
Abstract
Previous research has documented intergenerational transmission of human capital from children to parents. Less is known, however, about heterogeneity in this ‘upward transmission’ in low-resource settings. We examine whether co-resident adult children’s education is associated with improved health among older parents in India, using nationally representative data from the 2014 Indian National Sample Survey. Parents of children with tertiary education had a lower probability of reporting poor health than parents of children with less than primary education. The benefits of children’s education persisted after controlling for economic factors, suggesting that non-pecuniary pathways—such as health knowledge or skills—may play an important role. The association was more pronounced among economically dependent parents and those living in the North and West regions. Taken together, our results point to a strong positive association between children’s education and parental health, the role of non-pecuniary pathways, and the importance of subnational heterogeneity in India.
Introduction
India’s population is expected to grow from 1.34 billion to 1.64 billion by 2050, making India soon the most populous nation in the world (United Nations Department of Economic and Social Affairs, Population Division Citation2019). India is also ageing substantially: the proportion of the population aged 60 years and older was 9.4 per cent in 2017 and is expected to double by 2050 (United Nations Department of Economic and Social Affairs, Population Division Citation2017). India’s older population is particularly economically and socially vulnerable due to high rates of illiteracy and economic dependency (Bloom et al. Citation2010). In this context, investments in children’s education may be advantageous not only for the health of those individuals themselves (Grossman Citation1975; Link and Phelan Citation1995; Lleras-Muney Citation2005; Baker et al. Citation2011; Berkman et al. Citation2014; De Neve et al. Citation2015) and for their own children (Gakidou et al. Citation2010; Karlsson et al. Citation2019; Mensch et al. Citation2019), but also for the older generations (Zimmer et al. Citation2007; Torssander Citation2013).
Evidence on the health benefits of children’s education for older generations dates back to at least the early 2000s (Zimmer et al. Citation2002). Since then, a consistent positive association has been identified between children’s education and a wide range of parental health outcomes, including: (1) parental mortality (Torssander Citation2013; Friedman and Mare Citation2014; Elo et al. Citation2018; Smith-Greenaway et al. Citation2018; Wolfe et al. Citation2018; Sabater et al. Citation2019); (2) parental physical health (Yahirun et al. Citation2016, Citation2017; Meyer et al. Citation2019); and (3) parental mental health (Sabater and Graham Citation2016; Lee Citation2018; Peng et al. Citation2019; Yahirun et al. Citation2020). These associations persist after controlling for parents’ demographic and socio-economic characteristics (De Neve and Kawachi Citation2017). More recently, a handful of quasi-experimental studies have identified causal effects of children’s education on parental health. In high-income settings, such as Sweden, additional children’s education has generally led to modest and heterogeneous protective effects on parental mortality (Lundborg and Majlesi Citation2018; Potente et al. Citation2018). In contrast, in low-resource settings, substantial benefits of children’s education have been identified. In Tanzania, for instance, each additional year of children’s education reduced the probabilities of maternal and paternal death by 3.7 and 0.4 percentage points, respectively (De Neve and Fink Citation2018).
Hypothetical mechanisms
There are a number of mechanisms that may explain the effect of children’s education on parental health. Research has suggested that adult children may ‘repay’ their parents for investments received in childhood, especially in settings where governmental support for older individuals is limited (Frankenberg et al. Citation2002). Given the strong relationship between education and income (Psacharopoulos and Patrinos Citation2018), children with additional education may share their increased financial resources with their parents (Ladusingh and Narayana Citation2011), positively affecting the parents’ health outcomes. Children with more education may also share their health knowledge (He et al. Citation2015), skills (Kuziemko Citation2014), and behaviours (Berniell et al. Citation2013) with older family members. For example, children with more education may be better equipped to interact with the health system and manage the health needs of their parents, especially those with complex old-age care plans. Educated children may also be more aware of ‘emerging epidemics’, such as type 2 diabetes, which are increasingly common among older adults in rapidly developing middle-income economies (Geldsetzer et al. Citation2018). Additional education may also open up access to careers in the health sector, allowing the provision of direct care to family members (Chen et al. Citation2019).
Effect heterogeneity
The strength and pathways of the relationship between children’s education and parental health are also likely to vary by demographic and socio-economic characteristics. The relationship may be more pronounced for parents with a lower socio-economic status (SES) by acting as a ‘substitute’ for a lack of resources (Ross and Mirowsky Citation2010). The relationship may also vary by age of the parent. On the one hand, the benefits of children’s education for parental health may be attenuated later in life if selective mortality at older ages leads to a convergence in health among older adults—the idea that age is a ‘leveller’ (House et al. Citation2005). On the other hand, the advantages of children’s education for parental old-age health may ‘cumulate’ over a parent’s life course, leading to larger differences in health by children’s education as parents age (Ross and Wu Citation1996; Dannefer Citation2003). While a considerable amount of evidence suggests that age may be a leveller in high-income settings (Friedman and Mare Citation2014; Zimmer et al. Citation2016; Elo et al. Citation2018; Wolfe et al. Citation2018; Sabater et al. Citation2019; Yahirun et al. Citation2020), relatively little is known about the age gradient in low-resource settings. Similarly, the benefits of children’s education may also vary by geographical region. Older adults living in wealthier regions, for instance, may be able to take better advantage of opportunities arising from increased children’s education if employment opportunities or social services are more easily accessible. This may be particularly the case in large countries, where there is substantial variation in economic conditions across subnational administrative units (Jung et al. Citation2019).
Current study
This study adds to a growing body of research on the association between children’s education and parental old-age health. We study this question in a particular context—India—where co-residence between adult children and their older parents is among the highest in the world (Esteve and Liu Citation2017). In our analytical sample, described in detail later, only 20.8 per cent of older parents did not co-reside with offspring. This estimate is consistent with recent studies on the living arrangements of older adults in India (Samanta et al. Citation2015). Furthermore, with the institution of the Maintenance and Welfare of Parents and Senior Citizens Act, 2007, adult children are legally required to support their older parents if parents are unable to maintain themselves (Serrano et al. Citation2017). To our knowledge, however, no study has examined the relationship between children’s education and the old-age health of both mothers and fathers in India. In this study, we therefore aim to make three contributions to the literature on ‘upward transmission’ of human capital from children to parents. First, we examine the relationship between co-resident adult children’s education and parental health using nationally representative data from India. Second, we explore the role of key economic factors, such as household expenditure, as potential mechanisms. Third, we consider the importance of heterogeneity by parental demographic and socio-economic characteristics, including parental sex, age, and SES, as well as geographical region in India. In doing so, this study aims to point research and policy efforts towards more targeted interventions to improve the health outcomes of the rapidly growing older population in the region.
Methods
Data source and study population
Data were extracted from the 71st round of the Indian National Sample Survey (NSS), a cross-sectional, nationally representative survey conducted from January to June 2014. The survey collected comprehensive information on the health and socio-economic characteristics of the sample respondents. Although several large longitudinal data collection efforts are under way in India (Arokiasamy et al. Citation2012; Kowal et al. Citation2012), the NSS data provide the most recent nationally representative data on the health of older Indians. The survey used a stratified multistage design, with the sample stratified by district and then by urban or rural areas. First-stage sampling units were the census villages in the rural sector and Urban Frame Survey blocks in the urban sector. Second-stage sampling units were households in both urban and rural sectors. The survey also included households residing in an open space or a roadside shelter and persons staying in retirement homes. In total, the survey covered 65,932 households, yielding information on 333,104 individuals. Additional information on the survey and sampling is provided in detail elsewhere (Indian Council of Social Science Research Citation2014).
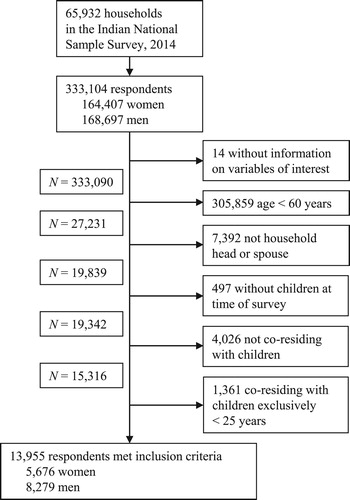
We limited our analyses to respondents aged at least 60 years (N = 27,231) who were a household head or their spouse (N = 19,839), had at least one living child at the time of the survey (N = 19,342), and co-resided with at least one child (N = 15,316). The NSS did not collect data on the educational level of children who were not co-resident with their parents. However, older adults in India generally live in multigenerational households, with 79.2 per cent of older adults in our sample living with at least one child. To our knowledge, there are currently no nationally representative data available for India that include the educational attainment of adult children living outside the household. We also limited the sample to parents who were co-residing with at least one child aged 25 years or older. Limiting the sample to parents with adult children meant that children would have had the opportunity to complete formal education. In sensitivity analyses, however, we examined alternative sample criteria including children aged at least either 15 or 20 years (instead of at least 25 years old). Our final analytical sample comprised 13,955 older parents. shows a study participant flow diagram.
Figure 1 Study participant flow diagram
Outcome variables
Our primary outcome variable was self-reported health (SRH). While respondents were asked whether they perceived their current state of health to be in one of five categories (poor, fair, good, very good, or excellent), field staff were instructed to enter (code) current state of health in three categories during data collection. The three final categories available in the original data set were therefore: (1) ‘poor’; (2) ‘fair/good’; or (3) ‘very good/excellent’ health (Indian Council of Social Science Research Citation2014). SRH has been shown to be a powerful indicator for both objective and subjective health, including among older adults in the Indian context (Subramanian et al. Citation2009; Hirve Citation2014). We also considered two secondary outcomes to capture different dimensions of health: parents’ change in SRH compared with the previous year as an additional subjective indicator but with a longer time span, and physical mobility as a more objective outcome (Leinonen et al. Citation1998; Jylhä Citation2009; Hirve Citation2014). Change in SRH was defined as either ‘worse’, the ‘same’, or ‘better’ compared with the previous year, whereas physical mobility was defined as either ‘confined to bed’, ‘confined to home’, or ‘physically mobile’ (Indian Council of Social Science Research Citation2014).
Children’s education
Our main independent variable of interest was adult children’s educational attainment. We defined children’s educational attainment as the maximum level of school achieved by any of the co-resident children. We categorized this into five levels: zero education or less than primary school completed (level 1), primary school (level 2), secondary school (level 3), high school (level 4), and college or university (level 5). We chose school levels completed as opposed to years of schooling because: (1) the NSS contains data on school level completed but not years of schooling; (2) school level may be less prone to measurement error (a degree is a relatively more tangible measure of educational achievement across varying contexts in India); and (3) possible financial pathways between children’s education and parental health are likely to be dependent on school level completed (i.e. their ‘credentials’ in the labour market) (Jaeger and Page Citation1996). In our main analysis, we chose the maximum level of schooling completed among adult children to further facilitate the interpretation of our results. In sensitivity analyses, however, we also used the mean and minimum educational levels completed by co-resident children, as well as the proportion of children with a certain level of education (Peng et al. Citation2019).
Covariates
Building on prior evidence and a conceptual framework for the role of children’s education in parental old-age health in low-resource settings (De Neve and Harling Citation2017), we included a set of parental characteristics: age group (60–64, 65–69, 70–74, 75+ years), sex, marital status, education, and social group (backward class, scheduled caste, scheduled tribe, other). Parental education, for instance, is linked both to improved health among individuals themselves and to educational attainment among children, including in the context of India (Azam and Bhatt Citation2015). Parental educational levels were constructed in the same way as children’s, to facilitate comparisons across generations.
We also examined variables that potentially mediate the link between children’s education and parental old-age health, including household-level per capita expenditure and primary household occupation group (casual labour, regular salary, self-employed, other), as well as parental economic dependence (not dependent on others, partially dependent on others, or fully dependent on others). As our measure of household expenditure, we used monthly per capita expenditure, which was constructed by dividing the total monthly expenditure by the number of household members. Household expenditure was then categorized into quintiles, with the first quintile being the lowest-spending quintile. Primary household occupation group was defined as ‘the occupation which fetched the maximum earnings to the household during the last 365 days preceding the date of survey’. Additional details on survey questions and the construction of covariates are described elsewhere (Indian Council of Social Science Research Citation2014).
Statistical analyses
We examined the relationship between children’s education and parental old-age health using an ordered logistic regression model (Guzman-Castillo et al. Citation2015). We considered two different models. First, we estimated a model controlling for potential confounders to see if the relationship between children’s education and parental health is robust to socio-demographic characteristics which likely precede children’s education, including parental age, parental sex, parental marital status, parental social group, and parental education (Model 1). Second, we aimed to assess whether economic factors may explain (e.g. as possible mediators) the relationship between children’s education and parental old-age health (Model 2). To do so, we additionally included household expenditure, primary household occupation group, and parental economic dependence along with the covariates of Model 1. We also tested for heterogeneity in associations by demographic and socio-economic characteristics, including parental age, sex, SES, and geographical region, by interacting all independent variables with each characteristic in separate models (parametrically identical to stratifying models). In addition to these pooled analyses, we show results obtained from stratifying our analyses by parental and children’s sex (Lee et al. Citation1994), parental age, parental education, parental economic dependence, geographical region, and type of parent–child relationship (biological children vs. sons/daughters-in-law) (De Neve and Kawachi Citation2017). We used sample weights for all descriptive statistics. We clustered standard errors at the primary sampling unit level to take into account spatial correlation between respondents.
In addition to the sensitivity analyses already described, we conducted a wide range of supplementary analyses to generate additional confidence in the robustness of our findings. First, we tested whether the proportional odds assumption was met. To do so, we conducted a Brant test (Brant Citation1990), which suggested that the parallel regression assumption was violated for three variables in our extended model (parental sex, marital status, and household expenditure). We therefore additionally estimated a partial proportional odds model (generalized ordered logistic regression) in which some variables were constrained to meet the proportional odds assumption while others were not (Williams Citation2006). Second, we examined alternative specifications of age. We included age and age squared to capture non-linearities in the relationship between parental health and old age. Third, we extended our sample inclusion criteria of biological children to sons/daughters-in-law, since prior literature has suggested a similar role in determining parental old-age health (Pinquart and Sorensen Citation2011). Fourth, we included a number of potential confounders and mediators (in addition to those included in Model 2) that were available in the NSS data, such as area, family structure, religion, and geographical region, to determine whether our main results would hold up to additional controls. We were also interested in knowing whether the association persisted when controlling for specific parental health conditions (such as chronic conditions) as well as healthcare usage. Fifth, we tested the association using NSS-provided sampling weights. Sixth, as a benchmark for our multivariable models, we estimated the bivariate (unadjusted) relationship between children’s education and parental health. This was a complete case analysis and all analyses were conducted in StataMP 15.1.
Results
Descriptive statistics
shows descriptive statistics, separately by parental sex and for the pooled sample. The mean age for all parents was 66.8 years (standard deviation (SD) 6.4; not shown in table). Across 13,955 older adults, 3,150 (18.9 per cent) rated their current state of health as poor, 9,752 (72.9 per cent) as good/fair, and 1,053 (8.2 per cent) as very good/excellent. Women rated their health worse than men on average. No substantial difference by sex was found across our secondary health outcomes (change in SRH compared with the previous year and physical mobility). In terms of socio-economic factors, we identified large differences by parental sex: for instance, 3,927 out of 5,676 women (70.4 per cent) and 2,803 out of 8,279 men (36.0 per cent) reported full economic dependence. Among economically dependent parents, nearly all men reported being financially supported by their children (96.4 per cent), whereas this was the case for about three in four women (76.5 per cent). In terms of parental educational attainment, 3,963 women (77.3 per cent) and 3,772 men (53.9 per cent) did not complete primary school, whereas more than three times as many men vs. women completed secondary school or higher. In contrast, children’s educational attainment was substantially higher than that of their parents, and gender gaps in children's education were generally small. Across the 13,955 participants, 3,787 parents (29.2 per cent) had children who had completed primary school, 4,615 (34.5 per cent) had children with completed secondary or high school, and 4,059 (23.0 per cent) had children with completed tertiary education. In terms of household characteristics, most households included four or five household members (42.5 per cent; not shown in table).
Table 1 Selected characteristics of study participants (older parents in India, 2014)
We also compared descriptive statistics of our analytical sample with those of the population-representative sample, defined as all individuals aged 60 years or older (regardless of whether they had children or lived with their adult children). Health outcomes and socio-demographic characteristics, including self-reported general health and educational attainment, were nearly identical across both samples, with the exception of parental economic dependence. In our analytical sample, more older adults reported being fully economically dependent on others (about 5 percentage points higher than in the population-representative sample), suggesting that they are somewhat more economically vulnerable. Descriptive statistics of the population-representative sample are available in the survey report (National Sample Survey Office Citation2014).
Children’s education and parental health
In , we show our main results displayed as proportional odds ratios (ORs). Under the proportional odds assumption, the OR is interpreted as constant across each ‘split’ of the categories of the ordinal outcome. Children’s educational level was positively associated with parental old-age health across all models. In regression models controlling only for socio-demographic variables (Model 1), compared with parents whose children had completed less than primary school, odds of reporting very good/excellent health (vs. the combined categories of poor and fair/good health) were higher for parents with children who had completed primary school (OR 1.09; 95 per cent confidence interval (CI) 0.95–1.25); secondary school (OR 1.32; 95 per cent CI 1.13–1.54); high school (OR 1.29; 95 per cent CI 1.09–1.52); or tertiary education (OR 1.41; 95 per cent CI 1.20–1.64). Parents whose children were better educated were also more likely to report positive changes in health during the year preceding the survey and higher levels of physical mobility. Compared with parents whose children had completed less than primary school, parents had 28 per cent higher odds of reporting improved health (vs. worse and similar health) if their children had completed tertiary education (OR 1.28; 95 per cent CI 1.11–1.48), and 33 per cent higher odds of reporting physical mobility (vs. being confined to bed or home) if their children had completed tertiary education (OR 1.33; 95 per cent CI 1.01–1.75). When additionally taking into account possible mediators such as household expenditure, the coefficients on children’s education were attenuated only slightly and remained strongly significant (Model 2). Parents whose children had completed tertiary education still had 39 per cent higher odds (OR 1.39; 95 per cent CI 1.18–1.63) of reporting very good/excellent health vis-à-vis parents whose children had completed less than primary education. Our results were robust to a wide range of sensitivity analyses, including when using alternative specifications of our model, covariates, and sample (Tables S1–S4 in the supplementary material). Our results also persisted when additionally controlling for healthcare usage by parents (Table S3, Model 10).
Table 2 Ordered logistic regression results for the association between children’s education and three measures of parental health, India, 2014
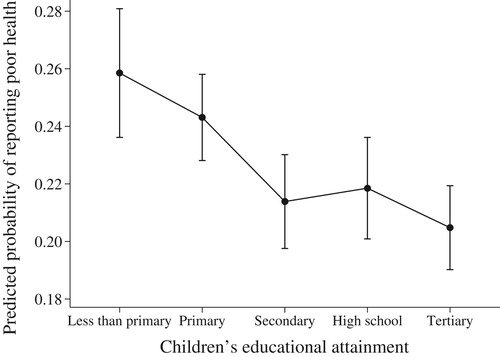
In , we plot the predicted probability among older parents of reporting poor health, by different levels of their children’s educational attainment. All covariates other than children’s education were held at their observed values. The absolute probability of reporting poor health among parents whose children had completed tertiary education was 5.4 percentage points lower (95 per cent CI 2.6–8.1), relative to a baseline of 25.9 per cent among parents whose children had completed less than primary education. To put these magnitudes into perspective, parents’ own tertiary education was associated with a reduction of 5.9 percentage points (95 per cent CI 3.1–8.7) in reporting poor health compared with less than primary education.
Figure 2 Predicted probability of parents reporting poor health, by children’s educational level, India 2014.
Notes: Chart shows results from an ordered regression model which controls for parental age, sex, education, marital status, and social group, as well as household expenditure, occupational group, and economic dependency status (Model 2). All covariates (other than children’s education) were held at their observed values. Self-reported health was defined as either poor (1), fair/good (2), or very good/excellent (3). Vertical bars depict 95 per cent confidence intervals and were calculated using Stata’s margins command. N = 13,955.
Source: Authors’ analysis of data from India National Sample Survey, 2014.
Heterogeneity
In the pooled analyses, the positive association of children’s education with parental self-reported general health did not differ by demographic and socio-economic characteristics, with the exception of parental economic dependence and geographical region in India (p < 0.10 for some interactions; see Table S5, supplementary material). When stratifying our results by parental economic dependence, we found the strongest association among parents who reported being partially economically dependent (Table S6, supplementary material). In , we show results from stratifying our analyses by geographical region in India. We found a stronger association among parents living in the North and West regions. Tables S7–S11 in the supplementary material show results from stratifying our analyses by five other factors, including parental sex, parental age group, parental education, children's sex, and type of relationship (biological children vs. sons/daughters-in-law). Overall, we found a similar association for fathers compared with mothers; whereas the association was somewhat more pronounced for the parental age group 65–69 years, parents with completed primary education or less, households with daughters rather than sons, and biological children compared with sons/daughters-in-law.
Table 3 Ordered logistic regression results for the association between children’s education and current self-reported parental health in India, 2014, by geographical region
Discussion
Using population-based, nationally representative data on nearly 14,000 older adults, we found a strong positive association between co-resident children’s education and parental self-reported health in India. The strong positive relationship between children's education and parental health persisted when controlling for economic factors. One reason could be that the effects of household expenditure and economic dependency status were already captured when entering parental educational attainment into our models (, Model 1). Nonetheless, the residual association between children's education and parental SRH remains large. Older adults in our sample were vulnerable to poor health, with low rates of schooling and high economic dependency. There was also a large gap in educational attainment across generations, and the level of co-residence between adult children and older parents was among the highest in the world (Esteve and Liu Citation2017). In this context, India’s older population may be particularly receptive to the positive health benefits of increased children’s resources (Saikia et al. Citation2019).
Our results are consistent with the limited role of financial mechanisms found in Mexico (Yahirun et al. Citation2016, Citation2017), but are somewhat at odds with findings from China (Jiang Citation2019; Ma Citation2019) and South Korea (Lee Citation2018). In China, additional children’s education increased the size of intergenerational wealth transfers from children to parents, whereas in South Korea wealth transfers partially mediated the relationship between sons’ education and the onset of dementia. Better educated children may also help their parents navigate the health system and gain access to treatment for common chronic conditions. Our results persisted, however, when controlling for chronic conditions and healthcare usage by older parents, suggesting that other mechanisms may play a key role. Alternative mechanisms may include knowledge transfers or skills that shape health behaviours (Berniell et al. Citation2013; Kuziemko Citation2014; Chen et al. Citation2019), the provision of help with household tasks (Jiang and Kaushal Citation2020), or increased emotional closeness.
Our study also provides insights into the heterogeneous nature of the association between children’s education and parental health. Our analyses stratified by socio-economic factors lend support to the notion of ‘resource substitution’ (Ross and Mirowsky Citation2010). Deprived population subgroups may reap the largest health benefits from increased children’s resources. Interestingly, however, when stratifying our analyses by geographical region in India, we found a stronger relationship in the North and West regions, which are relatively wealthy compared with other regions (e.g. East region). One reason could be that older parents who are deprived but live in more prosperous areas may be able to take better advantage of opportunities arising from increased children’s resources. The relationship between children’s education and parental health also peaked for the age group 65–69, but was attenuated for the older parental cohorts. The association later in life may be weakened by, for instance, selective survival of the healthiest parents (Friedman and Mare Citation2014). These findings add to the notion of increasing age ‘levelling out’ intergenerational transfers (Friedman and Mare Citation2014; Zimmer et al. Citation2016; Elo et al. Citation2018; Yahirun et al. Citation2020) and gender disparities in health (Ross and Bird Citation1994).
This study has a number of policy implications. The returns to investments in education programmes may be underestimated if they do not take into account the larger societal benefits of children’s education. Targeting children, in addition to older adults themselves, in public health programmes may be a promising strategy for reaching older family members, particularly in settings where children influence a substantial number of their parents’ health decisions. In China, for instance, an education programme delivered to schoolchildren as part of the formal school curriculum reduced cardiovascular risk factors among their older family members (He et al. Citation2015). In Malawi, a school-based intervention which aims to reduce cardiovascular risk factors in children and their family members is currently under way (UK Research and Innovation Citation2020). Non-communicable diseases, in particular, are expected to pose an increasing challenge for the ageing population in India (Geldsetzer et al. Citation2018), where the health system has largely focused on tackling infectious diseases and maternal and child mortality (Arokiasamy Citation2018). If our results are confirmed in future studies, policies targeting old-age care in India should consider the potential of children’s education to improve the health of the older generation. The positive association between children’s education and parental health also differed considerably between socio-economic groups and contexts, further highlighting the need for tailored interventions.
Limitations
First, although we controlled for a wide range of covariates, our results will represent the causal effect of children’s education only if all relevant confounders are measured and controlled for. Factors such as genetic traits and reverse causality may confound the relationship between children’s education and parental health. Second, our measures were based on self-reported information and hence are susceptible to recall or reporting bias. SRH, however, has been suggested to be a valid and reliable indicator when assessing the health of older adults in India (Subramanian et al. Citation2009). Third, as with most surveys, the NSS only provided information on children for parents who co-reside with their children. The parent–child relationship and causal pathways between children’s education and parental health may differ for children and parents who are not living under the same roof. While co-residence may facilitate the quantity of exchanges between adult children and their parents, living in the same household may add strain to the quality of the parent–child relationship (Umberson Citation1992). Selection bias might also occur if the decision of children to co-reside with older parents depends on children’s education, parental health outcomes, or both (Elwert and Winship Citation2014). The extent of selection bias resulting from co-residence in the study sample, however, is likely to be relatively small because of the high rates of co-residence observed in many Indian surveys (Berkman et al. Citation2012; United Nations Population Fund Citation2013; Samanta et al. Citation2015; Emran et al. Citation2018). Fourth, in Indian households, daughters typically move in with the in-laws after marriage, and sons continue to reside with parents (Chaudhuri and Roy Citation2009). However, our results were consistent when extending our sample to sons/daughters-in-law. Fifth, measures of a number of other relevant aspects of the parent–child relationship (e.g. financial transfers from adult children to their older parents, emotional closeness) were not available. Future research is needed to confirm if—and how—children’s resources shape parental old-age health in low-resource settings.
Conclusions
Children’s education was strongly associated with parental self-reported health, in particular among socio-economically disadvantaged parents and those living in the North and West regions in India. Our findings strengthen the evidence base for large societal benefits of formal education and shed light on considerable variation by demographic and socio-economic factors. Older adults are likely to depend on their children’s resources in settings where health and welfare systems are immature, and where the younger generation enjoys substantially better socio-economic opportunities. Policies that remove barriers to education may further narrow socio-economic disparities in health among older adults in low-resource settings.
Supplementary Material
Download PDF (695.1 KB)Notes
1 Berenike Thoma, Nikkil Sudharsanan, and Jan-Walter De Neve are based at the Heidelberg Institute of Global Health, Medical Faculty and University Hospital, Heidelberg University, Germany. Omar Karlsson is based in the Department of Economic History and the Centre for Economic Demography, both at Lund University, Sweden; and also in the Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Harvard University, USA. William Joe is based at the Population Research Centre, Institute of Economic Growth, University of Delhi Enclave, India. S.V. Subramanian is based in the Department of Social and Behavioral Sciences, Harvard T.H. Chan School of Public Health, Harvard University, USA; and also at the Harvard Center for Population and Development Studies, USA.
2 Please direct all correspondence to Jan-Walter De Neve, Heidelberg Institute of Global Health, Medical Faculty and University Hospital, Heidelberg University, Im Neuenheimer Feld 130.3, R.314, 69120 Heidelberg, Germany; or by E-mail: [email protected]
3 Funding: This work was supported by the Alexander von Humboldt Foundation, funded by Germany’s Federal Ministry of Education and Research, and the Else Kröner-Fresenius-Stiftung within the Heidelberg Graduate School of Global Health. Jan-Walter De Neve was also supported by the European Commission (825823); German Research Foundation (405898232); NICHD of NIH (R03-HD098982); and the Heidelberg University Excellence Initiative. William Joe is supported by a grant from the Tata Trusts to the Institute of Economic Growth, Delhi. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
4 Data availability and ethics: The study was approved by the Heidelberg University Hospital Ethics Committee (S-695/2018) and is based on analyses of anonymized secondary data in the public domain which can be obtained from the Indian National Sample Survey Office.
References
- Arokiasamy, P. 2018. India's escalating burden of non-communicable diseases, The Lancet Global Health 6(12): e1262–e1263. doi: 10.1016/S2214-109X(18)30448-0
- Arokiasamy, P., D. E. Bloom, J. Lee, K. Feeney, and M. Ozolins. 2012. Longitudinal Aging Study in India: Vision, design, implementation, and some early results, in Aging in Asia: Findings from New and Emerging Data Initiatives. J. P. Smith, and M. Majmundar (eds), Panel on Policy Research and Data Needs to Meet the Challenge of Aging in Asia. Committee on Population, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press, pp. 36–74.
- Azam, M., and V. Bhatt. 2015. Like Father, Like Son? Intergenerational educational mobility in India, Demography 52(6): 1929–1959. doi: 10.1007/s13524-015-0428-8
- Baker, D. P., J. Leon, E. G. Smith Greenaway, J. Collins, and M. Movit. 2011. The education effect on population health: a reassessment, Population and Development Review 37(2): 307–332. doi: 10.1111/j.1728-4457.2011.00412.x
- Berkman, L. F., I. Kawachi, and M. M. Glymour. 2014. Social Epidemiology. New York: Oxford University Press, pp. 1–16.
- Berkman, L., T. Sekher, B. Capistrant, and Y. Zheng. 2012. Social networks, family, and care giving among older adults in India, in J.P. Smith (ed), Aging in Asia: Findings From New and Emerging Data Initiatives. Washington, DC: The National Academies Press, pp. 261–278.
- Berniell, L., D. de la Mata, and N. Valdés. 2013. Spillovers of health education at school on parents’ physical activity, Health Economics 22(9): 1004–1020. doi: 10.1002/hec.2958
- Bloom, D. E., A. Mahal, L. Rosenberg, and J. Sevilla. 2010. Economic security arrangements in the context of population ageing in India, International Social Security Review 63(3-4): 59–89. doi: 10.1111/j.1468-246X.2010.01370.x
- Brant, R. 1990. Assessing proportionality in the proportional odds model for ordinal logistic regression. Biometrics 46(4): 1171–1178. doi: 10.2307/2532457
- Chaudhuri, A., and K. Roy. 2009. Gender differences in living arrangements among older persons in India, Journal of Asian and African Studies 44(3): 259–277. doi: 10.1177/0021909609102897
- Chen, Y., P. Persson, and M. Polyakova. 2019. The Roots of Health Inequality and The Value of Intra-Family Expertise, National Bureau of Economic Research (NBER) Working Paper No. 25618. doi: 10.3386/w25618
- Dannefer, D. 2003. Cumulative advantage/disadvantage and the life course: cross-fertilizing age and social science theory, The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 58(6): S327–S337. doi: 10.1093/geronb/58.6.S327
- De Neve, J.-W., and G. Fink. 2018. Children’s education and parental old age survival–quasi-experimental evidence on the intergenerational effects of human capital investment, Journal of Health Economics 58: 76–89. doi: 10.1016/j.jhealeco.2018.01.008
- De Neve, J.-W., G. Fink, S. V. Subramanian, S. Moyo, and J. Bor. 2015. Length of secondary schooling and risk of HIV infection in Botswana: evidence from a natural experiment, The Lancet Global Health 3(8): e470–e477. doi: 10.1016/S2214-109X(15)00087-X
- De Neve, J.-W., and G. Harling. 2017. Offspring schooling associated with increased parental survival in rural KwaZulu-Natal, South Africa, Social Science & Medicine 176: 149–157. doi: 10.1016/j.socscimed.2017.01.015
- De Neve, J.-W., and I. Kawachi. 2017. Spillovers between siblings and from offspring to parents are understudied: A review and future directions for research, Social Science & Medicine 183: 56–61. doi: 10.1016/j.socscimed.2017.04.010
- Elo, I. T., P. Martikainen, and M. Aaltonen. 2018. Children’s educational attainment, occupation, and income and their parents’ mortality, Population Studies 72(1): 53–73. doi: 10.1080/00324728.2017.1367413
- Elwert, F., and C. Winship. 2014. Endogenous selection bias: The problem of conditioning on a collider variable, Annual Review of Sociology 40(1): 31–53. doi: 10.1146/annurev-soc-071913-043455
- Emran, M. S., W. Greene, and F. Shilpi. 2018. When measure matters: Coresidency, truncation bias, and intergenerational mobility in developing countries, Journal of Human Resources 53(3): 589–607. doi: 10.3368/jhr.53.3.0216-7737R1
- Esteve, A., and C. Liu. 2017. Family and household composition in Asia, in Z. Zhao and A. Hayes (eds), Routledge: Handbook of Asian Demography, Chapter 20, pp. 370–393. Taylor & Francis Group, 563 pp.
- Frankenberg, E., L. Lillard, and R. J. Willis. 2002. Patterns of intergenerational transfers in Southeast Asia, Journal of Marriage and Family 64. doi: 10.1111/j.1741-3737.2002.00627.x
- Friedman, E. M., and R. D. Mare. 2014. The schooling of offspring and the survival of parents, Demography 51(4): 1271–1293. doi: 10.1007/s13524-014-0303-z
- Gakidou, E., K. Cowling, R. Lozano, and C. J. L. Murray. 2010. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis, The Lancet 376(9745): 959–974. doi: 10.1016/S0140-6736(10)61257-3
- Geldsetzer, P., J. Manne-Goehler, M. Theilmann, J. I. Davies, A. Awasthi, S. Vollmer, L. M. Jaacks, T. Bärnighausen, and R. Atun. 2018. Diabetes and hypertension in India, JAMA Internal Medicine 178(3. doi: 10.1001/jamainternmed.2017.8094
- Grossman, M. 1975. The correlation between health and schooling, National Bureau of Economic Research (NBER) Working Paper No. 22.
- Guzman-Castillo, M., S. Brailsford, M. Luke, and H. Smith. 2015. A tutorial on selecting and interpreting predictive models for ordinal health-related outcomes, Health Services and Outcomes Research Methodology 15(3-4): 223–240. doi: 10.1007/s10742-015-0140-6
- He, F. J., Y. Wu, X. X. Feng, J. Ma, Y. Ma, H. Wang, J. Zhang, J. Yuan, C. P. Lin, C. Nowson, and G. A. MacGregor. 2015. School based education programme to reduce salt intake in children and their families (school-EduSalt): cluster randomised controlled trial, BMJ 350(mar18 13): h770–h770. doi: 10.1136/bmj.h770
- Hirve, S. 2014. ‘In general, how do you feel today?’ – self-rated health in the context of aging in India, Global Health Action 7: 23421. doi: 10.3402/gha.v7.23421
- House, J. S., P. M. Lantz, and P. Herd. 2005. Continuity and change in the social stratification of aging and health over the life course: evidence from a nationally representative longitudinal study from 1986 to 2001/2002 (Americans’ Changing Lives study), The Journals of Gerontology: Series B 60(Spec No 2): S15–S26. doi: 10.1093/geronb/60.Special_Issue_2.S15
- Indian Council of Social Science Research. 2014. India - Social Consumption - Health Survey: NSS 71st Round. Delhi: Ministry of Statistics and Programme Implementation, Government of India.
- Jaeger, D. A., and M. E. Page. 1996. Degrees Matter: New evidence on sheepskin effects in the returns to education, The Review of Economics and Statistics 78(4): 733. doi: 10.2307/2109960
- Jiang, N. 2019. Adult children’s education and later-life health of parents in China: the intergenerational effects of human capital investment, Social Indicators Research 145(1): 257–278. doi: 10.1007/s11205-019-02109-9
- Jiang, N., and N. Kaushal. 2020. How children’s education affects caregiving: evidence from parent’s last years of life, Economics & Human Biology 38:100875. doi: 10.1016/j.ehb.2020.100875
- Jung, L., J.-W. De Neve, S. Chen, J. Manne-Goehler, L. M. Jaacks, D. J. Corsi, A. Awasthi, S. V. Subramanian, S. Vollmer, T. Bärnighausen, and P. Geldsetzer. 2019. The interaction between district-level development and individual-level socioeconomic gradients of cardiovascular disease risk factors in India: A cross-sectional study of 2.4 million adults, Social Science & Medicine 239. doi: 10.1016/j.socscimed.2019.112514
- Jylhä, M. 2009. What is self-rated health and why does it predict mortality? Towards a unified conceptual model, Social Science & Medicine 69(3): 307–316. doi: 10.1016/j.socscimed.2009.05.013
- Karlsson, O., J.-W. De Neve, and S. V. Subramanian. 2019. Weakening association of parental education: analysis of child health outcomes in 43 low- and middle-income countries, International Journal of Epidemiology 48(1): 83–97. doi: 10.1093/ije/dyy158
- Kowal, P., S. Chatterji, N. Naidoo, R. Biritwum, W. Fan, R. Lopez Ridaura, T. Maximova, P. Arokiasamy, N. Phaswana-Mafuya, S. Williams, J. J. Snodgrass, N. Minicuci, C. D'Este, K. Peltzer, J. T. Boerma, and S. Collaborators. 2012. Data resource profile: the World Health Organization study on global AGEing and adult health (SAGE), International Journal of Epidemiology 41(6): 1639–1649. doi: 10.1093/ije/dys210
- Kuziemko, I. 2014. Human capital spillovers in families: Do parents learn from or lean on their children?, Journal of Labor Economics 32(4): 755–786. doi: 10.1086/677231
- Ladusingh, L., and M. R. Narayana. 2011. The role of familial transfers in supporting the lifecycle deficit in India, in Population Aging and the Generational Economy: a Global Perspective. R. Lee and A. Mason. (Eds). pp. 459–474. Cheltenham, UK: Edward Elgar Publishing.
- Lee, Y. 2018. Adult children's educational attainment and the cognitive trajectories of older parents in South Korea, Social Science & Medicine 209: 76–85. doi: 10.1016/j.socscimed.2018.05.026
- Lee, Y. J., W. L. Parish, and R. J. Willis. 1994. Sons, daughters, and intergenerational support in Taiwan, American Journal of Sociology 99(4): 1010–1041. doi: 10.1086/230370
- Leinonen, R., E. Heikkinen, and M. Jylhä. 1998. Self-rated health and self-assessed change in health in elderly men and women – a five-year longitudinal study, Social Science & Medicine 46(4-5): 591–597. doi: 10.1016/S0277-9536(97)00205-0
- Link, B. G., and J. Phelan. 1995. Social conditions as fundamental causes of disease, Journal of Health and Social Behavior: 80–94. doi: 10.2307/2626958
- Lleras-Muney, A. 2005. The relationship between education and adult mortality in the United States, Review of Economic Studies 72(1): 189–221. doi: 10.1111/0034-6527.00329
- Lundborg, P., and K. Majlesi. 2018. Intergenerational transmission of human capital: Is it a one-way street?, Journal of Health Economics 57: 206–220. doi: 10.1016/j.jhealeco.2017.12.001
- Ma, M. 2019. Does children's education matter for parents’ health and cognition? Evidence from China, Journal of Health Economics 66: 222–240. doi: 10.1016/j.jhealeco.2019.06.004
- Mensch, B. S., E. K. Chuang, A. J. Melnikas, and S. R. Psaki. 2019. Evidence for causal links between education and maternal and child health: systematic review, Tropical Medicine & International Health 24(5): 504–522. doi: 10.1111/tmi.13218
- Meyer, A. C., H. L. Brooke, and K. Modig. 2019. The role of children and their socioeconomic resources for the risk of hospitalisation and mortality – a nationwide register-based study of the total Swedish population over the age 70, BMC Geriatrics 19(1). doi: 10.1186/s12877-019-1134-y
- National Sample Survey Office. 2014. India - Social Consumption - Health Survey: NSS 71st Round. Ministry of Statistics and Programme Implementation, Government of India.
- Peng, S., S. Bauldry, M. Gilligan, and J. J. Suitor. 2019. Older mother's health and adult children's education: Conceptualization of adult children's education and mother-child relationships, SSM - Population Health 7: 100390. doi: 10.1016/j.ssmph.2019.100390
- Pinquart, M., and S. Sorensen. 2011. Spouses, adult children, and children-in-law as caregivers of older adults: a meta-analytic comparison, Psychology and Aging 26(1): 1–14. doi: 10.1037/a0021863
- Potente, C., P. Präg, and C. Monden. 2018. Does Children’s Education Affect Parental Health and Mortality? A Regression Discontinuity Approach with Linked Census Data from England and Wales, SocArXiv (Available at: https://osf.io/preprints/socarxiv/eah4w/). doi: 10.31235/osf.io/eah4w
- Psacharopoulos, G., and H. A. Patrinos. 2018. Returns to investment in education: a decennial review of the global literature, Education Economics 26(5): 445–458. doi: 10.1080/09645292.2018.1484426
- Ross, C. E., and C. E. Bird. 1994. Sex stratification and health lifestyle: consequences for men's and women's perceived health, Journal of Health and Social Behavior 35(2): 161–178. doi: 10.2307/2137363
- Ross, C. E., and J. Mirowsky. 2010. Gender and the health benefits of education, The Sociological Quarterly 51: 1. doi: 10.1111/j.1533-8525.2009.01164.x
- Ross, C. E., and C. L. Wu. 1996. Education, age, and the cumulative advantage in health, Journal of Health and Social Behavior 37(1): 104–120. doi: 10.2307/2137234
- Sabater, A., and E. Graham. 2016. The role of children’s education for the mental health of aging migrants in Europe, GeroPsych 29: 81–92. doi: 10.1024/1662-9647/a000145
- Sabater, A., E. Graham, and A. Marshall. 2019. Does having highly educated adult children reduce mortality risks for parents with low educational attainment in Europe?, Ageing and Society: 1–36. doi: 10.1017/S0144686X19000795
- Saikia, N., J. K. Bora, and M. Luy. 2019. Socioeconomic disparity in adult mortality in India: estimations using the orphanhood method, Genus 75(1): 7. doi: 10.1186/s41118-019-0054-1
- Samanta, T., F. Chen, and R. Vanneman. 2015. Living arrangements and health of older adults in India, The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 70(6): 937–947. doi: 10.1093/geronb/gbu164
- Serrano, R., R. Saltman, and M.-J. Yeh. 2017. Laws on filial support in four Asian countries, Bulletin of the World Health Organization 95(11): 788–790. doi: 10.2471/BLT.17.200428
- Smith-Greenaway, E., S. Brauner-Otto, and W. Axinn. 2018. Offspring education and parental mortality: evidence from South Asia, Social Science Research 76: 157–168. doi: 10.1016/j.ssresearch.2018.07.001
- Subramanian, S. V., M. A. Subramanyam, S. Selvaraj, and I. Kawachi. 2009. Are self-reports of health and morbidities in developing countries misleading? Evidence from India, Social Science & Medicine 68(2): 260–265. doi: 10.1016/j.socscimed.2008.10.017
- Torssander, J. 2013. From child to parent? The significance of children’s education for their parents’ longevity, Demography 50(2): 637–659. doi: 10.1007/s13524-012-0155-3
- UK Research and Innovation. 2020. Tackling cardiovascular risk in the adolescent life-course through a schools’ salt-reduction intervention in sub-Saharan Africa, (Available at: https://gtr.ukri.org/projects?ref=MR%2FR022186%2F1).
- Umberson, D. 1992. Relationships between adult children and their parents: Psychological consequences for both generations, Journal of Marriage and the Family: 664–674. doi: 10.2307/353252
- United Nations Department of Economic and Social Affairs, Population Division. 2017. World Population Ageing 2017 (ST/ESA/SER.A/408). New York: United Nations.
- United Nations Department of Economic and Social Affairs, Population Division. 2019. World Population Prospects 2019: Data Booklet (ST/ESA/SER.A/424. New York: United Nations.
- United Nations Population Fund. 2013. Building a Knowledge Base on Population Ageing in India: Report on the Status of Elderly in Select States of India, 2011. New Delhi, India: United Nations.
- Williams, R. 2006. Generalized ordered logit/partial proportional odds models for ordinal dependent variables, The Stata Journal: Promoting Communications on Statistics and Stata 6(1): 58–82. doi: 10.1177/1536867X0600600104
- Wolfe, J. D., S. Bauldry, M. A. Hardy, and E. K. Pavalko. 2018. Multigenerational attainment and mortality among older men: An adjacent generations approach, Demographic Research 39: 719–752. doi: 10.4054/DemRes.2018.39.26
- Yahirun, J. J., C. M. Sheehan, and M. D. Hayward. 2016. Adult children's education and parents’ functional limitations in Mexico, Research on Aging 38(3): 322–345. doi: 10.1177/0164027515620240
- Yahirun, J. J., C. M. Sheehan, and M. D. Hayward. 2017. Adult children's education and changes to parents’ physical health in Mexico, Social Science & Medicine 181: 93–101. doi: 10.1016/j.socscimed.2017.03.034
- Yahirun, J. J., C. M. Sheehan, and K. N. Mossakowski. 2020. Depression in later life: The role of adult children’s college education for older parents’ mental health in the United States, The Journals of Gerontology: Series B 75(2): 389–402. doi: 10.1093/geronb/gby135
- Zimmer, Z., H. A. Hanson, and K. R. Smith. 2016. Offspring socioeconomic status and parent mortality within a historical population, Demography 53(5): 1583–1603. doi: 10.1007/s13524-016-0502-x
- Zimmer, Z., A. I. Hermalin, and H.-S. Lin. 2002. Whose education counts? The added impact of adult-child education on physical functioning of older Taiwanese, The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 57(1): S23–S32. doi: 10.1093/geronb/57.1.S23
- Zimmer, Z., L. G. Martin, M. B. Ofstedal, and Y.-L. Chuang. 2007. Education of adult children and mortality of their elderly parents in Taiwan, Demography 44(2): 289–304. doi: 10.1353/dem.2007.0020