
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Education is negatively associated with most major causes of death. Prior work ignores the premise that cause-specific hazards are interdependent and that both education and mortality depend on cognitive ability. We analyse Swedish men aged 18–63, focusing on months lost due to specific causes—which solves the interdependence problem—and use a structural model that accounts for confounding due to cognitive ability. In a standard Cox model controlling for Intelligence Quotient, improving education is associated with large decreases in mortality for major causes of death. In the structural model, improving education is associated with a small decrease in months lost for most causes and education levels. Among the least educated, however, improving education strongly reduces the months lost, mainly those lost from external causes, such as accidents and suicide. Results suggest that conventional analysis of education and mortality may be biased, even if accounting for observed cognition.
Introduction
Disparities in health and mortality across education groups are striking and pervasive, and are considered to be one of the most compelling and well-established phenomena in social science and social epidemiology research. It is commonly assumed that a large part of this association derives from the causal effect of education on health outcomes (Hummer and Lariscy Citation2011). For example, education may help individuals to make better use of existing medical care and choose more efficient ways to invest in their health. However, such processes may not be due to education per se but may be driven by confounding factors, such as cognitive ability or parental background, which affect both education choices and health (Mazumder Citation2008; Clark and Royer Citation2013; McCartney et al. Citation2013; Fletcher Citation2015). Because educational attainment and cognitive ability are strongly correlated, it is difficult to separate their effects on health (Auld and Sidhu Citation2005) or mortality (Deary and Johnson Citation2010). Thus, a better understanding of the influence of cognitive ability on shaping the relationship between education and mortality is needed to establish any potential direct benefits of improvements in education on mortality.
The impact of education on health is likely to differ by disease. Some diseases involve complex treatments that are easier to implement for the highly educated, while for other diseases the treatment is simple or hardly effective and, therefore, knowledge does not affect recovery. This implies that the impact of education on mortality may differ by cause of death. However, many studies on educational gains in cause-specific mortality ignore the fact that educational attainment depends on factors that also influence mortality later in life, such as parental background and cognitive ability (e.g., see Huisman et al. Citation2005; Kulhánová et al. Citation2014; Mackenbach et al. Citation2015). Ignoring such confounding in the analysis of the impact of education on cause-specific mortality will bias the estimated impact.
A common approach for investigating educational differences with respect to cause-specific mortality is to estimate a Gompertz (or Cox) proportional hazards model for each cause of death, including education as one of the explanatory variables (Næss et al. Citation2012; Elo et al. Citation2014; Kulhánová et al. Citation2014). However, the interpretation of the coefficients of education in a proportional hazards model is not obvious in the presence of competing risks, as both the total survival and cause-specific cumulative incidence functions depend not only on the cause-specific hazard but also on the hazards of all other causes. The proportional hazards model does not allow the importance of a specific cause of death in total mortality to be quantified directly.
Demographers frequently analyse life expectancy in terms of the contributions of specific causes of death, assuming that the removal of one cause of death will leave the risk of dying from the other causes unchanged (Beltrán-Sánchez et al. Citation2008). However, this method of cause-specific life years lost relies on the assumption of independent competing risks, excluding the existence of individual characteristics that have a similar impact on the mortality from different causes of death. To avoid these issues, a direct way to measure the impact of a particular covariate—education in our case—on cause-specific mortality is to estimate the months lost due to a specific cause.
Standard ‘months lost’ analysis still does not account for the possible confounding of cognitive abilities on the association between education and mortality. The method we use to account for the endogeneity of education attained and cause-specific mortality rates due to this confounding is an extension of the structural equation framework developed by Conti and Heckman (Citation2010) and Conti et al. (Citation2010) for a linear outcome; this has been extended to mortality hazards by Bijwaard, van Kippersluis, et al. (Citation2015) and Bijwaard, van Poppel, et al. (Citation2015). The model consists of three parts: (1) an ordered probit model for educational attainment depending on latent cognitive ability and childhood family characteristics; (2) potential cause-specific mortality hazards depending on the education level, latent cognitive ability, and childhood family characteristics; and (3) a measurement system for cognitive ability. We use the observed Intelligence Quotient (IQ) score as a measure of the latent, unobserved cognitive ability. The IQ score also depends on childhood family characteristics. The model allows for interdependencies between educational attainment, IQ score, and cause-specific mortality. Our approach takes a long step towards causality by removing an important part of the endogeneity bias. We acknowledge that not all of the endogeneity issue is solved. For example, there may be additional confounders, such as the personality traits (non-cognitive skills) of conscientiousness or neuroticism. However, cognitive ability has been shown to be an important determinant of both education and health, and therefore accounting for this confounder in a rigorous way is still an important improvement. Based on the parameter estimates of such a structural model, the educational gain for a specific cause of death is defined as the decrease in the implied number of months lost from age 18 to age 63 from a specific cause of death by improving the level of education.
Data from the Swedish Military Service Conscription Register (for men born 1951–60), linked to Swedish administrative registers, offer the opportunity to investigate the impact of education on cause-specific mortality; see Bijwaard et al. (Citation2017) for more information on these data. Nearly all men were conscripted because at that time military conscription was mandatory in Sweden. We have information on about half a million men who are followed from the date of conscription up to the end of 2012 or until their death. For those men who die, we observe the cause of death and categorize these into four categories: neoplasms (cancers), cardiovascular diseases, external causes, and ‘other’ causes of death. We distinguish four levels of education, running from less than ten years of education to university education. In the analysis we control for the childhood family characteristics of the men. From an intelligence test consisting of four subtests conducted at the military examination, we also observe the IQ scores in nine categories. The empirical results show that achieving the next highest education level could result in between two and nine additional months alive between ages 18 and 63 (nine for the least educated group). The men with the lowest levels of education could gain the most from educational improvement, with a reduction in external causes of death (seven months). They could also gain from a reduction in cancer mortality (one month) and a reduction in mortality from ‘other’ diseases (one month). Although standard Cox proportional hazards analysis shows large educational gains in cardiovascular mortality, we find that the educational gain in cardiovascular mortality is small, mainly due to accounting for cognitive ability. However, the implied educational gains due to external causes of death are larger in the structural model than standard Cox analyses would suggest.
Previous research and conceptual framework
Educational attainment is the most commonly used indicator of socio-economic status in studies of health and mortality (Hummer and Lariscy Citation2011). There are several reasons for using education as our measure of socio-economic status (Hummer et al. Citation1998; Preston and Taubman Citation2011). First, education is usually completed by early adulthood, hence educational attainment remains constant over the life course. Second, educational attainment precedes other dimensions of socio-economic status, such as income, occupation, and the accumulation of wealth (Mirowsky and Ross Citation2003). Third, income and occupation may often be affected by health fluctuations, while educational attainment is less prone to such issues of health endogeneity (Smith Citation2004). Fourth, education is likely to be more relevant than other measures of socio-economic status for individuals who are retired, unemployed, or out of the labour force. Finally, when using survey data, missing information on educational attainment is much less of an issue in comparison with income and occupation.
Many studies focusing on the educational gradient in health and mortality measure educational attainment with a single indicator of years of completed schooling, assuming that each additional year of education confers a monotonic increase in health (Elo and Preston Citation1996; Lynch Citation2003). Some other studies suggest that the relationship is not monotonic but is instead a step function that reflects levels reached (Backlund et al. Citation1999; Montez et al. Citation2012). We agree with that view and, like them, base our analyses on distinct levels of education (four).
Cause-specific mortality
Evidence suggests differential impacts of education on various diseases, resulting in different educational cause-specific mortality gradients (Galobardes et al. Citation2004). The associations for cardiovascular diseases appear to be stronger than for total mortality (Kulhánová et al. Citation2014). The main reason for this is that low education has been linked to cardiovascular risk factors, such as smoking, hypertension, and overweight. For cancers the educational gradient varies by cancer type (Galobardes et al. Citation2004; Kulhánová et al. Citation2014). Higher lung cancer mortality among those with low levels of education is clearly related to the higher prevalence of smoking among these individuals. The relationship between education level and the mortality rate for other cancers is more complex. Lifestyle differences, such as physical inactivity, might be one reason for this.
External causes, including traffic accidents, injuries, and suicides, are a major cause of early death and are also associated with education attained (Borrell et al. Citation2005; Lorant et al. Citation2005). For traffic accidents the educational gradient may be explained by differences in exposure, such as differential use of protective devices, as well as differences in susceptibility. Educational differences in mental illness, which is more prevalent among those with a low level of education, may partially explain the educational gradient in suicides. Note that this association may also be induced by joint confounding factors that explain both education and mental health (Halpern-Manners et al. Citation2016).
Cognitive ability
Understanding the doctor better and adhering to complex treatments may be driven by cognitive ability rather than education (Gottfredson and Deary Citation2004). It is obvious that cognitive ability influences educational attainment, and it has been established that a strong correlation exists between cognitive ability and health outcomes (Auld and Sidhu Citation2005; Cutler and Lleras-Muney Citation2008; Kaestner and Callison Citation2011). Intelligence, measured by some form of IQ test(s), is also associated with health outcomes (Gottfredson Citation2004; Deary Citation2008; Batty, Wennerstad et al., Citation2009) and mortality (Batty, Deary, et al. Citation2007; Batty, Wennerstad, et al. Citation2007; Batty, Gale, et al. Citation2009; Batty, Wennerstad, et al. Citation2009; Calvin et al. Citation2011).
Performance on an IQ test certainly depends on cognitive ability but also on other personal characteristics, such as family background. Using a factor model (Anderson and Rubin Citation1956)—which assumes that performance on one or more IQ tests is driven at least in part by a common unobserved (latent) factor (cognitive ability)—allows us to estimate the impact of education on cause-specific mortality while taking into account that cognitive ability influences both educational attainment and mortality. Recent papers by Conti and Heckman (Citation2010), Bijwaard, van Kippersluis, et al. (Citation2015), and Bijwaard, van Poppel, et al. (Citation2015) have also used this concept of measuring cognitive ability based on IQ scores. While cognitive ability cannot be measured directly, it accounts for measurement error in IQ scores and for the impact of childhood family characteristics on IQ scores. Note that we do not include the IQ score directly in the education equation, nor in the cause-specific mortality hazards. We use the IQ score to measure the latent cognitive ability, which we include in the education equation and the cause-specific mortality hazards.
Causal inference
In the literature three different approaches have been used to examine the causal effects of education on health and mortality. The first approach exploits changes in compulsory schooling policies, usually increases in the minimum age or the legally permitted grade for leaving school, as instrumental variables for schooling attainment to control for endogeneity, that is, an uncontrolled confounder affects both the education attained and the mortality. The estimates based on these studies point towards a small effect (Lleras-Muney Citation2005; van Kippersluis et al. Citation2011; Meghir et al. Citation2018) or even an entirely absent causal effect (Arendt Citation2005; Albouy and Lequien Citation2009; Clark and Royer Citation2013) of education on health outcomes. However, a major limitation of using changes in compulsory schooling to detect education effects on health outcomes, and in particular mortality, is that often only a relatively small part of the population is affected by the changes (Mazumder Citation2008; Fletcher Citation2015). Another issue with the instrumental variable methods applied in these studies is that they implicitly assume that the compulsory schooling reforms only affect long-term health through their effect on education, ignoring any other contemporary policy changes that may have accompanied these reforms.
A second identification strategy is to use variation in education among siblings, often identical (monozygotic) twins, to distinguish the unobserved factors shared by these siblings. These studies obtain estimates of the impacts of the differences in schooling within a pair of identical twins on their health differences at various schooling levels. Results from such studies have indicated that part of the educational differences in cause-specific mortality disappears when accounting for shared family background (Behrman et al. Citation2011; Næss et al. Citation2012; Lundborg Citation2013; Amin et al. Citation2015). Although by using twins it is possible to control for both shared environmental and shared genetic factors, a major shortcoming of twin studies is that they only analyse twins; yet twins are usually not representative of the whole population. Using twins will substantially reduce the statistical power, because only twins with different levels of education are analysed. Not only is it uncommon for twins to have the same cognitive ability, they also experience a large number of non-shared events throughout life; events that may be unobserved and influence both education and mortality (e.g., accidents).
A third approach, which we will use, is based on structural models in which the interdependence between education, health, and cognitive ability is explicitly modelled. Results from such models for health outcomes (Conti and Heckman Citation2010; Conti et al. Citation2010) or for total mortality (Bijwaard, van Kippersluis, et al. Citation2015; Bijwaard, van Poppel, et al. Citation2015) have shown that at least half of the health disparity across education groups is due to the selection of healthier, more able individuals into higher levels of education.
The contribution of this paper is that we develop a new method for estimating the educational gain in reducing cause-specific mortality. The innovative aspects of our method are twofold. First, contrary to the standard literature, we define the educational gains in terms of months lost due to a specific cause of death instead of using the hazard ratio. The ‘months lost’ measure is easier to interpret, additive, and not prone to issues of independence (see next section). Second, in the analyses we account for confounding of the effect of education due to omitted cognitive ability. To this end we extend the structural all-cause mortality model of Bijwaard, van Kippersluis, et al. (Citation2015) to cause-specific mortality.
Methods
The main issue with using the commonly applied Cox proportional hazards model to investigate the educational gradient in mortality separately for each cause of death is that it assumes that the competing causes of death are independent. This implies that the removal of one cause will leave the risk of dying from the other causes unchanged. However, the cause-specific hazard gives the mortality rate due to a particular cause, conditional on not having previously died from any other cause. Caution is needed when interpreting these results because a particular covariate can appear in several competing hazards (Thomas Citation1996). Even the sign of the effect of education is unclear, because both the total survival and the cause-specific cumulative incidence functions depend not only on the cause-specific hazard, but also on the hazards of all the other causes. In addition, the Cox competing risk models provide information only on the magnitude of the educational disparity, not on the importance of the specific cause.
Estimating Cox models with IQ scores included in the controls also ignores the premise that IQ affects not only mortality but also educational attainment. Using multivariate regression techniques is not sufficient to control for such endogeneity, as those methods do not account for selective educational attainment. Another problem is that the effect of the control variables on cause-specific mortality may differ by educational attainment. Even if this is accounted for, such control function solutions to the selection problem are very sensitive to differences in the distribution of the control variables between the least and most highly educated groups; see Imbens (Citation2004). The structural model defined later in this section and in the supplementary material (Section A1) accounts for such confounding.
Months lost due to a specific cause of death
Another measure of the mortality experience is the number of months lost due to a specific cause of death. This quantity is easier to interpret and avoids the issues of independence in competing risks proportional hazards models; see Andersen (Citation2013) and Andersen et al. (Citation2013). The ‘months lost’ formulation explicitly accounts for dependence of the competing causes of death because the ‘months lost’ to each cause of death is the integral of the cumulative incidence, the probability of dying from a specific cause before some given time, which in turn depends on the mortality rate from each cause of death. The months lost can be defined over the whole age distribution or over a segment of the age distribution, for example, the number of months lost before age 63 (as we will use). Based on the months lost we define the educational gain as the decrease in months lost (from a specific cause of death) when improving the level of education. A useful feature of the ‘months lost’ quantity is that it is an additive measure. The sum of months lost over all alternative causes of death within one level of education is equal to the total number of months lost for that education level. The sum of educational gains over all education levels within a cause of death is equal to the total educational impact for that cause of death. The months lost can be calculated based on estimated hazard coefficients, the implied total survival, and the cumulative incidence functions.
Structural model
Still, this does not account for possible confounding of cognitive abilities, affecting both educational attainment and cause-specific mortality. The method we use to account for this endogeneity is an extension of the structural equation framework developed by Bijwaard, van Kippersluis, et al. (Citation2015) and Bijwaard, van Poppel, et al. (Citation2015). The model consists of three parts: (1) an ordered probit model for educational attainment; (2) potential cause-specific mortality hazards; and (3) a measurement system for cognitive ability.
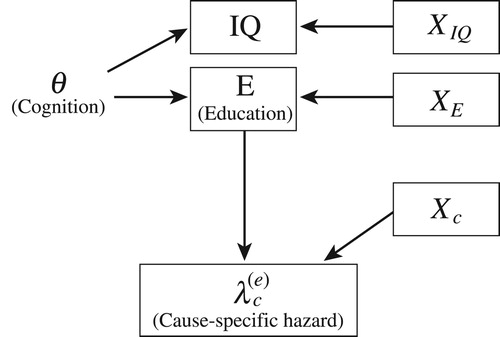
Figure 1 Graphical representation of the structural model on education, cognitive ability, and cause-specific mortality
Notes: Latent cognitive ability, θ, influences the individual education attained, E, and the (potential) cause-specific hazard, , for each cause, c, and each education level, E = e. Educational attainment and the cause-specific hazard also depend on observed covariates XE or Xc. The IQ measurement, IQ, depends on the latent cognitive ability and on observed covariates XIQ. Note that XE, Xc, and XIQ may overlap or even be the same.
The intuition of the structural model is as follows:
(1) Ordered probit model. In our model, as in standard discrete choice models, we assume that individuals implicitly evaluate the expected consequences of future choices and their costs, including both monetary and psychic costs, to decide whether to continue their schooling. We are agnostic about the decision model used by the individuals and do not observe the cost of education, just like most of the treatment evaluation literature. We do not impose rational expectations. The decision is influenced by unobserved cognitive ability. Conditioning on cognitive ability accounts for all the dependence across educational choices and cause-specific mortality. We assume that the value of cognitive ability is known by the individual but not by the researcher and that it is fixed at the moment an individual makes their schooling and behavioural choices. shows the structure of the model.
Let E* denote the (latent) net utility of an individual choosing a particular level of education. We assume that the educational choice is endogenous and that selection into schooling is fully accounted for by the individual’s observed characteristics, X, their latent cognitive ability, θ, and the underlying latent utility of choosing a particular level of education. We assume a linear model for the net utility of each schooling level, E* = γ′X + αEθ + νE, with νE being an unobserved random variable also affecting utility, which is assumed to be statistically independent of both X and θ. The indicator of education, E, takes the value e if the individual has attained the given level of education, with E = 1, … , 4: E = e if ζe
−1 < E* ≤ ζe where ζ0 = −∞ and ζ4 = ∞. We assume that νE is normally distributed, therefore we have an ordered probit model for educational attainment. Therefore, the probability that an individual has attained education level e, Pr(E = e) is given by:(1)
(1) with Φ(·) as the standard normal cumulative density.
Once the individual has decided their level of education, future mortality is potentially causally related to this decision. More importantly, the model allows individuals to select their schooling level, anticipating future mortality differences by education level. This implies that individuals select their schooling level by comparing (future) outcomes by schooling level. To deal with the issue of schooling choice based on future outcomes, we use potential outcome models in which we allow observed and unobserved variables (unobserved from the research point of view, but known to the individual) to be correlated across schooling levels and (cause-specific) mortality rates. This model is a Roy-type model (Roy Citation1951), commonly applied in economics to model choices based on potential outcomes.
(2) Potential cause-specific hazards. A common characteristic of mortality studies is that not all individuals experience death during the observation period. Such right-censoring makes inference based on means unreliable. Another issue is that, due to dynamic selection, those still alive at age 18 (the time they are observed at the military examination) may not be a random selection of the original population of those born 18 years earlier. We therefore model the cause-specific mortality hazard as this effectively deals with these data issues. The second part of the structural model comprises the potential cause-specific mortality hazards, , with e = 1, … , 4 and c being the cause of death. These hazard rates are potential outcomes because for each individual the cause-specific mortality is only observed for the actual level of education the individual has chosen and not for the potential alternative education levels. The model assumes that each individual compares the potential hazards
, … ,
for each cause of death, c, when choosing schooling level. For all but external causes of death we assume a Gompertz proportional mortality rate, which assumes an exponential increase in cause-specific mortality by age. We tested age dependence of death due to external causes and rejected it. A Gompertz mortality rate is known to provide accurate mortality rates for middle-aged individuals (Gavrilov and Gavrilova Citation1991). Specifically, the potential hazard of dying from cause c at age t for education level e is:
(2)
(2)
The shape of the hazard is captured by ηec, which is equal to zero for deaths due to external causes, and the scale of the hazard by the parameters βec0, which all depend on the education level and differ by cause of death. The effect of latent cognitive ability on the hazard is captured by αec. Note that we do not control for personal characteristics such as marital status, income, or occupation in the hazard rates, because these variables are on the pathway from education to cause-specific mortality.
(3) Measurement system for cognitive ability. The structural model is closed by measurement equations for cognitive ability (θ), linking intelligence (IQ scores) with latent cognitive ability and observed individual characteristics. We assume that the IQ measurements are normally distributed with:(3)
(3) where νIQj is normally distributed with mean zero and variance
. For identification we need at least three intelligence tests, J ≥ 3 and αIQ1 = 1. We use the four available subtests from the military examination: the logical test, the technical test, the verbal test, and the geometrical test. We use a maximum likelihood estimation method to estimate all the parameters of the model. Thus, we jointly estimate the parameters of educational attainment, the cause-specific mortality hazards, and the measurement equation. We explain this method in more detail in the supplementary material (Section A1).
Based on the parameter estimates, the educational gain for a specific cause of death is defined as the average difference from improving one education level in the implied number of months lost from age 18 to age 63 (the maximum observed age range) for a specific cause of death. We explain this method in more detail in the supplementary material (Section A2).
Data
The data come from several Swedish population-wide registers, which are linked using unique individual identification. The Swedish Military Service Conscription Register includes demographic information on the conscripts and information obtained at the military examination, including a battery of intelligence tests. We linked these data to information on their parental socio-economic situation at birth, parental education, and the individual’s own education, date of death, and cause of death. The data consist of the population of men born between 1951 and 1960, who were enlisted between 1969 and 1980, sometime between ages 18 and 20. Military service was mandatory for men but not for women. We selected only the 459,682 men for whom at least one parent was known and who had a known conscription date. Then we removed 5,859 men with missing education level; however, those with missing data on parental education and socio-economic position were not removed but included as separate categories in the analysis. Finally, we also removed 7,278 men without an IQ measurement. We ended up with 446,545 men.
We aggregated the observed education into four classes: (i) compulsory (less than ten years of education); (ii) some secondary education (two additional years); (iii) full secondary education (three additional years); and (iv) post-secondary education (university degree or PhD). In our sample 21 per cent belonged to the least educated group, 36 per cent had acquired some secondary education (maximum twelve years’ education in total), 12 per cent had full secondary education (maximum 13 years’ education in total), and 30 per cent had completed at least three years at university. The IQ measurement is based on a battery of IQ tests, which consisted of four subtests that measured logical, spatial, verbal, and technical abilities. Each subtest was first evaluated on a normalized nine-point (stanine) scale. The subtest scores were summed to obtain an overall score and transformed onto a stanine scale with a mean of five and standard deviation of two. In the analysis we assume that the scores from these tests are close to continuous.
presents selected demographic and childhood family characteristics at the time of military examination, by conscripts’ level of education. We see a clear positive relationship between maternal socio-economic status, paternal education, and the education attained by the military conscript. The higher the social class and education of the parents, the higher the level of education of the conscript. The average IQ score at age 18 also clearly increases with education attained.
Table 1 Sample characteristics, Swedish conscripts born 1951–60 (N = 446,545)
We aggregated the causes of death into four categories, using the International Classification of Diseases (ICD). The four categories are: (1) neoplasms, all kind of cancers (ICD8 and ICD9 140–240, ICD10 C0–D490: of which 22 per cent digestive cancer, 13 per cent lung cancer, 12 per cent bowel cancer); (2) cardiovascular diseases (ICD8 and ICD9 390–460, ICD10 I: of which ischaemic heart disease 53 per cent and stroke 15 per cent); (3) external causes (ICD8 and ICD9 E800–E999, ICD10 V–Y: of which suicide 43 per cent and traffic accidents 20 per cent); and finally (4) ‘other’ (natural) causes of death (of which psychiatric diseases 17 per cent, liver diseases 14 per cent, nervous system diseases 10 per cent). We list suicide as an external cause of death because it is not a natural cause. The death ratios (number of deaths per 1,000 men up to the end of the observation period, 31 December 2012) differ by level of education and by cause of death. For all four causes of death we observe a clear educational gradient, but much less for neoplasms. For the two groups with the highest education, mortality due to neoplasms is the most important cause of death, while for the two groups with lower education, external causes are more important.
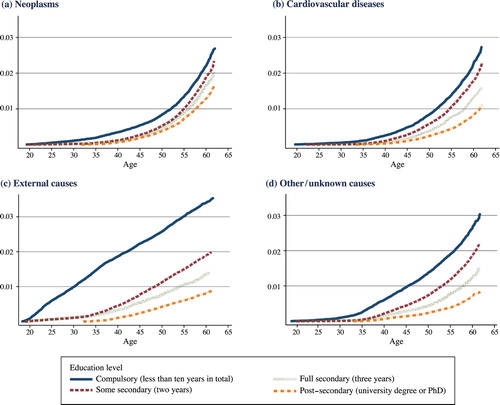
To take the timing of the deaths into account, we also calculated the cumulative incidence functions (the probability of dying from a specific cause of death before a specific age). The (non-parametric) Aalen–Johansen cumulative incidence functions (Aalen and Johansen Citation1978) depicted in show again a clear educational gradient in the probability of dying from each of the four causes of death. They also show that external causes of death, such as traffic accidents, suicides, and homicides, play a major role in the early mortality of the least educated. For this group, the cumulative incidence function for external causes of death is close to linear, indicating little age dependence in the hazard of dying from external causes.
Figure 2 Cumulative incidence curves by level of education for (a) neoplasms, (b) cardiovascular diseases, (c) external causes, and (d) ‘other’/unknown causes; Swedish conscripts born 1951–60
Source: Authors’ calculations based on Swedish Military Service Conscription Register linked to Swedish administrative registers.
Results
Before we turn to discuss the educational gains in reducing months lost to mortality, we first estimate educational differences in cause-specific mortality rates using Cox proportional hazards models, the common approach taken in the literature (Elo et al. Citation2014; Kulhánová et al. Citation2014). Later in this section we discuss the results from our structural model.
Standard Cox proportional hazards analysis
Most studies of educational differences in cause-specific mortality using Cox models report the hazard ratio of each education dummy on the cause-specific hazard. In our case this would correspond to estimating the hazard ratios for some secondary education (two years), full secondary education (three years), and post-secondary education, for each of the four causes of death considered. To relax the assumption of common age dependence, we estimate separate models for each of the three adjacent education levels: some secondary education (two years) vs. compulsory; full secondary education (three years) vs. some secondary education (two years); and post-secondary education vs. full secondary education (three years). In each of these models we estimate the hazard ratio for the higher of the two education levels (). This makes comparison of these results with the results from the models for ‘months lost’ analyses easier. Note that estimation of a joint Cox model with three education dummies does not change the conclusion on the educational gradient in the cause-specific hazards. The estimated hazard ratios of full secondary education and post-secondary education in a joint model are close to the product of the odds ratios in (2)–(3) and (2)–(4) in . When accounting for IQ differences, the joint Cox models give slightly smaller education effects than when not accounting for IQ.
Table 2 Cox proportional hazards odds ratios of education on cause-specific mortality, Swedish conscripts born 1951–60, ages 18–63
The results in show that across all causes of death, higher levels of education are associated with reduced mortality hazards, with the strongest association for the hazard of dying from external causes. The smallest associations are found for cancer mortality, consistent with the view that the risk of getting cancer is less affected by healthy lifestyle, except for lung cancer, and that the effectiveness of cancer treatment is less influenced by the knowledge of the patient. Controlling for childhood family characteristics hardly affects this association with education, but additionally accounting for differences in intelligence, as measured by the IQ score, changes the education association for half of the causes of death. Including the IQ score in the controls reduces the estimated association with education for cardiovascular diseases and ‘other’ causes of death, but only by a very small amount.
Months lost due to a specific cause: results from the structural model
When estimating the structural model, we include the following observed childhood family characteristics: mother’s socio-economic status around birth, father’s education, age of mother at birth, birth order, and birth year dummies. For most causes of death and levels of education, higher cognitive ability reduces the hazard of dying. However, cognitive ability significantly reduces the risk of dying from cancer only for men with two years of secondary education. This reflects the premise that higher intelligence has little influence on cancer survival. For the least educated group death due to external causes increases with cognitive ability. Not surprisingly, cognitive ability is positively related to the education attained (in the educational choice equation) and the IQ score (in the IQ measurement equations). The full table of estimated coefficients is given in Table B2 in the supplementary material.
Based on the estimated coefficients of the structural model, we calculate the average number of cause-specific months lost from age 18 until age 63, as well as the implied educational gains (). For the least educated group, 55 per cent of the ‘months lost’ up to age 63 is due to external causes, such as traffic accidents and suicides, while this drops to 40 per cent among the other education groups. Although the amount of time lost due to cancers decreases with education level, its relative importance increases, from 17 per cent for the lowest level of education to 26 per cent for the men who went to university. The number of months lost to death by cardiovascular diseases and to ‘other’ diseases both show an educational gradient, although their relative importance in the total time lost by education level is rather stable.
Table 3 Months lost and educational gain (at ages 18–63) by cause of death and level of education, structural model, Swedish conscripts born 1951–60
The educational gains are the largest for external causes: we estimate an educational gain of seven months from a reduction in mortality due to external causes when comparing men who have some secondary education with those with only compulsory education, which is 75 per cent of the total gain. All the other educational gains are around one month or smaller except for the gain in cancer survival for those with the lowest level of education. For example, the educational gains for cardiovascular diseases are only 0.3–0.6 months for each increase in education. This rather low impact of education on cardiovascular mortality is probably because we can only follow the conscripts up to age 63, which is before most heart attacks occur. The same holds for cancer mortality.
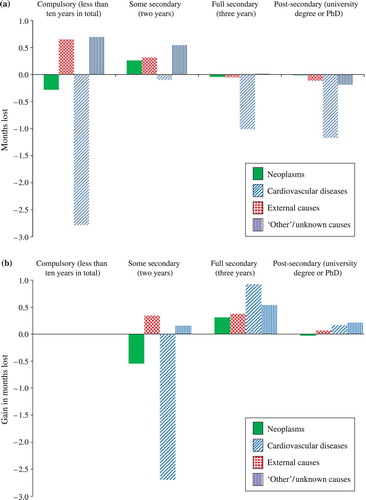
We also estimate the implied months lost and educational gains based on the estimation results from the Cox models. In we compare both the estimated months lost by cause of death and education level and the implied educational gains of improving the education level based on the structural model (in ) with the implied estimated months lost and educational gains based on the estimated Cox models that account for childhood family characteristics and the IQ score (estimated hazard ratios in ). (a) shows that the estimated Cox models, which ignore the premise that the childhood family characteristics and cognitive ability also affect the education attained, imply a lower number of months lost between ages 18 and 63 for the two more highly educated groups. They show a higher number of months lost for the lower two education groups, except for external causes and for neoplasms among the least educated. We obtain the largest differences between the educational gain implied by the Cox model and the structural model for deaths due to external causes ((b)). The total implied educational gain for the men with the lowest level of education is also lower when using Cox models than structural models, but higher for the other two education levels. This is mainly caused by differences in educational gain for external causes.
Figure 3 (a) Months lost and (b) educational gains (at ages 18–63): differences between Cox model and structural model, Swedish conscripts born 1951–60
Notes: (a) The difference in months lost by education level for the Cox model compared with the structural model, where a positive value indicates that the Cox model overestimates the months lost. (b) The difference between the Cox model and the structural model in the implied educational gains in reducing the number of months lost by improving the education level, where a positive value indicates that the Cox model overestimates this educational gain. See for the results from the structural model.Source: As for .
Conclusion and discussion
Prior research has documented a strong negative association between education and mortality for most major causes of death (Huisman et al. Citation2005; Kulhánová et al. Citation2014; Mackenbach et al. Citation2015). This literature has often ignored the premise that cause-specific hazard rates are interdependent and that education and mortality both depend on unobserved cognitive ability. In this study we analysed the education–mortality gradient at ages 18–63 among Swedish men, focusing on months lost due to specific causes of death (which solves the interdependence problem) and using a structural model that accounts for confounding due to cognitive ability.
Our results suggest that conventional analysis of education and mortality may be biased, even if accounting for observed cognitive score. First, using our preferred structural model, we find that the educational gains in mortality are much smaller for most major causes of death among those with higher levels of education than would be implied by a standard proportional hazards regression with measured cognitive score. This finding supports the notion of strong positive selection into higher levels of education based on unobserved cognitive ability. Second, we find that among the least educated, our preferred structural model shows larger educational gains in terms of total mortality than a standard proportional hazards regression. This difference is attributable mostly to external causes of death. The fact that accounting for unobserved cognitive ability increases the educational gains in mortality might be explained by positive discrimination in the Swedish educational system towards those with the lowest cognitive abilities (the system tries to lift even those with very low cognitive ability into secondary education). Another reason for this might be that other unobserved factors, such as non-cognitive skills, influence both the education attained and cause-specific mortality.
Our paper makes three distinct contributions to the literature: two methodological and one substantive. First, we define the educational gains for different causes of death in terms of months lost instead of through hazard ratios. Specifying the educational gains in terms of months lost instead of the odds of dying has important advantages. A Cox model ignores the premise that the competing causes of death are often interdependent and, also, the interpretation of the coefficients in a Cox model is difficult, as the probability of dying from one particular cause depends on the hazards of dying from all other causes. The ‘months lost’ due to a specific cause of death takes the interdependence into account, especially in our structural model, and the interpretation is very simple. An additional advantage of the ‘months lost’ measures is that they are additive, over both the causes of death and the levels of education. Second, we use a structural model to estimate the educational gains, accounting for the interdependence of cognitive ability and education, and their joint influence on mortality from each cause. The advantage of using a structural model is that it explicitly accounts for cognitive ability, which affects both educational attainment and cause-specific mortality.
Our third contribution is empirical. Our results reveal that the largest educational gains in months alive are found for men with compulsory education only, via the reduction of external causes of death, such as traffic accidents and suicide. We estimate an educational gain of seven months alive between ages 18 and 63 if they were to go through two years of secondary education in addition. This result is larger than standard (non-structural) proportional hazards regression would imply, even if the standard model controls for observed cognitive score. It appears that the standard approach may suffer from downward bias for the least educated. A hypothesis stemming from this finding, and a potential explanation for this downward bias, might be the positive discrimination in the Swedish educational system. It is beyond the scope of this study to analyse the importance of such (potential) positive discrimination further, but it appears that, if confirmed, this would lend further strong support for policies targeted at improving the educational outcomes of low-achieving boys and men.
We also find that for more highly educated groups the educational gain is the largest from the reduction of external causes, but this gain is only one month between ages 18 and 63. For this age range the educational gains in the reduction of cardiovascular and cancer mortality are also rather small, at less than one month.
Our study has four distinct strengths compared with previous research. First, a clear advantage of the study is the very large sample size, which allows the estimation of the detailed structural model with four education levels and four causes of death, accounting for confounding in the education attained. Second, the data are population based and not prone to self-selection, because military conscription was mandatory in Sweden during the 1950s. Third, our statistical method, using a structural model in which the education attained and cause-specific mortality are modelled simultaneously, accounts for the confounding effect of intelligence on cause-specific mortality. This enables us to draw (close to) causal conclusions from our analysis without suffering the generalization issues inherent in using compulsory schooling reforms to account for confounding. Fourth, contrary to the standard literature on causes of death (competing risks), we define the educational gains of causes of death in terms of months lost due to each specific cause of death instead of using the hazard ratio. This ‘months lost’ quantity is easier to interpret, avoids the issues of independence in competing risks proportional hazards models, and can be defined over a segment of the age distribution. The ‘months lost’ quantity is also an additive measure: the sum over all alternative causes of death within one education level is equal to the total number of months lost (and the educational gain) for that education level, while the sum of educational gains over all education levels within a cause of death is equal to the total educational impact for that cause of death.
Our study also has limitations. First, there is no military examination information or other large data set containing an intelligence test for women that would allow for similar analyses for women. Second, the follow-up time is relatively short, with a maximum age of 63. A fruitful avenue for future research would be to investigate the data again, say, ten years from now, when the cohort has reached age 73 and the distribution of the causes of death may have changed (presumably with more cardiovascular and cancer deaths). Third, although we controlled for some childhood family background, through paternal education and maternal socio-economic status, we may have ignored important family characteristics. Nor could we account for unobserved family characteristics. However, Elo et al. (Citation2014) have found that once observed parental education and socio-economic status are controlled for, the unobserved family factors do not matter for the education–mortality association. Fourth, although military conscription was mandatory in Sweden, men with severe mental disabilities or severe chronic diseases were exempted from the military examination. Thus, our results only apply to those with no severe mental disabilities or chronic diseases at age 18. Finally, a limitation of our data is the absence of direct measurements of non-cognitive ability, such as the Big Five taxonomy of personality traits: conscientiousness, openness, extraversion, agreeableness, and neuroticism. Hence, we cannot rule out the premise that specific non-cognitive factors influence both education and cause-specific mortality; this means that our educational gain cannot be interpreted as the causal effect of education on months lost and may in fact be an upper bound to it. Bijwaard, van Kippersluis, et al. (Citation2015) have shown that when accounting for non-cognitive skills as well, the educational gain in mortality becomes smaller. Finally, the issue of reverse causality—early childhood health affecting educational attainment—might distort our analyses. We do not have sufficient information about childhood health status, which prevents us from investigating the possibility of reverse causality from health to education in our sample.
Supplementary Material
Download PDF (86.5 KB)ORCID
Govert E. Bijwaard http://orcid.org/0000-0002-6458-1647
Notes
1 Govert E. Bijwaard is at the Netherlands Interdisciplinary Demographic Institute. Per Tynelius is at the Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden and the Centre for Epidemiology and Community Medicine, Stockholm County Council, Stockholm, Sweden. Mikko Myrskylä is at the Max Planck Institute for Demographic Research, the London School of Economics and Political Science, and the University of Helsinki. Please direct all correspondence to Govert E. Bijwaard, Netherlands Interdisciplinary Demographic Institute (NIDI-KNAW/University of Groningen), PO Box 11650, 2502 AR The Hague, The Netherlands; or by E-mail: [email protected]
References
- Aalen, O. and S. Johansen. 1978. An empirical transition matrix for nonhomogeneous Markov chains based on censored observations, Scandinavian Journal of Statistics 5:141–150.
- Albouy, V. and L. Lequien. 2009. Does compulsory education lower mortality? Journal of Health Economics 28(1): 155–168. doi: 10.1016/j.jhealeco.2008.09.003
- Amin, V., J. R. Behrman, and H. P. Kohler. 2015. Schooling has smaller or insignificant effects on adult health in the US than suggested by cross-sectional associations: New estimates using relatively large samples of identical twins, Social Science & Medicine 127: 181–189. doi: 10.1016/j.socscimed.2014.07.065
- Andersen, P. K. 2013. Decomposition of number of life years lost according to causes of death, Statistics in Medicine 32(30): 5278–5285. doi: 10.1002/sim.5903
- Andersen, P. K., V. Canudas-Romo, and N. Keiding. 2013. Cause-specific measures of life years lost, Demographic Research 29(41): 1127–1152. doi: 10.4054/DemRes.2013.29.41
- Anderson, T. and H. Rubin. 1956. Statistical inference in factor analysis, in J. Neyman (ed.), Proceedings of the Third Berkeley Symposium Mathematical Statistics and Probability, Volume V. Berkeley: University of California Press, pp. 111–150.
- Arendt, J. N. 2005. Does education cause better health? A panel data analysis using school reforms for identification, Economics of Education Review 24(2): 149–160. doi: 10.1016/j.econedurev.2004.04.008
- Auld, M. C. and N. Sidhu. 2005. Schooling, cognitive ability and health, Health Economics 14(10): 1019–1034. doi: 10.1002/hec.1050
- Backlund, E., P. D. Sorlie, and N. J. Johnson. 1999. A comparison of the relationships of education and income with mortality: The national longitudinal mortality study, Social Science & Medicine 49: 1373–1384. doi: 10.1016/S0277-9536(99)00209-9
- Batty, G. D., I. J. Deary, and L. S. Gottfredson. 2007. Premorbid (early life) IQ and later mortality risk: Systematic review, Annals of Epidemiology 17(4): 278–288. doi: 10.1016/j.annepidem.2006.07.010
- Batty, G. D., C. R. Gale, P. Tynelius, I. J. Deary, and F. Rasmussen. 2009. IQ in early adulthood, socioeconomic position, and unintentional injury mortality by middle age: A cohort study of more than 1 million Swedish men, American Journal of Epidemiology 169(5): 606–615. doi: 10.1093/aje/kwn381
- Batty, G. D., K. M. Wennerstad, G. D. Smith, D. Gunnell, I. J. Deary, P. Tynelius, and F. Rasmussen. 2007. IQ in early adulthood and later cancer risk: Cohort study of one million Swedish men, Annals of Oncology 18(1): 21–28. doi: 10.1093/annonc/mdl473
- Batty, G. D., K. M. Wennerstad, G. D. Smith, D. Gunnell, I. Deary, P. Tynelius, and F. Rasmussen. 2009. IQ in early adulthood and mortality by middle age: Cohort study of 1 million Swedish men, Epidemiology 20(1): 100–109. doi: 10.1097/EDE.0b013e31818ba076
- Behrman, J., H. Kohler, V. Jensen, D. Pedersen, I. Petersen, P. Bingley, and K. Christensen. 2011. Does more schooling reduce hospitalization and delay mortality? New evidence based on Danish twins, Demography 48(4): 1347–1375. doi: 10.1007/s13524-011-0052-1
- Beltrán-Sánchez, H., S. Preston, and V. Canudas-Romo. 2008. An integrated approach to cause-of-death analysis: Cause-deleted life tables and decompositions of life expectancy, Demographic Research 19(35): 1323–1350. doi: 10.4054/DemRes.2008.19.35
- Bijwaard, G. E., M. Myrskylä, P. Tynelius, and F. Rasmussen. 2017. Educational gains in cause-specific mortality: Accounting for cognitive ability and family-level confounders using propensity score weighting, Social Science & Medicine, 184: 49–56 doi: 10.1016/j.socscimed.2017.05.019
- Bijwaard, G. E., H. van Kippersluis, and J. Veenman. 2015. Education and health: The role of cognitive ability, Journal of Health Economics 42: 29–43. doi: 10.1016/j.jhealeco.2015.03.003
- Bijwaard, G. E., F. van Poppel, P. Ekamper, and L. H. Lumey. 2015. Gains in life expectancy associated with higher education in Men , PloS ONE 10(10), e0141200. doi: 10.1371/journal.pone.0141200
- Borrell, C., A. Plasència, M. Huisman, G. Costa, A. Kunst, O. Andersen, M. Bopp, J.-K. Borgan, P. Deboosere, M. Glickman, S. Gadeyne, C. Minder, E. Regidor, T. Spadea, T. Valkonen, and J. P. Mackenbach. 2005. Education level inequalities and transportation injury mortality in the middle aged and elderly in european settings , Injury Prevention 11(3): 138–142. doi: 10.1136/ip.2004.006346
- Calvin, C. M., I. J. Deary, C. Fenton, B. A. Roberts, G. Der, N. Leckenby, and G. D. Batty. 2011. Intelligence in youth and all-cause-mortality: Systematic review with meta-analysis, International Journal of Epidemiology 40(3): 626–644. doi: 10.1093/ije/dyq190
- Clark, D. and H. Royer. 2013. The effect of education on adult mortality and health: Evidence from Britain, American Economic Review 103(6): 2087–2120. doi: 10.1257/aer.103.6.2087
- Conti, G. and J. J. Heckman. 2010. Understanding the early origins of the education-health gradient: A framework that can also be applied to analyze gene-environment interactions, Perspectives on Psychological Science 5(5): 585–605. doi: 10.1177/1745691610383502
- Conti, G., J. J. Heckman, and S. Urzua. 2010. The education-health gradient, American Economic Review 100(2): 234–238. doi: 10.1257/aer.100.2.234
- Cutler, D. and A. Lleras-Muney. 2008. Education and health: Evaluating theories and evidence, in J. S. House, R. F. Schoeni, G. A. Kaplan, and H. Pollack (eds.), Making Americans Healthier: Social and Economic Policy as Health Policy. New-York: Russell Sage Foundation.
- Deary, I. J. 2008. Why do intelligent people live longer? Nature 456(7219): 175–176. doi: 10.1038/456175a
- Deary, I. J. and W. Johnson. 2010. Intelligence and education: Causal perceptions drive analytic processes and therefore conclusions, International Journal of Epidemiology 39(5): 1362–1369. doi: 10.1093/ije/dyq072
- Elo, I. T. and S. H. Preston. 1996. Educational differentials in mortality: United States, 1979–1985. Social Science & Medicine 42: 47–57. doi: 10.1016/0277-9536(95)00062-3
- Elo, I. T., P. Martikainen, and M. Myrskylä. 2014. Socioeconomic status across the life course and all-cause and cause-specific mortality in Finland, Social Science & Medicine 119: 198–206. doi: 10.1016/j.socscimed.2013.11.037
- Fletcher, J. M. 2015. New evidence of the effects of education on health in the US: Compulsory schooling laws revisited, Social Science & Medicine 127: 101–107. doi: 10.1016/j.socscimed.2014.09.052
- Galobardes, B., J. W. Lynch, and G. D. Smith. 2004. Childhood socioeconomic circumstances and cause-specific mortality in adulthood: Systematic review and interpretation, Epidemiologic Reviews 26(1): 7–21. doi: 10.1093/epirev/mxh008
- Gavrilov, L. A. and N. S. Gavrilova. 1991. The Biology of Life Span: A Quantitative Approach. New York: Harwood Academic Publisher.
- Gottfredson, L. 2004. Intelligence: is the epidemiologists’ elusive ‘fundamental cause’ of social class inequalities in health? Journal of Personality and Social Psychology 86(1): 174–199. doi: 10.1037/0022-3514.86.1.174
- Gottfredson, L. S. and I. J. Deary. 2004. Intelligence predicts health and longevity, but why? Current Directions in Psychological Science 13(1): 1–4. doi: 10.1111/j.0963-7214.2004.01301001.x
- Halpern-Manners, A., L. Schnabel, E. M. Hernandez, J. L. Silberg, and L. J. Eaves. 2016. The relationship between education and mental health: New evidence from a discordant twin study, Social Forces, 95(1):107–131. doi: 10.1093/sf/sow035
- Huisman, M., A. E. Kunst, M. Bopp, J.-K. Borgan, C. Borrell, G. Costa, P. Deboosere, S. Gadeyne, M. Glickman, C. Marinacci, C. Minder, T. Valkonen, and J. P. Mackenbach. 2005. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations, The Lancet 365(9458): 493–500. doi: 10.1016/S0140-6736(05)17867-2
- Hummer, R. A. and J. T. Lariscy. 2011. Educational attainment and adult mortality, in R. G. Rogers and E. M. Grimmins (eds.), International Handbook of Adult Mortality, Volume 2. Dordrecht, the Netherlands: Springer, pp. 241–260.
- Hummer, R. A., R. G. Rogers, and I. W. Eberstein. 1998. Sociodemographic differentials in adult mortality: A review of analytic approaches, Population and Development Review 24(3): 553–578. doi: 10.2307/2808154
- Imbens, G. W. 2004. Nonparametric estimation of average treatment effects under exogeneity: A review, Review of Economics and Statistics 86(1): 4–29. doi: 10.1162/003465304323023651
- Kaestner, R. and K. Callison. 2011. Adolescent cognitive and noncognitive correlates of adult health, Journal of Human Capital 5(1): 29–69. doi: 10.1086/660082
- Kulhánová, I., R. Hoffmann, T. A. Eikemo, G. Menvielle, and J. P. J. P. Mackenbach. 2014. Educational inequalities in mortality by cause of death: First national data for the Netherlands, International Journal of Public Health 59(5): 687–696. doi: 10.1007/s00038-014-0576-4
- Lleras-Muney, A. 2005. The relationship between education and adult mortality in the United States. Review of Economic Studies 72(1): 189–221. doi: 10.1111/0034-6527.00329
- Lorant, V., A. E. Kunst, M. Huisman, G. Costa, and J. P. Mackenbach. 2005. Socio-economic inequalities in suicide: A European comparative study, British Journal of Psychiatry 187(1): 49–54. doi: 10.1192/bjp.187.1.49
- Lundborg, P. 2013. The health returns to schooling: What can we learn from twins? Journal of Population Economics 26(2): 673–701. doi: 10.1007/s00148-012-0429-5
- Lynch, S. M. 2003. Cohort and life-course patterns in the relationship between education and health: A hierarchical approach. Demography 40(2): 309–331. doi: 10.1353/dem.2003.0016
- Mackenbach, J. P., I. Kulhánová, M. Bopp, P. Deboosere, T. A. Eikemo, R. Hoffmann, M. C. Kulik, M. Leinsalu, P. Martikainen, G. Menvielle, E. Regidor, B. Wojtyniak, O. Östergren, and O. Lundberg. 2015. Variations in the relation between education and cause-specific mortality in 19 European populations: A test of the ‘fundamental causes’ theory of social inequalities in health, Social Science & Medicine 127: 51–62. doi: 10.1016/j.socscimed.2014.05.021
- Mazumder, B. 2008. Does education improve health: A reexamination of the evidence from compulsory schooling laws, Economic Perspectives 33: 2–16.
- McCartney, G., C. Collins, and M. Mackenzie. 2013. What (or who) causes health inequalities: Theories, evidence and implications? Health Policy 113(3): 221–227. doi: 10.1016/j.healthpol.2013.05.021
- Meghir, C., M. Palme, and E. Simeonova. 2018. Education and mortality: Evidence from a social experiment. American Economic Journal: Applied Economics 10(2): 234–256.
- Mirowsky, J. and C. E. Ross. 2003. Education, Social Status, and Health. New York: Aldine de Gruyter.
- Montez, J. K., R. Hummer, and M. D. Hayward. 2012. Educational attainment and adult mortality in the United States: A systematic analysis of functional form, Demography 49: 315–336. doi: 10.1007/s13524-011-0082-8
- Næss, Ø., D. A. Hoff, D. Lawlor, and L. H. Mortensen. 2012. Education and adult cause-specific mortality—examining the impact of family factors shared by 871 367 Norwegian siblings, International Journal of Epidemiology 41(6): 1683–1691. doi: 10.1093/ije/dys143
- Preston, S. H. and P. Taubman. 2011. Socioeconomic differences in adult mortality and health status, in L. G. Martin and S. H. Preston (eds.), Demography of Aging. Washington, DC: National Academy Press, pp. 279–318.
- Roy, A. 1951. Some thoughts on the distribution of earnings, Oxford Economic Papers 3: 135– 146. doi: 10.1093/oxfordjournals.oep.a041827
- Smith, J. P. 2004. Unraveling the SES-health connection, Population and Development Review 30: 108–132. doi: 10.1111/j.1728-4457.2004.011_1.x
- Thomas, J. M. 1996. On the interpretation of covariate estimates in independent competing-risks models, Bulletin of Economic Research 48(1): 27–39. doi: 10.1111/j.1467-8586.1996.tb00622.x
- Van Kippersluis, H., O. O’Donnell, and E. van Doorslaer. 2011. Long-run returns to education: Does schooling lead to an extended Old Age? Journal of Human Resources 46(4): 695–721. doi: 10.1353/jhr.2011.0006