
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Back pain is associated with activity such as walking or assembly line work that involves upper-body movement. However, no single study has explored the effect of these tasks on back pain, spinal angles and balance in an older adult female population. This study investigated changes in back pain, postural sway, upper-, lower- and full-spine angle and EMG activation of trunk muscles following 30 minutes of walking and a modified quiet standing task. Fourteen older adult females (62 ± 11yrs) with low to moderate chronic back pain were recruited as participants. Findings demonstrated that following these activities, increased acute back pain and upper-spine flexion occur although acute back pain was not clinically significant; postural control and muscle activation remained unchanged. This suggests that walking and modified quiet standing can lead to subtle acute back pain in older females that could be due to an increased upper spinal flexion rather than muscle fatigue.
Practitioner summary: Back pain and postural problems are common in older adults. Older adult female participants experienced increased back pain and greater upper-spine flexion following 30-minute walking and standing with trunk rotation, but the practical importance was less clear. However, balance was unaffected, suggesting no increase in fall risk.
Abbreviations: CBP: chronic back pain; MQS: modified quiet standing; QS: quiet standing; RPE: rating of perceived exertion; TD: trapezius descendens; TT: trapezius transversalis; TA: trapezius ascendens; ESL: erector spinae longissimus; C7: seventh cervical vertebrae; T7: seventh thoracic vertebrae; T10: tenth thoracic vertebrae; T12: twelfth thoracic vertebrae; L2: second lumbar vertebrae; S2: second sacral vertebrae; AP: anterior-posterior; ML: medial-lateral; SWAYtot: total postural sway; M: mean
Introduction
It is estimated that 12.5% of UK work absences are back pain related (Bevan et al., 2012, cited in Wynne-Jones et al. Citation2014) and it has been observed that the longer an individual remains off work, the lower the probability they will return (Waddell & Burton, 2006, cited in Wynne-Hones et al. 2014). Chronic back pain (CBP) also impacts the ability to perform daily functional tasks and activities (Nordeman et al. Citation2017; Yiengprugsawan et al. Citation2017). CBP has been associated with monotonous tasks such as repetitive stationary assembly line work (Balasubramanian, Adalarasu, and Regulapati Citation2009; Coenen et al. Citation2018; Macfarlane et al. Citation1997). Similarly, acute back pain can arise during quiet standing over a period of 30 minutes to 4.5 hours, even in healthy people without chronic lower back pain (Gregory and Callaghan Citation2008; Wall et al. Citation2019; Waters and Dick Citation2015; Andersen, Haahr, and Frost Citation2007); this may also develop into chronic back pain (CBP) (Locks et al. Citation2018). A systematic review tentatively suggested a detrimental effect of prolonged standing on lower back pain, but also noted that there were a limited number of high-quality studies (Coenen et al. Citation2018). The mechanisms for back pain is therefore not yet clear and need understanding so that they can be avoided.
The task demands are an important factor to consider in the aetiology of chronic and acute back pain and the study of the causative factors would benefit employees in work environments (Claus et al. Citation2016). Moreover, older employees are at potentially greatest risk of lower back pain, due to effect of ageing; this is particularly problematic for older women (Mika, Unnithan, and Mika Citation2005; Sinaki et al. Citation2005). Thus given the increasing average age of the working population, CBP will likely become a greater problem in older female employees. However, limited occupational task constraints have been studied in older female populations.
Standing for up to 40 minutes at a time has been recommended to alleviate the detrimental effects of siting, in dominantly sedentary jobs, in an attempt to increase physical activity levels (Parry et al. Citation2019). However, given that back pain can occur during standing for 30 minutes per hour in adult workers (Andersen, Haahr, and Frost Citation2007) it may not be advisable for some. Further still, back pain has been put forward as a reason that older adults experience difficulty standing in one place for longer than 15 minutes (Edmond and Felson Citation2003), suggesting that there may be a larger effect in this specific population. This is further suggested by Freitas et al. (Citation2005), who showed that 30 minutes of quiet standing negatively impacted postural control in older adults. Along with standing, continuous walking for up to 40 minutes has been recommented to avoid sedentary working (Parry et al. Citation2019). However, researchers such as Edmond and Felson (Citation2003) found restricted ability to walk a half mile associated with back pain. The occurrence of back pain may therefore undermine the positive impact of standing and walking as older adults try and avoid pain. Similarly, the early experience of back pain in assembly line workers may make the work experience unpleasant and lead to increased pain that could make the completion of their role impossible, impacting both them and the employer. Thus, greater understanding of back pain aetiology is warranted.
Research has demonstrated increased muscle activation in the trunk muscles, including the trapezius and erector spinae muscles, during prolonged standing (Balasubramanian, Adalarasu, and Regulapati Citation2009; Madeleine et al. Citation2002). In addition, increased muscle activation of different back muscles has also been associated with back pain (van Dieën, Selen, and Cholewicki Citation2003). As such, prolonged activity such as periods of standing or walking may induce fatigue (Ament and Verkerke Citation2009; Ghamkhar and Kahlaee Citation2019), which when sufficient has been associated with back pain (Waters and Dick Citation2015). Another consequence of fatigue and pain is the adoption of different postures such as increased flexion in the upper and lower spine (Gregory et al. Citation2008; Hung-Kay Chow et al. Citation2011). Lumbar and hip flexion could be an adaptive strategy to reduce pain (Gallagher and Callaghan Citation2016; Gallagher, Campbell, and Callaghan Citation2014). Similarly, individuals who develop pain can demonstrate greater extension of their lumbosacral spine (Gallagher and Callaghan Citation2016). Potentially, the change in posture could explain the negative impact of standing and walking activity on balance/postural control too (Fewster et al. Citation2020; Garcia, Laubli, and Martin Citation2018; Ghamkhar and Kahlaee Citation2019; Walsh, Low, and Arkesteijn Citation2018), although this has not yet been explored previously.
In much of the aforementioned literature, the protocols typically do not encompass upper body motion. This is despite during stationary assembly line work, the quiet standing tasks typically involve upper body movements and axial rotational activities as part of manual handling of objects and tools (Allread, Marras, and Burr Citation2000). Upper body movement has been shown to influence the postural movement/position (Glinka et al. Citation2018). Rotational activities have also been shown to influence spinal loading and muscle recruitment (Rohlmann et al. Citation2001; Schinkel-Ivy and Drake Citation2019). Furthermore, dynamic tasks are less fatiguing than stationary tasks (Balasubramanian, Adalarasu, and Regulapati Citation2009). Within these studies, the tasks also typically involve younger adults (Balasubramanian, Adalarasu, and Regulapati Citation2009) who do not demonstrate the age-related changes that can impact posture, balance and back pain. Therefore, the use of quiet standing to evaluate fatigue has limitations to occupational task specific demands of older employees. Similarly, given the past observations that relatively short periods of standing may lead to acute back pain, understanding of the impact of incorporating upper-body movement whilst standing may be beneficial to those making recommendations to effectively limit sedentarism.
Although previous research has shown that prolonged standing and continuous walking can affect back pain, postural alignment and control, this has not been explored in a single study in older females. Further still, walking and prolonged standing have been previously evaluated separately, but not directly compared in the same population. Therefore, the aim of this study was to compare the posture, static postural control and acute back pain in older females before and after a bout of walking and modified quiet standing (MQS) comprising of repetitive manual handling requiring axial rotations. The primary hypothesis was that following MQS and walking, there would be an increase in acute pain, upper spine flexion and postural sway.
Material and methods
Participants
Fourteen older adult females (62 ± 11yrs; 162.3 ± 7.6 cm; 70.6 ± 11.8 kg), with no known neuromuscular or cognitive impairment which would inhibit stability agreed to take part in this study. The study was approved by an institutional ethics process in accordance with the Declaration of Helsinki. Each participant completed a health questionnaire and consentform to confirm their understanding of the protocol and their right to withdraw at any time without consequence. Chronic back pain using the Von Korff pain scale (Von Korff, Ormel, Keefe, & Dworkin, Citation1992) was assessed and participants were considered as having similar back pain (prior MQS median = 1 (range 1–5) and prior walking median = 1 (range 1–2)).
Experimental procedures
Participants attended a familiarisation and two test session all of which were separated by at least 48 hours (See ). Within the familarisation session, participants were given a verbal and visual description of the tasks, shown the equipment used, experienced walking on the treadmill and signed the information and consent forms. On the test occasions, participants completed a walking or MQS task, in a randomised order across participants. Within 3 minutes prior to and following these activities, five quiet standing trials were collected each lasting 30 seconds in duration. During these trials, upper body kinematics, postural control and upper body muscle activation were measured while standing in a double leg position.
Figure 1. caption. Schematic of the data collection during quiet standing trials (QS) before and after the randomised order of the modified quiet standing (MQS) and walking task allocation.
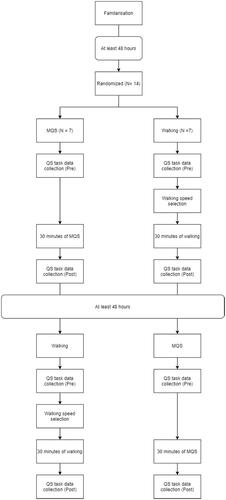
Participants completed the walking task at a self-selected pace, undertaken using a treadmill (h/p/cosmos, Germany). Participants were given a two-minute warm-up period to select their preferred walking speed and then walked in a normal fashion and without holding the treadmill support bars, for 30 minutes, modifying the speed throughout in order to maintain a sustainable walking pace (average speed of 0.92 ± 0.40 ms−1) that allows them to complete the duration of the test.
During the MQS task, participants performed a lateral rotation of the trunk at the hips, whilst keeping the feet fixed to the floor, moving weights from one plastic container to another. In total, three plastic containers (33.5 cm wide, 45 cm long 17 cm deep) were placed within easy reach from one another, on top of a table (93 cm high [55–60% of the participants’ height], 152 cm long, 79.5 cm wide); five weights were placed into one container, each weight accounted for approximately 1% of the participants body mass, to the nearest decimal. Participants moved each weight, one at a time, from one container to the next. Once all weights were moved from left to right, the process continued with the weights being moved from right to left; this process continuing for 30 minutes. During both tasks, Rating of Perceived Exertion (RPE) measured via a 10-point Likert scale was recorded at minutes 5, 15 and 25 of the activity.
In all sessions, participants wore a medical gown, which was secured using Hypafix tape (5 cm x 10 cm, Hillside Medical Supplies) to expose their posterior trunk. Reflective markers were placed at the bony processes of the cervical 7th (C7), thoracic 7th (T7), thoracic 10th (T10), thoracic 12th (T12), lumbar 2nd (L2 and sacral 2nd (S2) vertebrae; these locations were based on a modified model used previously (Fowler, Rodacki, and Rodacki Citation2006). Surface EMG activation of the Trapezius Descendens (TD), Trapezius Transversalis (TT), Trapezius Ascendens (TA) and Erector Spinae Longissimus (ESL) were recorded on both the right and left side, by wearing electrodes located and prepared in accordance with the SENIAM guidelines (Hermens et al. Citation2000); these were placed parallel to the muscle fibres.
Participants were required to stand quietly in their natural foot position with arms relaxed at their sides. Trials were performed with eyes open whereby participants were instructed to stare at a cross placed at approximately eye-height, 1.8 m from the force platform that was not adjusted during the course of the study. Foot position was noted by an outline traced around the participants' feet on an acetate sheet, fixed by sticky tape to the force platform to ensure inter-trial consistency. The number (5 trials) and length of trials (30 seconds) were based on previous research (Doyle et al. Citation2008; Letz and Gerr Citation1995; Santos et al. Citation2008) to provide sufficient data, that when averaged produces reliable CoP analysis without inducing fatigue.
Experimental measurements
Upper body kinematics were recorded using an eight-camera, 3-dimentional motion capture system (50 Hz, Eagle cameras, Cortex, Motion Analysis Corp., CA, USA). Simultaneous and synchronised force platform (AMTI, MA, USA) data were also recorded at a frequency of 50 Hz. Kinematic data was filtered using a 2nd order Butterworth filter with a cut-off frequency of 10 Hz before joint angles were calculated. Three, two-dimensional (2D) angles were calculated using motion analysis software for the upper (C7-T7-T12), lower (T10-L2-S2) and full trunk (C7-T12-S2) segments. A straight spinal position was defined as an angle of zero degrees, with increasing angles indicating any change in flexion. The average angular position of the segment was calculated for each trial.
The anterior-posterior (AP) and medial-lateral (ML) positional data provided by the force plate, were used to calculate total postural sway during the trial (SWAYTOT) utilising Equation (1):
where i = 1 and i = 3000 denote the first and last data frame and APn and MLn represent displacement for the whole sample (n).
EMG activity was recorded at a sample frequency of 1000 Hz using eight wireless transmitters (BTS FREEEMG 300, BTS Bioengineering, Milan, Italy) fitted with pre-gelled silver-silver chloride disposable electrodes with an inter electrode distance of 20 mm. The signals were amplified and A/D converted by the wireless transmitters before being transferred to EMGAnalyser software (BTS Bioengineering, Milan, Italy). Processing of all EMG signals was conducted using custom made programme written in MatLab software (Mathworks Inc., MA, USA). The raw EMG signals were bandpass filtered using a dual-pass 4th order Butterworth filter with a 20–450Hz cut-off frequency before subtracting the mean of the signal to correct baseline-offsets. The bandpass filtered signal was then full-wave rectified and low-pass filtered to produce a linear envelope using a dual-pass 2nd order Butterworth filter with a 10 Hz cut-off frequency. Mean amplitude was recorded and normalised as a percentage of peak activation level collected during a maximal back strength test conducted after the associated period of quiet standing. Maximal back strength was assessed using a back-strength dynamometer (Takei Back-D, Takei Scientific Instruments, Japan). Five measurements were taken using this equipment, with the largest EMG muscle activation used to normalise the EMG data. Finally, participants rated their acute back pain at the start and end of the prolonged walking or MQS on a 10-point Likert scale, with 10 being the worst pain possible.
Statistical analysis
Statistical analysis was performed within SPSS (IBM, version 26.0). Independent variables included Time (2 levels [before and after task]) and Task (2 levels [Walking and MQS]). For the kinematic, postural control and EMG dependent variables, the data calculated for each of the 5 trials was averaged across trials and used for the statistical analysis. Back strength was analysed using the highest value obtained with the dynamometer.
Data assumptions for parametric tests were met and subsequently, separate Two-way repeated measures Multivariate Analysis of Variance (RM MANOVA) were conducted for the spine angles and EMG data given that there were multiple sub-category of data for each dependent variable. The RPE scores collected during the prolonged tasks were analysed- using a Two-way RM ANOVA, with Time (3 levels [5, 15 and 25 minutes]) and Task (2 levels [Walking and standing]) as independent variables. Upon significant RM MANOVA, univariate analysis, provided within the SPSS output was then explored. Postural control (SWATTOT), back pain and back strength were analysed using a Two-way repeated measures ANOVA since there was only one sub-category data collected for each dependent variable.
Statistical significance was indicated at α ≤ 0.05. For significant main univariate effects and interactions, post-hoc tests were performed using Bonferroni adjustments. Group mean data, standard deviations and effect sizes were also determined. For effect size, Partial Eta Squared (ηp2) statistics were used wherein 0.02 was categorised as small, 0.13 as moderate and 0.26 as large (Cohen Citation1988).
The inter-session (using average scores provided as baseline on the two test sessions) and intra-session (using the five angles calculated on the first test session) reliability of spinal angles were assessed using a single measures and average measures two-way random ICC respectively. To interpret the reliability statistics, 0.5 or less is indicative of poor reliability 0.5–0.75 moderate reliability, 0.75–0.90 indicative of good reliability and 0.9 and greater indicates excellent reliability (Portney and Watkins Citation2015).
Standard Error of the Measurement (SEM) was calculated using the square root of the mean square error term provided from within the ANOVA table (Weir Citation2005). The SEM units are those of the data for which the SEM is calculated (e.g. degrees). This measurement provides an estimation the random variation occurring across scores, collected on multiple occasions, when no real change has taken place (Beninato and Portney Citation2011; Portney and Watkins Citation2015)
Results
Spine angle
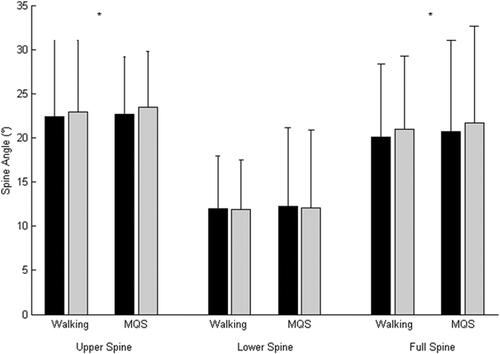
The Two-way RM MANOVA indicated a significant main effect of Time on spine angle (F(3, 11) = 6.781; p = .007; ηp2 = 0.649). The subsequent univariate analysis demonstrated greater upper (Mbefore = 22.5 degrees ± 7.54, Mafter = 23.18 ± 7.17, F(1, 13) = 11.474; p = .005; ηp2 = 0.469) and full-spine (Mbefore = 20.39 degrees ± 9.17, Mafter = 21.36 ± 9.15, F(1, 13) = 13.292; p = .003; ηp2 = 0.506) angle following the tasks; lower-spine was not significantly different (Mbefore = 12.15 degrees ± 7.42, Mafter = 12.00 ± 7.25, F(1, 13) = 1.368; p = .263; ηp2 = 0.095) (). There were no effect of Task performed (F(3, 10) = 0.318; p = .813; ηp2 = 0.080) on spine angle. There were also no significant interaction between the independent variables for any spine angle (F(3, 11) = 0.141; p = .933; ηp2 = 0.037).
Figure 2. caption. The upper, lower and full spine angles during quiet standing before (black) and after (grey) the Walking (black line) and Modified Quiet Standing task (grey line). * indicates significant increase in angle from before to after task completion.
The inter-session reliability of the upper and full spine were moderate (ICC = 0.824 and 0.672 respectively), whilst the lower spine was poor (ICC = 0.052). SEM for the upper, lower and full spine angle was 3.21, 7.63 and 5.42 degrees respectively.
The intra-session reliability for the upper, lower and full spinal angles were shown to be excellent (ICC = 0.99 for each angle). The SEM for upper, lower and full spinal angles were 0.63, 1.10 and 0.84 degrees respectively.
Postural control
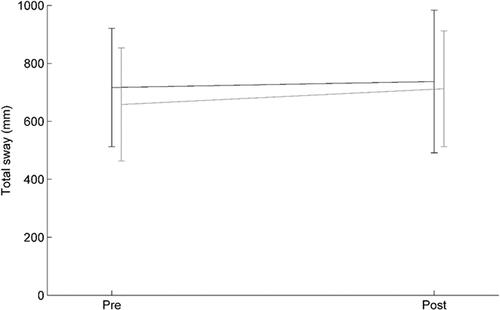
For the analysis of postural control, there were no significant main effects of Time (F(1, 13) = 1.781; p = .205; ηp2 = 0.120) or Task (F(1, 13) = 1.453; p = .249; ηp2 = 0.101) on SWAYTOT. Likewise, there was no significant interaction between Time and Task for this measure (F(1, 13) = 0.173; p = .684; ηp2 = 0.013) ().
Figure 3. caption. Total sway before and after the Walking (black lines) and Modified Quiet Standing task (grey lines).
Muscle activation
The Two-way RM MANOVA analysis of the EMG data indicated that there was no significant main effect of Time (F(8, 1) = 3.106; p = .414; ηp2 = 0.961), or Task (F(8, 1) = 1.375; p = .581; ηp2 = 0.917) (). Likewise, there were also no significant interaction between independent variables (F(8,1) = 1.312; p = .592; ηp2 = 0.913) for any EMG measurement.
Table 1. Muscle activation levels (%) during quiet standing before (Pre)and after (Post) Walking and Modified Quiet standing (MQS).
Back strength
Back strength did not change pre- and post- activity (F(1, 13) = 0.682; p = .424; ηp2 = 0.050). Likewise, the activity type did not impact maximal back strength (F(1, 13) = 0.005; p = .946; ηp2 < 0.001) (). Further still there was no significant interaction between the independent variables (F(1,13) = 0.196, p = .665, ηp2 = 0.015).
Table 2. Maximal Voluntary Contraction and Acute Back Pain during quiet standing before (Pre)and after (Post) Walking and Modified Quiet standing (MQS).
Acute back pain
Back pain change was demonstrated following the 30 minutes of activity (F(1, 13) = 8.273; p = .013; ηp2 = 0.389) where pain was higher immediately following the tasks (). Similarly, there was also a significant main effect of Task (F(1, 13) = 7.601; p = .016; ηp2 = 0.369) where pain was shown to be higher for MQS compared to Walking. However, these differences were independent of time as there was no significant interaction between the independent variables (F(1,13) = 2.116, p = .169, ηp2 = 1.40).
Rating of perceived exertion score
The RPE data collected during the activities changed over time (F(1.293, 24) = 6.970; p = .013; ηp2 = 0.367) (). RPE score increased between time points 1 and 3 (p = .043) but not between time points 1 and 2 (p = .064) or 2 and 3 (p = .164). There was no significant main effect of Task (F(1, 12) = 1.893; p = .194; ηp2 = 0.136), nor was there a significant interaction between the independent variables (F(2, 24) = 1.473, p = .249, ηp2 = 0.109).
Discussion
The main finding of the present study was that while posture changed following both walking and MQS, this did not increase the postural sway. In addition, acute back pain increased following prolonged activity, irrespective of the task. Finally, there were no changes in muscle activation, nor were any interactions observed between time and activity for any of the dependent variables, indicating that both tasks had similar effects.
The present study is the first to show that both prolonged walking and modified quiet standing with axial rotations, increased the forward flexion of the upper body during normal quiet standing in the same female older adult population. This is in agreement with previous research that has reported that walking with a backpack in young adults induced increased forward flexion (Hung-Kay Chow et al. Citation2011). In addition, in younger adults, a static, repetitive forward and vertical reaching task, performed to fatigue, induced greater forward flexion (Fuller et al. Citation2009), which is similar to the increase in flexion that occurred with axial reaching task utilised in this study. Thus, older women appear to show similar postural response to that of young adults to these activities, but without necessary the exposure duration or additional load, such as backpacks. This suggests these tasks could make older women more prone for increased forward flexion during occupational tasks, in particular if it would involve longer durations and higher loading than in the present study.
The addition of a manual handling task to quiet standing was considered appropriate to replicate typical upper-body activities associated with some employment setting. The low dexterity demands (Gilles et al. Citation2017)) and ability to self-pace could have limited the biomechanical load experienced (Claudon et al. Citation2020). This is supported by the lack of change in maximal back strength and the unchanged muscle activation in any of the muscles. Thus, it suggests that muscle fatigue of the upper body was unlikely to be a factor in the changes in spinal angles observed. Potentially, the increased forward flexion was due to other factors, such as such as the occurrence of creep in ligaments or other soft tissues (Larson, Menezes, and Brown Citation2020; Sánchez-Zuriaga, Adams, and Dolan Citation2010), or sensory feedback alterations (Pinsault and Vuillerme Citation2010).
The present study showed that acute back pain increased following both tasks which supports previous evidence from walking and standing studies (Andersen, Haahr, and Frost Citation2007); the addition of the lateral rotation also supports another study utilising repeated movements (Nelson-Wong and Callaghan Citation2010) . The increase in acute pain was also reflected in the RPE that increased from the beginning to the end of the tasks. There was higher acute pain score before and after MQS compared with prolonged walking; this may have been due to anticipation effects, rather than the development of acute back pain before that activity. Despite the change in back pain following the tasks, the magnitude of change would not be considered clinically relevant (difference of 2<for numerical rating scales) (Ostelo et al. Citation2008) and thus, it is questionable that the effect of the pain would have real world impact. Given this, after adding lateral movement of the trunk rotation to quiet standing, 30 minutes of this activity for older adults remains within the limit of safe exposure time previously suggested (Coenen et al. Citation2017). However, although not clinically relevant, it may be unpleasant for the individual and put them off from doing such activity.
The lack of effect on postural sway can be explained by the small of change in posture (≈1 degree). More rigorous, high intensity firefighting tasks, have been shown to have a significant impact on younger, healthy individuals, with (Gregory et al. Citation2008) reporting an increase in spinal flexion following the 3 minutes of these activities. Therefore, if the quiet stance task used greater load, quicker movement or of a longer duration a greater challenge on the postural system may have been experienced, increasing the postural sway experienced. In addition, the present study indicates that the inclusion of more dynamic movements during MQS could be sufficient to negate impaired postural control compared with prolonged quiet standing (Fewster et al. Citation2020; Freitas et al. Citation2005; Ghamkhar and Kahlaee Citation2019). This extends a previous finding that fatigue and pain increase less during dynamic tasks compared with static tasks and thus the effect on postural control would also be less (Balasubramanian, Adalarasu, and Regulapati Citation2009). The lack of change following walking for sway path length is also supportive of the findings of Walsh, Low, and Arkesteijn (Citation2018). Combined, it indicates that the risk of a fall was not altered, potentially by allowing the participant to move while standing in the same place and/or a low intensity task.
Macfarlane et al. (Citation1997) highlights that CBP is influenced by short term factors that are avoidable. From a practical perspective, the present study shows that older employees performing 30 minutes of repetitive stationary tasks and walking might at best increase forward flexion, but with a relatively small absolute effect; this would also be true for 30 minutes of habitual walking or activities such as washing-up or factory line work. Further still, although walking is suggested as beneficial compared to standing for reducing lower leg swelling and leg muscle fatigue (Wall et al. Citation2020), it does not appear to impact the relative change in forward flexion. These results also suggest that sedentary individuals may wish to encorporate either approach to improve their activity level without impacting posture and postural control differently. However, it will not reduce the the occurance of subtle acute back pain, which may develop over the longer term into CBP for both standing (Locks et al. Citation2018) and walking (Balasubramanian, Adalarasu, and Regulapati Citation2009; Coenen et al. Citation2018; Macfarlane et al. Citation1997). As such, regular rest periods are likely needed for activities with durations longer than 30 minutes.
A limitation of the present study is that the short exposure time to the tasks may limit the application to the full length of sustained work. Whilst some subtle changes were observed they would have likely been greater had a longer period of time been used. The degree of change would have impacted the ability to detect statistical changes. Another study limitation is the use of relatively small sample, although this was similar to other studies with less than 20 participants where differences were found during similar activities, albeit it in younger adults (Balasubramanian, Adalarasu, and Regulapati Citation2009; Fuller et al. Citation2009; Garcia et al. Citation2016; Lepers et al. Citation1997); it was expected that the older age would excaserbate the observations of younger adults and thus the power would have been sufficeint in the current study to detect change. Various large effect sizes were present, which did not consistently result in significant differences, indicative of an insufficient sample size (Johnson Citation1999; Sullivan and Feinn Citation2012). However, small effect sizes were calculated for the spinal angle data that were not significant, suggesting that greater sample recruitment would unlikely lead to ‘real’ differences being demonstrated. The population sample of older females, also limits drawing broad conclusions to male employees, as their muscle activation levels during standing have recently been found to be different (Cui et al. Citation2020). Similarly, clinical populations were not included, and therefore further research should expand the inclusion criteria. Within the sample of older adult females, heterogeneity in physiological characteristics may have impacted conclusions. Future research should take appropriate measures to either narrow inclusion criteria or explore how these factors influence the degree of change in the outcome variables studied. However, given the within subject nature of the study design, this would detract from the significant effects demonstrated in this study and the generalisation to older adults. The present study did not take into account the participant height in relation to the working height, and no ergonomic adjustable working height was selected. This could have exacerbated the forward flexion during the manual handling task for taller individuals. However, this is common in various workplaces, and the present study compared posture before and after the tasks during quiet standing poses, not during the tasks. Finally, it is important to add that whilst the intra-session reliability of the spinal angle data was excellent and the SEM values small, given the small absolute change in spinal angle this may impact the interpretation of the findings obtained.
Further research could directly compare quiet standing with modified quiet standing and allowing more movement, to determine if this could be of potential benefit to assembly line workers. Monitoring back pain during work activities also appears warranted, as the present study showed minor increased pain that may increase over a short period of time, leading to greater postural change and control impairment. Future research could focus on all day long tasks, which might exercebate the increase upper spine flexion and pain present, as well as including more physically demanding tasks and exploring the potential benefit of introducing short breaks.
To conclude, this study shows that 30-minute real-world activities such as comfortable continuous walking or repetitive work similar to that performed at a stationary assembly line impacts minimally on posture and acute back pain in older female populations. Similarly, there were no muscle activation and postural control changes suggesting that falls risk is also unaltered. Therefore, the appearance of subtle acute back pain following 30 minutes of activity is most likely due to increased upper spinal flexion, but the magnitude of the effect is not considered clinically relevant.
Acknowledgments
We acknowledge no financial interest or benefit that has arisen from the direct applications of this research.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Allread, W. G., W. S. Marras, and D. L. Burr. 2000. “Measuring Trunk Motions in Industry: Variability Due to Task Factors, Individual Differences, and the Amount of Data Collected.” Ergonomics 43 (6): 691–701. doi:https://doi.org/10.1080/001401300404670.
- Ament, W., and G. J. Verkerke. 2009. “Exercise and Fatigue.” Sports Medicine 39 (5): 389–422.
- Andersen, J. H., J. P. Haahr, and P. Frost. 2007. “Risk Factors for More Severe Regional Musculoskeletal Symptoms: A Two-Year Prospective Study of a General Working Population.” Arthritis and Rheumatism 56 (4): 1355–1364.
- Balasubramanian, V., K. Adalarasu, and R. Regulapati. 2009. “Comparing Dynamic and Stationary Standing Postures in an Assembly Task.” International Journal of Industrial Ergonomics 39 (5): 649–654. doi:https://doi.org/10.1016/j.ergon.2008.10.017.
- Beninato, M., and L. G. Portney. 2011. “Applying Concepts of Responsiveness to Patient Management in Neurologic Physical Therapy.” Journal of Neurologic Physical Therapy 35 (2): 75–81.
- Gallagher, K. M., and J. P. Callaghan. 2016. “Standing on a Declining Surface Reduces Transient Prolonged Standing Induced Low Back Pain Development.” Applied Ergonomics 56: 76–83.
- Gallagher, K. M., T. Campbell, and J. P. Callaghan. 2014. “The Influence of a Seated Break on Prolonged Standing Induced Low Back Pain Development.” Ergonomics 57 (4): 555–562.
- Claudon, L., K. Desbrosses, M. A. Gilles, A. Pichene-Houard, O. Remy, and P. Wild. 2020. “Temporal Leeway: Can It Help to Reduce Biomechanical Load for Older Workers Performing Repetitive Light Assembly Tasks?” Applied Ergonomics 86: 103081. doi:https://doi.org/10.1016/j.apergo.2020.103081.
- Claus, A. P., J. A. Hides, G. L. Moseley, and P. W. Hodges. 2016. “Thoracic and Lumbar Posture Behaviour in Sitting Tasks and Standing: Progressing the Biomechanics from Observations to Measurements.” Applied Ergonomics 53 (Pt A): 161–168. doi:https://doi.org/10.1016/j.apergo.2015.09.006.
- Coenen, Pieter, Sharon Parry, Lisa Willenberg, Joyce W. Shi, Lorena Romero, Diana M. Blackwood, Genevieve N. Healy, David W. Dunstan, and Leon M. Straker. 2017. “Associations of Prolonged Standing with Musculoskeletal symptoms-A Systematic Review of Laboratory studies.” Gait Posture 58: 310–318. doi:https://doi.org/10.1016/j.gaitpost.2017.08.024.
- Coenen, Pieter, Lisa Willenberg, Sharon Parry, Joyce W. Shi, Lorena Romero, Diana M. Blackwood, Christopher G. Maher, Genevieve N. Healy, David W. Dunstan, and Leon M. Straker. 2018. “Associations of Occupational Standing with Musculoskeletal Symptoms: A Systematic Review with Meta-Analysis.” British Journal of Sports Medicine 52 (3): 176–183. doi:https://doi.org/10.1136/bjsports-2016-096795.
- Cohen, J. 1988. Statistical Power Analysis for the Behavioral Sciences, 2nd ed. Hillsdale: Erlbaum Associates.
- Cui, A., K. Emery, A. S. Beaudoin, J. Feng, and J. N. Cote. 2020. “Sex-Specific Effects of Sitting vs Standing on Upper Body Muscle Activity during Text Typing.” Applied Ergonomics 82: 102957. doi:https://doi.org/10.1016/j.apergo.2019.102957.
- Doyle, R. J., B. G. Ragan, K. Rajendran, K. S. Rosengren, and E. T. Hsiao-Wecksler. 2008. “Generalizability of Stabilogram Diffusion Analysis of Center of Pressure Measures.” Gait & Posture 27 (2): 223–230. doi:https://doi.org/10.1016/j.gaitpost.2007.03.013.
- Edmond, S. L., and D. T. Felson. 2003. “Function and Back Symptoms in Older Adults.” Journal of the American Geriatrics Society 51 (12): 1702–1709.
- Fewster, K. M., K. M. Gallagher, S. H. Howarth, and J. P. Callaghan. 2020. “Low Back Pain Development Differentially Influences Centre of Pressure Regularity following Prolonged standing.” Gait Posture 78: e1–e6. doi:https://doi.org/10.1016/j.gaitpost.2017.06.005.
- Fowler, N. E., A. L. F. Rodacki, and C. D. Rodacki. 2006. “Changes in Stature and Spine Kinematics during a Loaded Walking Task.” Gait & Posture 23 (2): 133–141. doi:https://doi.org/10.1016/j.gaitpost.2004.12.006.
- Freitas, S. M., S. A. Wieczorek, P. H. Marchetti, and M. Duarte. 2005. “Age-Related Changes in Human Postural Control of Prolonged Standing.” Gait & Posture 22 (4): 322–330. doi:https://doi.org/10.1016/j.gaitpost.2004.11.001.
- Fuller, J. R., K. V. Lomond, J. Fung, and J. N. Côté. 2009. “Posture-Movement Changes following Repetitive Motion-Induced Shoulder Muscle Fatigue.” Journal of Electromyography and Kinesiology 19 (6): 1043–1052. doi:https://doi.org/10.1016/j.jelekin.2008.10.009.
- Garcia, M. G., T. Laubli, and B. J. Martin. 2018. “Muscular and Vascular Issues Induced by Prolonged Standing with Different Work-Rest Cycles with Active or Passive Breaks.” Human Factors 60 (6): 806–821. doi:https://doi.org/10.1177/0018720818769261.
- Garcia, M. G., R. Wall, B. Steinhilber, T. Laubli, and B. J. Martin. 2016. “Long-Lasting Changes in Muscle Twitch Force during Simulated Work While Standing or Walking.” Human Factors 58 (8): 1117–1127. doi:https://doi.org/10.1177/0018720816669444.
- Ghamkhar, L., and A. H. Kahlaee. 2019. “The Effect of Trunk Muscle Fatigue on Postural Control of Upright Stance: A Systematic Review.” Gait & Posture 72: 167–174. doi:https://doi.org/10.1016/j.gaitpost.2019.06.010.
- Gilles, M. A., J. C. Guelin, K. Desbrosses, and P. Wild. 2017. “Motor Adaptation Capacity as a Function of Age in Carrying out a Repetitive Assembly Task at Imposed Work Paces.” Applied Ergonomics 64: 47–55. doi:https://doi.org/10.1016/j.apergo.2017.04.007.
- Glinka, M., S. Metzger, D. Viggiani, and J. Callaghan. 2018. “The Effect of Task Type and Perceived Demands on Postural Movements during Standing Work.” Applied Ergonomics 69: 146–152. doi:https://doi.org/10.1016/j.apergo.2018.01.015.
- Gregory, D. E., and J. P. Callaghan. 2008. “Prolonged Standing as a Precursor for the Development of Low Back Discomfort: An Investigation of Possible Mechanisms.” Gait & Posture 28 (1): 86–92. doi:https://doi.org/10.1016/j.gaitpost.2007.10.005.
- Gregory, D. E., S. Narula, S. J. Howarth, C. Russell, and J. P. Callaghan. 2008. “The Effect of Fatigue on Trunk Muscle Activation Patterns and Spine Postures during Simulated Firefighting Tasks.” Ergonomics 51 (7): 1032–1041.
- Hermens, H. J., B. Freriks, C. Disselhorst-Klug, and G. Rau. 2000. “Development of Recommendations for SEMG Sensors and Sensor Placement Procedures.” Journal of Electromyography and Kinesiology 10 (5): 361–374. doi:https://doi.org/10.1016/S1050-6411(00)00027-4.
- Hung-Kay Chow, D., C. Kit-Fong Hin, D. Ou, and A. Lai. 2011. “Carry-over Effects of Backpack Carriage on Trunk Posture and Repositioning Ability.” International Journal of Industrial Ergonomics 41 (5): 530–535. doi:https://doi.org/10.1016/j.ergon.2011.04.001.
- Johnson, D. H. 1999. “The Insignificance of Statistical Significance Testing.” The Journal of Wildlife Management 63 (3): 763–772. doi:https://doi.org/10.2307/3802789.
- Larson, D. J., P. G. Menezes, and S. H. M. Brown. 2020. “Influence of Creep Deformation on Sub-Regional Lumbar Spine Motion during Manual Lifting.” Ergonomics 63 (10): 1304–1311. doi:https://doi.org/10.1080/00140139.2020.1774666.
- Lepers, R., A. X. Bigard, J.-P. Diard, J.-F. Gouteyron, and C. Y. Guezennec. 1997. “Posture Control after Prolonged Exercise.” European Journal of Applied Physiology and Physiology 76 (1): 55–61. doi:https://doi.org/10.1007/s004210050212.
- Letz, R., and F. Gerr. 1995. “Standing Steadiness Measurements: Empirical Selection of Testing Protocol and Outcome Measures.” Neurotoxicology and Teratology 17 (6): 611–616. doi:https://doi.org/10.1016/0892-0362.(95)00023-2.
- Locks, F., N. Gupta, D. Hallman, M. Birk Jorgensen, A. B. Oliveira, and A. Holtermann. 2018. “Association between Objectively Measured Static Standing and Low Back Pain – A Cross-Sectional Study among Blue-Collar Workers.” Ergonomics 61 (9): 1196–1207. doi:https://doi.org/10.1080/00140139.2018.1455900.
- Macfarlane, G. J., E. Thomas, A. C. Papageorgiou, P. R. Croft, M. I. Jayson, and A. J. Silman. 1997. “Employment and Physical Work Activities as Predictors of Future Low Back Pain.” Spine 22 (10): 1143–1149.
- Madeleine, P., L. Jørgensen, K. Søgaard, L. Arendt-Nielsen, and G. Sjøgaard. 2002. “Development of Muscle Fatigue as Assessed by Electromyography and Mechanomyography during Continuous and Intermittent Low-Force Contractions: Effects of the Feedback Mode.” European Journal of Applied Physiology 87 (1): 28–37. doi:https://doi.org/10.1007/s00421-002-0578-4.
- Mika, A., V. B. Unnithan, and P. Mika. 2005. “Differences in Thoracic Kyphosis and in Back Muscle Strength in Women with Bone Loss Due to Osteoporosis.” Spine 30 (2): 241–246.
- Nelson-Wong, E., and J. P. Callaghan. 2010. “The Impact of a Sloped Surface on Low Back Pain during Prolonged Standing Work: A Biomechanical Analysis.” Applied Ergonomics 41 (6): 787–795. doi:https://doi.org/10.1016/j.apergo.2010.01.005.
- Nordeman, L., L. Thorselius, R. Gunnarsson, and K. Mannerkorpi. 2017. “Predictors for Future Activity Limitation in Women with Chronic Low Back Pain Consulting Primary Care: A 2-Year Prospective Longitudinal Cohort Study.” BMJ Open 7 (6): e013974. doi:https://doi.org/10.1136/bmjopen-2016-013974.
- Ostelo, Raymond W. J. G., Rick A. Deyo, P. Stratford, Gordon Waddell, Peter Croft, Michael Von Korff, Lex M. Bouter, and Henrica C. de Vet. 2008. “Interpreting Change Scores for Pain and Functional Status in Low Back Pain: Towards International Consensus regarding Minimal Important change.” Spine 33 (1): 90–94. doi:https://doi.org/10.1097/BRS.0b013e31815e3a10.
- Parry, S. P., P. Coenen, N. Shrestha, P. O’Sullivan, C. G. Maher, and L. M. Straker. 2019. “Workplace Interventions for Increasing Standing or Walking for Decreasing Musculoskeletal Symptoms in Sedentary Workers.” Cochrane Database of Systematic Reviews (11).
- Pinsault, N., and N. Vuillerme. 2010. “Degradation of Cervical Joint Position Sense following Muscular Fatigue in Humans.” Spine 35 (3): 294–297. doi:https://doi.org/10.1097/BRS.0b013e3181b0c889.
- Portney, L. G., and M. P. Watkins. 2015. Foundations of Clinical Research: Applications to Practice (3 ed. Vol. 892). Upper Saddle River, NJ: Pearson/Prentice Hall.
- Rohlmann, A., S. Neller, L. Claes, G. Bergmann, and H. J. Wilke. 2001. “Influence of a Follower Load on Intradiscal Pressure and Intersegmental Rotation of the Lumbar Spine.” Spine 26 (24): E557–561. doi:https://doi.org/10.1097/00007632-200112150-00014.
- Sánchez-Zuriaga, D., M. A. Adams, and P. Dolan. 2010. “Is Activation of the Back Muscles Impaired by Creep or Muscle Fatigue?” Spine 35 (5): 517–525.
- Santos, B. R., A. Delisle, C. Larivière, A. Plamondon, and D. Imbeau. 2008. “Reliability of Centre of Pressure Summary Measures of Postural Steadiness in Healthy Young Adults.” Gait & Posture 27 (3): 408–415. doi:https://doi.org/10.1016/j.gaitpost.2007.05.008.
- Schinkel-Ivy, A., and J. D. M. Drake. 2019. “Interaction between Thoracic Movement and Lumbar Spine Muscle Activation Patterns in Young Adults Asymptomatic for Low Back Pain: A Cross-Sectional Study.” Journal of Manipulative and Physiological Therapeutics 42 (6): 461–469. doi:https://doi.org/10.1016/j.jmpt.2018.11.022.
- Sinaki, M., R. H. Brey, C. A. Hughes, D. R. Larson, and K. R. Kaufman. 2005. “Balance Disorder and Increased Risk of Falls in Osteoporosis and Kyphosis: Significance of Kyphotic Posture and Muscle Strength.” Osteoporosis International 16 (8): 1004–1010. doi:https://doi.org/10.1007/s00198-004-1791-2.
- Sullivan, G. M., and R. Feinn. 2012. “Using Effect Size – Or Why the p Value is Not Enough.” Journal of Graduate Medical Education 4 (3): 279–282. doi:https://doi.org/10.4300/JGME-D-12-00156.1.
- van Dieën, J. H., L. P. Selen, and J. Cholewicki. 2003. “Trunk Muscle Activation in Low-Back Pain Patients, an Analysis of the Literature.” Journal of Electromyography and Kinesiology 13 (4): 333–351.
- Von Korff, M., J. Ormel, F. J. Keefe, and S. F. Dworkin. 1992. “Grading the Severity of Chronic Pain.” Pain 50 (2): 133–149. doi:https://doi.org/10.1016/0304-3959(92)90154-4.
- Wall, R., G. Garcia, T. Laubli, R. Seibt, M. A. Rieger, B. Martin, and B. Steinhilber. 2020. “Physiological Changes during Prolonged Standing and Walking considering age, gender and standing work experience.” Ergonomics 63 (5): 579–592. doi:https://doi.org/10.1080/00140139.2020.1725145.
- Wall, R., T. Läubli, R. Seibt, M. A. Rieger, and B. Steinhilber. 2019. “Associations between Low Back Muscle Activity, Pelvic Movement and Low Back Discomfort Development during Prolonged Standing – An Exploratory Laboratory Study.” International Journal of Industrial Ergonomics 72: 380–389. doi:https://doi.org/10.1016/j.ergon.2019.07.001.
- Walsh, G. S., D. C. Low, and M. Arkesteijn. 2018. “The Effect of Prolonged Level and Uphill Walking on the postural control of older adults.” Journal of Biomechanics 69: 19–25. doi:https://doi.org/10.1016/j.jbiomech.2018.01.015.
- Waters, T. R., and R. B. Dick. 2015. “Evidence of Health Risks Associated with Prolonged Standing at Work and Intervention Effectiveness.” Rehabilitation Nursing 40 (3): 148–165. doi:https://doi.org/10.1002/rnj.166.
- Weir, J. P. 2005. “Quantifying Test-retest Reliability Using the Intraclass Correlation Coefficient and the SEM.” The Journal of Strength & Conditioning Research 19 (1): 231–240.
- Wynne-Jones, G., J. Cowen, J. L. Jordan, O. Uthman, C. J. Main, N. Glozier, and D. van der Windt. 2014. “Absence from Work and Return to Work in People with Back Pain: A Systematic Review and Meta-Analysis.” Occupational and Environmental Medicine 71 (6): 448–456. doi:https://doi.org/10.1136/oemed-2013-101571.
- Yiengprugsawan, V., D. Hoy, R. Buchbinder, C. Bain, S. A. Seubsman, and A. C. Sleigh. 2017. “Low Back Pain and Limitations of Daily Living in Asia: Longitudinal Findings in the Thai Cohort Study.” BMC Musculoskeletal Disorders 18 (1): 19. doi:https://doi.org/10.1186/s12891-016-1380-5.