infrequent compared to other types of CEM. Overall, the highest incidence among all types of CEM is observed in CMMOE, accounting for 39.5% of cases.
The incidence rates of CEM and CMMOE were found to be higher in males compared to females. However, the maximum incidence of CEM was observed in cases affecting both ears bilaterally, accounting for 52.9% of cases. This high incidence can primarily be attributed to the presence of bilateral large vestibular aqueduct syndrome, defined as an inner ear malformation in this study. Specifically, out of a total 2,658 cases, 879 cases (33.1%) were identified as having this syndrome on both ears. As for CMMOE, the highest incidence was found on the right side, representing 46.3% of cases.
Microtia and CMMOE
Microtia is considered an essential sign for CMMOE as per the definition. While microtia is a characteristic feature of CMMOE, it cannot be classified as belonging exclusively to CMMOE. Among the total of 1,090 cases (1,379 ears) of microtia, it was found that 40 cases (48 ears), accounted for 3.7% (40/1,090 cases), did not present middle ear malformations according to CT scans of the temporal bone. Consequently, microtia was observed in 96.3% (1,050/1,090 cases) of CMMOE. Moreover, CMMOE accounts for 39.5% (1,050/2,658 cases) of all CEM cases. In this study, the malformation of the middle ear was examined by CT and/or surgical operation. In fact, it is difficult to determine by CT for slight malformation, especially for the stapes footplate, which needs to be confirmed in surgical operation. Therefore, the possibility of malformation of the middle ear cannot be completely ruled out in 40 cases (48 ears) with normal middle ear diagnosed by CT. Indeed, it is confirmed that at least 96.3% of microtia cases belong to the category of CMMOE. This observation aligns with the clinical understanding that microtia rarely occurs as an isolated condition. Furthermore, it was only 3.6% (48/1,331 ears) of CMMOE cases presented with normal outer ear canal, microtia, and middle ear malformation concurrently. This further reinforces the association between microtia and the presence of middle ear malformations within the context of CMMOE.
Clinical epidemiological characteristics of CMMOE
(1) General Information The incidence of CMMOE predominantly occurs in males and is more common on the right side [Citation5,Citation6]. We hypothesize that fetal hypoxia plays a significant role in the development of CMMOE. Additionally, we propose that male androgens can lower the rate of mitochondrial respiration and enhance sensitivity to chemical hypoxia. It has been reported that the mitochondria in the right ear mature at a later stage compared to the left side. Since mitochondria are primarily responsible for aerobic respiration in eukaryotic cells, this delayed maturation of mitochondria in the right ear may contribute to the higher incidence of CMMOE in males and the preference for the right ear [Citation4]. The age range of our patients, which predominantly falls between 6 and 14 years old, aligns with the typical timing for auricle reconstruction. In the early stages of treatment, many clinicians opt to initiate auricle reconstruction surgeries at around 6 years old to minimize potential psychological impacts on children and avoid significant disruptions to their schooling. However, our retrospective analysis indicated that the optimal time-frame for auricle reconstruction is between 10 and 15 years old [Citation4]. In this study, we found that 1.5% of the patients with CMMOE had a family history of the condition. This percentage differs from the reported rates of 9.86% and 1.2% in other studies. These variations in family history rates could potentially be attributed to factors such as ethnic differences, regional variations, and biases in data collection [Citation7, Citation8]. The history of maternal drug use during pregnancy accounted for 2.0%, and it has been reported that the uses of progesterone, Chinese herbal medicine, and nonsteroidal anti-inflammatory drugs in early pregnancy may contribute to a high incidence of microtia [Citation9]. Indeed, family history and drug use during pregnancy are important factors to consider in the study of genetic predisposition and pathogenesis of CMMOE.
(2) Main clinical manifestations The global incidence of microtia ranges from 0.8/10,000 to 17.4/10,000, especially in America, Northern Europe, Asia, Spain, and China, ranking in the top 10 among more than 8,000 birth defects in China [Citation10,Citation11]. According to the degree of microtia, we developed a 5-grade method which was specifically designed to be clear, well-defined, and easy to implement in a clinical setting. Grade III (rope, peanut, and sausage shape of auricle) was the highest 74.1% (819/1105 ears). Among the 1331 CMMOE ears, the incidence rates of outer ear canal atresia, stenosis, normal and ossicle malformation in the middle ear were 86.5%, 9.9%, 3.6%, and 98.3%, respectively. From the perspective of embryonic development, the tissues that give rise to the inner ear and the middle and outer ear are indeed different, and they develop in distinct locations. The inner ear is originated from ectodermal tissues and occurs in the R5R6 region of rhombencephalon, while the middle and outer ear are originated from migrating interlacing neural crest cells and mesodermal tissues and occurs in the R1-R4 region of rhombencephalon. This may be attributed to the fact that the clinical malformations of the inner ear often occur independently, while those of the middle and outer ear tend to occur more concurrently [Citation4].
(3) Multiple malformations The multiple malformations associated with CMMOE, ranked from high to low, were head, face, and neck (68.3%; 717/1050 cases), around the ear (26.2%; 349/1331 cases), heart (7.1%; 13/184 cases), motor system (3.9%; 41/1050 cases), genitourinary system (3.3%; 5/150 cases), eyes (1.5%; 16/1050 cases) and digestive system (0.1%; 1/1050 cases). According to the reported data, out of 3463 cases of microtia, 51.5% were found to have craniofacial malformations, and 11.0% were associated with motor system malformations [Citation8]. These findings are consistent with the results obtained in our study. Among the 1563 cases with microtia, 13.0% of them were combined with oral, facial and neck malformations, 4.4% with eye malformations, and 3.3% with musculoskeletal system malformations. This difference may be related to statistical methods, evaluation criteria and ethnic incidence [Citation12].
There are 50.5% (530/1050 cases) hemifacial microsomia and 5.1% (54/1050 cases) small mandibles, from the point of embryonic development, the first pharyngeal arch forms the upper and mandibular processes, which is related to the development of the upper and lower jaws, respectively. There is a central Meckel cartilage in the mandibular process, Human Meckel cartilage reaches full length at embryo 6th week and forms tympanae and mandibular branches at the 16th week. The end of the tympanae branch forms the incus and head of malleus. The mandibular branch is associated with the development of the mandible. Therefore, it can be inferred that CMMOE often coexists with mandibular malformations, which is considered to be one of the distinguishing features of craniofacial (or hemifacial) microsomia [Citation4].
In this study, we found that 7.1% (13/184 cases) exhibited cardiac malformations, and 2.0% (3/150 cases) had kidney malformations. These findings are consistent with another report, which indicated a similar incidence of cardiac malformations (4.8%) and genitourinary system malformations (1.7%) in a larger sample of 3463 microtia cases [Citation8]. However, there is another report where the incidence of cardiac malformations was reported to be higher (51.6%), along with a higher incidence of genitourinary system malformations (18.9%) in a smaller sample of 1563 microtia cases [Citation12]. Another study also showed that the incidence of kidney and heart malformations in microtia was higher than that in the general population [Citation13]. YiHui Zou suggests that in embryonic development, the cardiac origin tissue is adjacent to the ventral area of the inner ear and the lower area of the middle and outer ear, when the ear damage is severe and extensive, it may be complicated with heart malformations. Heart and kidney diseases pose significant risks to the overall health and well-being of patients with CMMOE. Therefore, it is crucial to prioritize the treatment of these conditions alongside ear malformations. In clinical practice, it is recommended to routinely perform preoperative ultrasonography of the heart and kidneys for patients diagnosed with CMMOE. This proactive approach allows for the timely identification of any underlying cardiac or renal abnormalities and enables healthcare professionals to address potential risks effectively.
Preauricular fistula and accessory ear are frequently observed as concomitant conditions with CEM. we examined the incidence of these conditions alone or in combination with CEM. Approximately 16.8% (542/3231 cases) of preauricular fistula occurred alone, 3.0% (97/3231 cases) were accompanied by CMMOE, and 1.1% (37/3231 cases) were accompanied by other CEM. The total number of preauricular fistulas was 676 cases, and the proportions of the three conditions were 80.2%, 14.3% and 5.5%, respectively. The incidence of the accessory ear was 3.7% (120/3231 cases), 1.0% (31/3231 cases) was accompanied with CMMOE, and 0.5% (17/3231 cases) was accompanied with other CEM. In total, there were 168 cases of accessory ears, and the proportions of the three conditions were 71.4%, 18.5% and 10.1%, respectively (). These data provide valuable insights into the incidence and co-occurrence of preauricular fistula and accessory ear with CEM.
(4) Syndrome In this study, the most common syndromes associated with CMMOE are Treacher–Collins syndrome (1.4%; 15/1050 cases) and Goldenhar syndrome (0.9%, 9/1050 cases). Middle ear malformation was associated with Alport syndrome (1 case), and inner ear malformation with Waardenburg syndrome (2 cases), indicating a low incidence of syndromes. The syndrome related to CEM can involve multiple organ systems, and its etiology and pathogenesis are complex. The current literature on CEM primarily consists of studies investigating its pathogenesis and case reports, and a few syndromes have been confirmed to have clear responsible genes. For example, the pathogenic genes of Treacher–Collins syndrome include TCOF1, POLR1D, POLR1C, and POLR1B; while those of Goldenhar syndrome include MYT1, ZYG11B, EYA3, and SF3B2 [Citation14]. The diagnosis and treatment of syndromes are complex tasks that necessitate the collaboration of highly skilled experts from various disciplines. Achieving optimal therapeutic outcomes for patients requires a multidisciplinary approach and the coordinated efforts of these experts.
(5) Complications ①The incidence of complications associated with the ear in our study was 16.9% (177 out of 1050 cases), including otitis media (7.9%, 83/1050 cases), outer ear canal cholesteatoma (6.3%; 66/1050 cases), middle ear cholesteatoma (1.5%, 16/1050 cases), and retroauricular abscess (1.1%, 12/1050 cases). In cases where there is atresia or stenosis of the outer ear canal, the infection of the outer ear canal or cholesteatoma cannot be naturally drained. As a result, the inflammation may spread through weak areas in the outer ear canal, leading to the formation of an abscess. The most common clinical abscess is retroauricular abscess, which is easily confused with local sebaceous abscess and branchial cleat abscess. CT examination of the temporal bone can be used to identify the conditions of the outer ear canal, the mastoid and the middle ear. In addition, for CMMOE patients with an infected lesion that needs to be cleared, it is crucial to carefully plan the incision to ensure the preservation of the flap blood supply for subsequent auricle reconstruction. ② The incidence of nasal and pharyngeal complications was 18.6% (195/1050 cases), including tonsil hypertrophy (13.7%, 144/1050 cases), sinusitis (2.9%, 30/1050 cases), deviated nasal septum (1.5%, 16/1050 cases) and adenoid hypertrophy (0.5%, 5/1050 cases). Nevertheless, there is currently no evidence available to establish a direct relationship between nasal and pharyngeal lesions and the malformation observed in CMMOE.
In conclusion, the extensive data collection spanning 30 years from a large hospital in China provides a valuable resource for conducting epidemiological studies on CEM. The statistical analysis provides valuable insights and serves as a reference for understanding the prevalence, distribution, and characteristics of CEM.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- China Birth Defect Prevention Report. Chinese Pharmacy. 2012; 23(39):3693.
- Li Y, Xia RM. Analysis of birth defects in 106,370 perinatal infants in Chaoyang district, Beijing. China Maternal and Child Health Care. 2017;32(01):81–85.
- Lin MF, Chen F, Ding YH, et al. 158194 cases of perinatal birth defects monitoring analysis [C]. Yangtze River delta among 2019 medical conference in Zhejiang province and among medical academic conference proceedings. [publisher unknown], 2019: p. 303. doi: 10.26914/Arthur.c. nkihy. 2019.102056.
- Zou YH. Congenital ear malformation (CEM). Acta Otolaryngol. 2023;143(S1):S3–S16. doi: 10.1080/00016489.2023.2279263.
- Paul A, Achard S, Simon F, et al. Congenital abnormalities associated with microtia: a 10-YEARS retrospective study. Int J Pediatr Otorhinolaryngol. 2021;146:110764. doi: 10.1016/j.ijporl.2021.110764.
- Liu L, Zhao XL, Wang HT, et al. A multicentric clinical study of congenital microtia and its concomitant malformation. Chin J Plastic Surg. 2020;(01). 13–19.
- Wu J, Zhang R, Zhang Q, et al. Epidemiological analysis of microtia: a retrospective study in 345 patients in China. Int J Pediatr Otorhinolaryngol. 2010;74(3):275–278. doi: 10.1016/j.ijporl.2009.12.001.
- Guo R, Wang BQ, Liu T, et al. Clinical epidemiological study of microtia and its concomitants [J]. Chinese Journal of Otolithol. 2022;20(03):409–416.
- Liu Q. Etiology, audiological characteristics and plasticity of hearing function center of congenital microtitis [D]. Beijing Union Medical College, PhD dissertation. 2019. doi: 10.27648/,dcnki.Gzxhu.2019.000183.
- Luquetti DV, Heike CL, Hing AV, et al. Microtia: epidemiology and genetics[J]. Am J Med Genet A. 2012;158A(1):124–139. doi: 10.1002/ajmg.a.34352.
- Deng K, Dai L, Yi L, et al. Epidemiologic characteristics and time trend in the prevalence of anotia and microtia in China. Birth Defects Res A Clin Mol Teratol. 2016;106(2):88–94. doi: 10.1002/bdra.23462.
- Cabrejo R, Persing J, Alperovich M. Epidemiologic assessment of microtia in over 23 million consecutive United States births. J Craniofac Surg. 2019; 30(2):342–346. doi: 10.1097/SCS.0000000000004885.
- Ramprasad VH, Shaffer AD, Jabbour N. Utilization of diagnostic testing for renal anomalies and congenital heart disease in patients with microtia. Otolaryngol Head Neck Surg. 2020; 162(4):554–558. doi: 10.1177/0194599820901351.
- Atletico M, Zhou WH. Genetic characteristics of common microtit-related syndrome in neonates. Chin J Pediatrics. 2022;4(06):614–619.