
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Vietnam was previously lauded as a model for fighting the COVID-19 pandemic and it imposed localized lockdowns to deal with the emergence of deadly new variants. Here, daily data from 63 Vietnamese provinces for the period January–July 2021 (i.e., before vaccinations became available) are collected, and a panel event study is performed to evaluate the effectiveness of the localized lockdown policy. The number of infected cases is found to increase despite the lockdowns reducing visits to public areas. These results have implications for the lateness of the localized lockdowns and strictness of social distancing.
KEYWORDS:
1. INTRODUCTION
Although Vietnam’s model for fighting COVID-19 attracted researchers’ attention in the first and second waves of the pandemic, the emergence of the Delta variant changed the story. While New Zealand immediately locked down the entire country with one confirmed case, Vietnam was reluctant to follow suit because of its twin objectives of containing the pandemic while minimizing disruption in economic activities.Footnote1 Therefore, the Vietnamese government decided to apply localized lockdowns in areas with confirmed cases. Especially in the context of the Delta variant, effective approaches that helped contain the coronavirus in previous waves might no longer work. Does a heterogeneous lockdown policy at the province level contain the deadly spread of new variants? Motivated by the different approaches of Vietnam and New Zealand, this study investigates whether infected cases declined after multiple lockdown dates in different areas.
In contrast to many other countries, Vietnam applied two different lockdown policies at separate times: once in March 2020 at very early stages of the pandemic in 63 provinces (Huynh, Citation2020a), and another in May 2021 with sporadic execution (for more details, see Appendix A in the supplemental data online). It is argued that inconsistent policies may undermine effective responses to the COVID-19 pandemic. However, it is difficult to determine how the number of cases would be affected if the lockdown had been implemented earlier. Therefore, this study sheds light on the effectiveness of localized lockdown and reports evidence of an increase in infected cases after the adoption dates. In addition, Long et al. (Citation2021) find evidence of the limited effect of regionally targeted lockdowns on human mobility, but this study does not consider the linkage between COVID-19 cases and death rates in Canada. Theoretically, the interrelationship between mobility and localized lockdowns could affect COVID-19 incidence and mortality.
As discussed above, this study first contributes to the literature on COVID-19 by examining whether localized lockdowns of specific regions in Vietnam actually help reduce the infection rate through affecting interregional mobility. In addition, not only does the paper evaluate the effectiveness of public health policies before having pharmaceutical interventions such as mass-vaccination campaigns, but also it extends the debates related to the effectiveness of stringent lockdowns widely adopted in China as part of its consistent zero-COVID policy (Yuan, Citation2022). Non-pharmaceutical interventions have initially been introduced to mitigate the spread of coronavirus from individual-level recommendations (i.e., wearing masks, hand sanitizers, etc.) to society-level regulatory actions (i.e., mandatory quarantine, school-office closures, localized as well as national lockdowns, etc.). However, the efficacy of these policies is far from uniform across countries. For example, Carranza et al. (Citation2022) find that the effects of localized lockdown in Chile significantly depend on the rate of mobility and socio-economic factors. By contrast, Long et al. (Citation2021) reveal that using regionally targeted interventions has a neutral (or even no) effect on the mobility. Arguably, the evaluation of health policies critically requires examining a variety of contexts, using various data samples and exploiting reliable identification strategies. Second, this study contributes to the growing literature by documenting evidence of the effectiveness of localized lockdowns in Vietnam. While other studies examine the first or second wave of COVID-19 in 2020 (Long et al., Citation2021; Carranza et al., Citation2022), this paper provides a novel finding about the effectiveness of localized lockdowns in response to the emergence of the Delta variant in a recent wave of the COVID-19 pandemic. Vietnam had applied the national lockdown in the first and second waves; however, the policy changed due to the trade-off between pandemic containment and economic growth. To sum up, the novelty of this study lies on two main pillars: (1) exploring the effectiveness of localized lockdowns implemented to reduce human mobility while maintain the resilience of the public health system and achieve robust economic growth; and (2) examining the efficacy of responses to containing the Delta variant in Vietnam.
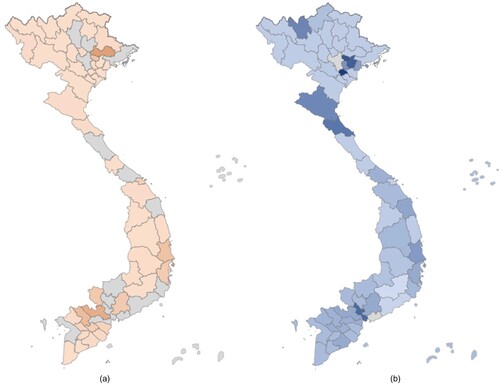
There are two possible reasons for an increase in cases. First, a localized lockdown may be too late to prevent community-acquired infection. However, this explanation rests upon the observation that the lockdown policy response should be rapidly applied at the national scale as in the first wave of COVID-19 (Nguyen et al., Citation2021). At that time, Vietnam successfully contained the spread of the coronavirus and became the role model. However, Vietnam changed its approach from a comprehensive national lockdown to localized lockdowns in 2021 to maintain two goals: economic growth and virus containment. Thus, the national lockdown was not implemented when the Delta variant emerged. Second, provinces without localized lockdowns would experience increased risk of exposure to the virus. This study explored the differences between the north and south regions of Vietnam in terms of compliance and infected cases. illustrates the inconsistent lockdown policies of 63 Vietnamese provinces. The northern provinces tended to apply strict lockdown policies, while the southern provinces did not. also shows the spatial heterogeneity of the third wave of the pandemic in Vietnam, which was driven by the Delta variant. During this wave, Vietnam had an extremely low vaccination rate of below 1%. Therefore, the number of cases was not affected by pharmaceutical interventions. This quasi-natural experiment permits identifying the effectiveness of the localized lockdown policy in Vietnam.
Figure 1. Differences in (a) cases per capita and (b) lockdown days among the 63 provinces of Vietnam.
Note: Lighter colours represent fewer infected cases and lockdown days; dark colours represent the opposite. The number of lockdown days was calculated from the difference between the implementation of Directive No. 16/CT-TTg and 29 July 2021 (i.e., last day of non-pharmaceutical intervention).
The remainder of this paper is organized as follows. Section 2 briefly summarizes the current literature on the causes and consequences of lockdowns. Section 3 presents the data and methodology. Section 4 discusses the empirical results and policy debate. Section 5 concludes.
2. LITERATURE REVIEW
A central question related to the COVID-19 pandemic for policymakers has been the efficacy of lockdowns. A particular issue is when to implement a lockdown. Delaying any actions would allow the virus to spread owing to its long incubation period (Wang et al., Citation2020). Thus, taking action sooner would improve the efficacy. Based on provincial data from Italy, Bourdin et al. (Citation2021) argue that the early lockdown at the beginning of March 2020 played a crucial role in curbing COVID-19 transmission. Their finding is consistent with other studies using different global and subnational datasets (Ullah, Citation2020). In this context, Karnon (Citation2020) develop a decision framework for policymakers to implement an immediate and mandatory lockdown. This framework assumes that choosing a later lockdown is worse than implementing a sooner and immediate lockdown across all scenarios. In contrast, Coccia (Citation2021) concludes that a longer lockdown does not significantly reduce fatalities but does significantly hurt the economy.
Note that most empirical studies have focused on the first or second waves of COVID-19 in 2020. East Asian countries implemented policies that appeared to promptly and effectively contain the spread of COVID-19 when it started in 2020 (Jin et al., Citation2021). Many countries such as Taiwan, China and Vietnam chose to follow zero-COVID policies of eliminating any single infected cases until pharmaceutical interventions such as vaccinations became available. Because of their success during the first and second waves, these countries felt that the situation was sufficiently stable to focus on economic resilience and gradually reopened their borders. However, their governments then faced the challenge of an unexpected outbreak of confirmed cases and had to decide whether to respond to that with an immediate or delayed lockdown.
To assess the effectiveness of lockdown measures, there are many perspectives that both scientists and policymakers need to consider. A relevant framework must take into consideration the trade-off between economic loss and human life. Caulkins et al. (Citation2021) model an optimal lockdown policy that allows the healthcare system to manage COVID-19 cases. They also argue that implementing a new lockdown after lifting initial restrictions should not be considered as a sign of policy failure. However, their theoretical model does not capture the interaction between the economy and pandemic. Devendra and Kandhway (Citation2022) select Burundi, India and the United States to represent three levels of economic conditions and tune the model parameters to incorporate the economic situation. Their model emphasizes the flexibility of switching between partial and complete lockdowns in the event of a significant increase in confirmed cases. Therefore, the above literature indicates that the economic conditions should be considered as a determinant of the effectiveness of lockdown policies.
Spatial factor analysis has been used to investigate the heterogeneity of COVID-19 waves across regions or countries. Bourdin et al. (Citation2021), by performing a geographical study, show that an effective global health network could be a crucial element for coping with the spread of COVID-19. They identify a concentrated hub in Northern Italy, while the effects seem weaker in Southern Italy. Although their initial hypothesis is based on gradual spatial homogeneity, they do not find any evidence of the best timing to implement a lockdown. McCann et al. (Citation2021) and Rodríguez-Pose and Burlina (Citation2021) explore whether geographical characteristics could predict the excess mortality related to COVID-19 in Europe. They show that the socio-economic interactions between economic geography and institutional setup play an important role in shaping COVID-19 outcomes of European countries. Although these two studies do not focus on national-level policy decisions, Hsiang et al. (Citation2020) point out that the timely deployment of policy packages could decrease the spreading speed of COVID-19 and improve health outcomes. This finding is partially supported by Bargain and Aminjonov (Citation2020) who study 233 regions in 19 European countries. Therefore, applying an earlier lockdown might mitigate the spread of COVID-19. I also acknowledge the limitation of this study, which could not explain whether the policy could work well if the lockdown policies had been imposed earlier. However, some countries delayed implementing lockdowns because they could hurt the economy. During the first and second waves of COVID-19, Vietnam achieved remarkable economic growth (Weber & Huynh, Citation2022), which may explain why the government did not implement a broad lockdown to minimize economic loss. In contrast, Michie (Citation2020) argue that human life is of paramount importance, so saving lives must come first.
3. DATA AND RESEARCH DESIGN
In the present study, data are collected from 63 provinces in Vietnam to examine the effectiveness of lockdown policies. In particular, I perform a panel event study to evaluate the effectiveness of the localized lockdown policy. Using different research designs, I consistently obtain the null results. Provinces without lockdown are considered as the control group, and the treated group includes provinces that did implement a localized lockdown. It was observed that people in provinces under lockdown reduces their interactions and visits to public areas but increased their time in residential areas after the event date.
Based on a review of the existing literature, the determinants of COVID-19 incidence include population density (McCann et al., Citation2021; Bourdin et al., Citation2021), provincial competitiveness index,Footnote2 the average number of hospital beds (Feng et al., Citation2022), and dummy variables for the holiday period (i.e., New Year, Lunar new year and Independence Day). The rationale to include the holiday period dummy variable in the regression is greater social interactions during this special period (Plümper & Neumayer, Citation2021). Arguably, COVID-19 incidence can be higher over the holiday period and the effect could last after two weeks after the ending date of holiday. Therefore, the model does not only incorporate the holiday period dummy but also binary variables for periods following holiday time (after seven and 14 days). The objective is to evaluate the effectiveness of a flexible lockdown (i.e., partial restrictions) on the number of infected cases in Vietnam.
Information is collected from a massive dataset of COVID-19 mobility reports from Google in Vietnam at the provincial level. The reports provide daily data of mobile device users based on their locations, which measure the types of visits, length of stays and different geographies over a specific period compared with the baseline period. Locations could be divided into six groups:Footnote3 retail and recreation, groceries and pharmacies, parks (e.g., public gardens, dog parks, beaches), public transit stations (e.g., for subways, buses and trains), workplaces and residential areas. Due to their usefulness for COVID-19 research, the Google Mobility reports have been widely used in academic studies (Mendolia et al., Citation2021; Brodeur et al., Citation2021). Huynh (Citation2020b) constructs an uncertainty avoidance index and shows that people in countries with high scores tend to follow social distancing rules by staying at home. Long et al. (Citation2021) employ the same indicator to study the reduction in human mobility. It is worth mentioning that including six indicators of Google Mobility in one single regression could result in multicollinearity. Therefore, the principal component analysis (PCA) was used to construct two new indices in our regressions, which is used in the current literature (Huynh, Citation2020b; Chen et al., Citation2023). The detailed procedures to obtain the Mobility 1 and Mobility 2 are provided in .
Concomitantly, legal documents are manually collected to identify when provinces implemented lockdowns, which corresponds to the date that local authorities approved Directive No. 16/CT-TTg (see Table A1 in Appendix A in the supplemental data online). The study period is between 1 January and 29 July 2021. Other control variables include population density, the provincial competitiveness index, the average number of hospital beds and dummy variables for holiday periods. Table A2 online contains descriptive statistics of all variables.
To test whether Directive No. 16/CT-TTg effectively reduced the number of infected cases, a panel event study is designed with lag and lead terms (Freyaldenhoven et al., Citation2019). This method is also known as the dynamic difference-in-differences.Footnote4 The existence of post-event indicators across all period’s posterior to the occurrence of an event (i.e., application of Directive No. 16/CT-TTg) within a province can be defined as follows:
(1)
(1) where cases represents the number of infected cases in province i at day t. In addition,
,
and
are the province and time fixed effects, and the residual term, respectively.
is a vector of time-varying control variables. The lag and lead to the event of interest can be defined as follows:
(2)
(2)
(3)
(3) Typical lag and lead periods are 14 and 21 days because the horizon of Directive No. 16/CT-TTg was 14 days. These variables capture the temporal and geographical fixed effects in equation (1), as suggested by Duflo (Citation2004). More specifically, leads and lags are dummy variables that indicate the number of days away from the lockdown date for each province. This study also chooses the baseline reference period as the first lag variable. This model is an extension of the difference-in-difference approach that helps evaluate the effect of policy from the lockdown date. However, various provinces applied different lockdown dates with different situations (e.g., Thua Thien Hue strictly applied Directive No. 16/CT-TTg on 13 July 2021 with zero case, while Binh Duong executed on 19 July 2021 with 503 cases). Therefore, the differences in the number of infected cases between the control (non-lockdown) and treated (lockdown) groups are allowed to vary over different periods. The inclusion of lead and lag dummy variables in the regression permits estimating the difference between the treated and control groups in a specific period compared with that in the baseline omitted period (the first lag is omitted as the base period). While the conventional difference-in-difference considers the average difference between two groups with the cut-off point (before and after treatment effect), the panel event study offers the evolving differences between control and treated groups over time, relative to the omitted period.Footnote5
The panel event study approach was used to evaluate the effectiveness of lockdowns implemented in Vietnam for two reasons. First, different provinces chose to implement the lockdown at different dates, so including lead and lag terms could capture the difference in infected cases between lockdown provinces and non-lockdown ones, compared with the prevailing difference in the omitted base period (the first lag, j = 1). Second, the endogeneity problem with panel data could be resolved. Without addressing this problem, the empirical findings may interfere with causal relationships indicating the effectiveness of a lockdown policy. This approach has been widely applied in previous studies (Angrist & Jörn-Steffen, Citation2009; Clarke & Kathya, Citation2022; Freyaldenhoven et al., Citation2019; Goodman-Bacon, Citation2018; Stevenson & Justin, Citation2006). Background data are included from previous studies to check the preliminary trends of the lead and lag effects and confirm that the coefficients are jointly statistically different to zero. To mitigate the effects of a large population the number of infected cases was divided by the provincial population, and the panel event study approach is applied again to validate the results for further policy debates.
4. RESULTS AND DISCUSSION
4.1. Empirical findings
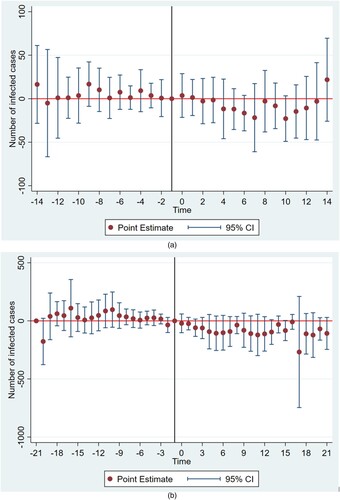
The current literature explores the impact of non-pharmaceutical interventions on public health (Lai et al., Citation2020). In Sweden, Cho (Citation2020) shows that the number of infected cases may change on days 7, 14 and 20 depending on the incubation period. Using the European data, Flaxman et al. (Citation2020) fully identify infection trends two to three weeks ahead of time. In the present study, the event study is performed for the time intervals [−14, 14] and [−21, 21] days. plots the point estimates and confidence intervals of the lag and lead dummy variables. The figure shows an overall reduction in infected cases with an insignificant decline 14 and 21 days following localized lockdowns. Most post-event coefficients are negative but statistically insignificant at conventionally accepted levels. This implies that the provincial-level lockdown policy was not effective in reducing the number of COVID-19 cases.
Figure 2. Effects of localized lockdown on the number of infected cases.
Note: Results from the panel event study are shown. Point estimates are represented along with their 95% confidence intervals as described in the model equation in specific time intervals and controlling for residential mobility and national holidays. The baseline (omitted) base period (solid vertical line) was one day before the adoption of a localized lockdown by each province. The event date was when each province applied Directive No. 16/CT-TTg (i.e., strict social distancing measures) to contain the spread of COVID-19.
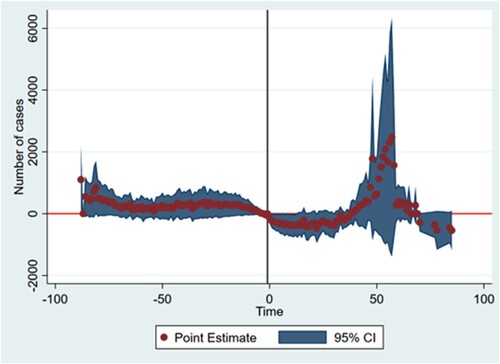
For the following analysis, the temporal and geographical fixed effects are considered with all lag and lead terms to interpret the entire sample period. As shown in , the initial finding of the ineffectiveness of localized lockdowns in Vietnam is confirmed. The results regarding the timing are somewhat alarming; the number of infected cases tended to decrease in the 14 days following the event date, but the trend reversed and spiked around day 50. These results are consistent with the current literature showing that localized lockdowns may not effectively contain the spread of the Delta variant. Furthermore, they may indicate that the infection rate may be deeply connected to community-acquired transmission and that lockdowns were probably implemented too late. As shown in Figure A1 in Appendix A in the supplemental data online, people became less likely to gather in public areas and more likely to stay at home during lockdowns, but the compliance eased after 50 days. This phenomenon challenges policymakers when it comes to determining when to lift a lockdown at the provincial level. Mobility among provinces may have been a factor driving the increase in infected cases.
Figure 3. Effects of localized lockdown on the number of infected cases considering fixed effects.
Note: Results from the panel event study are shown considering multiple levels of fixed effects. Point estimates are represented along with their 95% confidence intervals as described in the model equation in specific time intervals and controlling for residential mobility (estimated by principal component analysis) and national holidays.
Subsample analysis is performed for two regions that differ in politics and history: the North (i.e., socialist) and South (i.e., capitalist). After localized lockdowns, the number of infected cases tended to decrease in the first 25 days. However, this effect was not pronounced in the North, and differences were not significant (see Figure A2 in Appendix A in the supplemental data online). People in the South, where the culture is more individualistic and democratic, showed more persistent compliance after the event date than their counterparts in the North (see Figure A3 online). The conventional difference-in-differences approach (control group: 20 provinces; treatment group: 41 provinces) is applied, and the effects are averaged to check for the robustness of my findings. Negative but statistically insignificant coefficients are obtained, which supports the existing literature that early and tight lockdowns may save lives (Caselli et al., Citation2022). More precisely, a stringent lockdown policy may be better than mild but prolonged measures in the short term. The robustness of the results is checked by normalizing the cases against the population size of each province. As shown in , the robustness is confirmed. The post-estimation results in indicate that the null hypothesis (i.e., all lead and lag coefficients are equal to zero) can be rejected. Therefore, the null effects were concluded reliable for further analysis and discussion.
Figure 4. Effects of localized lockdown on the cases per population considering fixed effects.
Note: Results from the panel event study are shown considering multiple levels of fixed effects with cases per population. Point estimates are represented along with their 95% confidence intervals as described in the model equation in specific time intervals and controlling for residential mobility (estimated by principal component analysis – PCA) and national holidays.
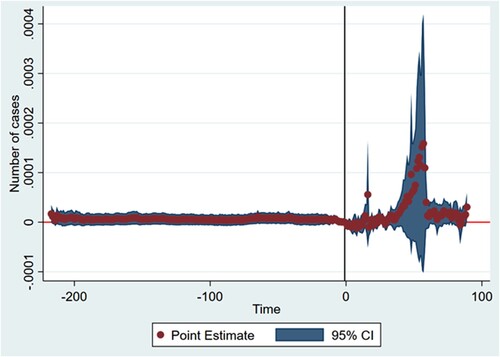
Table 1. Post-estimation test for the joint significance of leads, lags and event terms.
When looking at other determinants in , I find that staying at home and workplaces, proxied by the Mobility 2 variable, could predict a significant drop in the number of infected cases at the 5% level of statistical significance. Arguably, people were more likely to spend time in their residence when the lockdown policy was executed. It is interesting to discuss the effectiveness of the ‘3-in-place’ policy (work, quarantine and stay at one place) implemented by the Vietnamese government.Footnote6 The employees were not able to leave the workplace for roughly seven-day shifts. That is the main reason to aggregate two indicators of ‘residence’ and ‘workplaces’ for the regression, which predicts the lower infected cases when having an increase in these areas. In addition, only population density has a predictive power on the COVID-19 cases at the 1% level of statistical significance. It is intuitive that population density is positively associated with COVID-19 incidence because social interactions could be more intensive in densely populated provinces. This finding is also consistent with previous studies (McCann et al., Citation2021; Bourdin et al., Citation2021). However, the health system capacity and local governance, proxied respectively by the number of hospital beds and provincial competitiveness index, have no statistically significant effect on infected cases. When it comes to discussing the temporal effect in Figure A4 in Appendix A in the supplemental data online, there was a difference in the average number of infected cases between lockdown and non-lockdown provinces. Figure A4 depicts the estimated mean and confidence interval of COVID-19 cases for lockdown and non-lockdown provinces between 27 April and 29 July 2021. It demonstrates that there are no significant differences in average cases between the two groups before July 2021. However, after July 2021, the number of cases in lockdown provinces is higher than that in non-lockdown ones. In addition, the confidence interval for the lockdown group is greater than that for the remaining group after July 2021. A potential explanation is that there exists higher variation in the number of cases between provinces in the lockdown group. Therefore, instead of using the traditional difference-in-differences estimator focusing on the average differences before and after the cutting point, the data illustrated in Figure A4 online at least partially motivate the adoption of the panel event study to account for differences between two groups from the temporal perspective.
Table 2. Estimation results of mobility and socio-economic factors on the number of infected cases.
4.2. Policy debate
4.2.1. Failure of the localized lockdown policy
The main results are in line with Long et al. (Citation2021) who focus on Ontario in Canada. They conclude that locally targeted interventions do not affect interregional mobility. This implies that the failure of a lockdown policy is predictable when applied at the district scale (e.g., Go Vap District) instead of the city or country levels (Paddock & Doan, Citation2021).
The failure to maintain no community-acquired transmission of COVID-19 cases opens a new chapter in Vietnam’s policy debate. The late response to the Delta variant probably led to a massive and ongoing outbreak in Vietnam. This caused the Vietnamese government to shift from a ‘zero-COVID’ policy to a ‘living with COVID’ policy (Reed & Pham, Citation2021). After two years, Vietnam has resumed international flights to recover tourism and economic activities. In contrast, China has maintained closed borders and been persistent in its zero-COVID policy (Mallapaty, Citation2022). Until the 2022 Olympics, the Chinese government has pursued a policy of responding swiftly to infected cases. However, at present China has more than 14 provinces and cities (including Beijing) experiencing cases due to the Omicron variant (Mallapaty, Citation2022). Silver (Citation2021) finds it difficult to understand why China is sticking to a zero-COVID policy when its vaccination rate is nearly 75%. Although some countries such as Australia and New Zealand that followed the no-cases approach have outperformed expectations, these countries have now shifted to a ‘living with COVID’ approach. Evaluating the costs and benefits of the different approaches is not easy for policymakers. Their choice should rely on the feasibility of a policy and the availability of pharmaceutical interventions such as vaccinations or other treatments.
4.2.2. Inconsistency in the localized lockdown policy
It is easy to assume that Vietnam maintained a consistent policy from the central government to the local authorities. It may be surprising that each province was allowed to implement a lockdown at its own discretion (New Straits Times, Citation2021). For example, some bars, restaurants, and shopping centres remained open in some provinces, but they were forced to close in other provinces. The mobility data showed no reduction in movement with regional-scale lockdowns, so the number of cases can be expected to increase. Therefore, Vietnam did not take serious actions to trace and reduce the number of community-acquired infected cases. McCann et al. (Citation2021) and Rodríguez-Pose and Burlina (Citation2021) find that COVID-19 outbreaks could be driven by geographical and institutional features. This confirms that understanding low-level local features could lead to better policies. For example, different regions may have their own levels of urbanization, subnational governance, healthcare capacity, etc. These determinants could simultaneously interact with each other and influence COVID-19 outcomes. Overall, the same model should not be applied to all regions. However, any lockdown policy for preventing sudden increases in the number of infected cases should be applied consistently and in a timely manner to reduce unnecessary social interactions.
4.2.3. Optimal policy
Formulating an optimal policy is difficult. Using subnational data for Vietnam, I demonstrate that a timely lockdown policy was not implemented although the effectiveness of the vaccination campaign was not considered. However, the Vietnamese government should be able to address this concern despite its stumbles. One point of emphasis is its desire to recover its economy and avoid the middle-income trap. It is also a lesson of income shock from the Spanish data (Palomino et al., Citation2022). However, it is still struggling to satisfy its twin objectives of resuming economic activities by living with COVID-19 and suppressing the numbers of total and severe cases below the capacity of the public health system. Adapting to new situations after policy failure is key to developing the economy and controlling the COVID-19 situation, especially with vaccines now becoming widely available.
As of 17 July 2022, China is still applying strict lockdown policies, even a slight tweak,Footnote7 while Vietnam has lifted all COVID-19 restrictions, including mandatory testing on arrival and before departure.Footnote8 In comparison with other countries, Vietnam is more likely to adapt with the flexible policy about COVID-19. After achieving good vaccination coverage, Vietnam has resumed economic activities and reopened the border to welcome foreign tourists. The national lockdown or localized lockdown has been considered as the non-pharmaceutical intervention before the vaccine appearance to contain the spread of COVID-19. However, policy should be flexibly adopted depending on whether the proportion of the population that has been vaccinated may help balance the economic costs and the resilience of the public health system. One of main reasons that China does not follow the ‘dynamic zero-COVID policy’ is the unpredictability of morbidity differences in different cities (Dai & Dai, Citation2022; Yuan, Citation2022). This also puts enormous pressure on the Chines economy while the other economies started considering the economic resiliency and supply chain disruption (Tian et al., Citation2022).Footnote9 A lesson for other countries is to flexibly adjust the lockdown policies. One infected case has been founded; the immediate national lockdown could be applied as the case of New Zealand on 17 August 2021. If not, the vaccination rate could help because the higher vaccination reduces the COVID-19 mortality (Van Nguyen et al., Citation2021). There is no optimal policy to deal with the emergence of new variants of the coronavirus, but we can flexibly choose the policy based on the capacity of the public health system.
4.3. Further discussion
While this study focuses on responses to the Delta variant, the world is currently facing several challenges from the Omicron and other variants of the coronavirus. The failure of the localized lockdown policy resulted in Vietnam restarting all economic activity instead of continuing the zero-COVID policy. Although the daily number of infected cases in Vietnam reached 95,300, the government has decided to live with COVID-19. Karim and Karim (Citation2021) suggest that the Omicron variant would open a new chapter in the story of the pandemic. This is true for Vietnam, which changed its policy after failing to control community-acquired infection. Therefore, the findings for this study come with the caveat that the scope was limited to the Delta variant.
This paper contributes to the existing literature on the effectiveness of lockdown policies, in which there is still controversy over the trade-off between economic loss and human lives. The findings provide important insights into avoiding inappropriate policies when new COVID-19 variants appear. Concomitantly, the study extends discussions of regions in a time of pandemic with the Vietnam data (Bailey et al., Citation2020).
There are several caveats for the policy debate during the COVID-19 period. First, this study indicates that the localized lockdowns did not work well, and the lateness could be speculated as one of main reasons. However, it is not easy to disentangle if the early lockdown could help or not because there are enormous confounding factors such as the type of coronavirus, the number of incubation cases in the society, etc. Therefore, the caveat could indicate that we might overestimate the timeliness of lockdown or the stringency of policy while the other factors might be overlooked. Second, what holds true currently might not work with the future situation. For example, the lockdown is only applied when there are no pharmaceutical interventions (vaccines, or treatment medicines). However, visionary policies might be changed when having these factors; for example, from zero-COVID to living with COVID. Therefore, this study also provides empirical evidence of localized lockdown policy in terms of the Delta variant in Vietnam, and everything happens before the mass vaccination campaign.
5. CONCLUSIONS
The localized lockdown policy appeared to have failed to contain the spread of the Delta variant. This painful lesson from Vietnam should be heeded by other countries in the context of emerging variants of concern (e.g., Mu, Gamma). Vietnam has followed a zero-COVID policy since March 2020 of suppressing any infections in the community. The failure of the lockdown policy forced Vietnam to consider vaccinations and to shift to a living-with-COVID approach and reopen the economy. However, the present study was limited between January and July 2021 when the zero-COVID policy was in effect and no vaccines were available. Therefore, the panel event study approach with dynamic treatment groups captures the null results better rather than considering the moderating effects of pharmaceutical interventions. This study also discusses the crucial shift from the zero-COVID approach to living with COVID approach. The appearance of COVID-19 affected all public economic policies.
The main limitation of this study originates from data availability. Because research on COVID-19 in Vietnam is not systematically structured, collecting a comprehensive dataset is challenging. Future research may exploit data measured at lower levels such as ward, district, city, etc. In addition, advanced econometric models are needed to update or even to learn the pattern of infected cases or mortality. For example, the machine learning or big data could be advantageous in the future direction. Concomitantly, future research should focus on developing new pathways for economic resiliency in specific areas (Bailey et al., Citation2020; Bailey et al., Citation2021).
Supplemental Material
Download PDF (786.5 KB)ACKNOWLEDGEMENTS
I am grateful for helpful comments from Klaus F. Zimmermann, Erdal Tekin, Hendrik Schmitz, Phil Tomlinson, Damian Clarke, Trung Vu, Khanh Hoang and the seminar participants at the University of Economics Ho Chi Minh City (Vietnam). I also thank two anonymous reviewers for several useful suggestions that substantially improved the article. I also greatly acknowledge Thach N. Ly, Minh Huyen Dao, Duc V. Nguyen and Duy Duong for preparing the data and excellent research assistance. All errors are my own.
DATA AVAILABILITY
The data are available from the author upon request.
DISCLOSURE STATEMENT
No potential conflict of interest was reported by the author.
Additional information
Funding
Notes
2. The main motivation is that the provincial competitiveness index is a proxy for the quality of local governance (Nguyen et al., Citation2018). I conjecture that provinces with better governance quality could take sooner actions to contain the spread of the coronavirus. The relationship between local governance and COVID-19 incidence has been explored in several studies (Dutta & Fischer, Citation2021; McCann et al., Citation2021). Accordingly, strong local governance is associated with a reduction in COVID-19 cases and mortality.
3. This classification by Google Mobility is based on the default different categories of places by the Google reports; https://www.google.com/covid19/mobility/?hl=en/.
4. I am grateful to Nick C. Huntington-Klein who suggested this terminology for precisely calling the method.
5. I thank an anonymous referee for pointing out the insightful suggestion.
6. Resolution No. 88/NQ-CP issued by the Prime Minister of Vietnam Government on 12 August 2021.
REFERENCES
- Angrist, J., & Jörn-Steffen, P. (2009). Mostly harmless econometrics: An empiricist’s companion. Princeton University Press.
- Bailey, D., Clark, J., Colombelli, A., Corradini, C., De Propris, L., Derudder, B., Fratesi, U., Fritsch, M., Harrison, J., Hatfield, M., Kemeny, T., Kogler, D. F., Lagendijk, A., Lawton, P., Ortega-Argilés, R., Otero, C. I., & Usai, S. (2020). Regions in a time of pandemic. Regional Studies, 54(9), 1163–1174. https://doi.org/10.1080/00343404.2020.1798611
- Bailey, D., Crescenzi, R., Roller, E., Anguelovski, I., Datta, A., & Harrison, J. (2021). Regions in COVID-19 recovery. Regional Studies, 55(12), 1955–1965. https://doi.org/10.1080/00343404.2021.2003768
- Bargain, O., & Aminjonov, U. (2020). Trust and compliance to public health policies in times of COVID-19. Journal of Public Economics, 192, 104316. https://doi.org/10.1016/j.jpubeco.2020.104316
- Bourdin, S., Jeanne, L., Nadou, F., & Noiret, G. (2021). Does lockdown work? A spatial analysis of the spread and concentration of COVID-19 in Italy. Regional Studies, 55(7), 1182–1193. https://doi.org/10.1080/00343404.2021.1887471
- Brodeur, A., Gray, D., Islam, A., & Bhuiyan, S. (2021). A literature review of the economics of COVID-19. Journal of Economic Surveys, 35(4), 1007–1044. https://doi.org/10.1111/joes.12423
- Carranza, A., Goic, M., Lara, E., Olivares, M., Weintraub, G. Y., Covarrubia, J., Escobedo, C., Jara, N., & Basso, L. J. (2022). The social divide of social distancing: Shelter-in-place behaviour in Santiago during the COVID-19 pandemic. Management Science, 68(3), 2016–2027. https://doi.org/10.1287/mnsc.2021.4240
- Caselli, F., Grigoli, F., & Sandri, D. (2022). Protecting lives and livelihoods with early and tight lockdowns. The B.E. Journal of Macroeconomics, 22(1), 241–268. https://doi.org/10.1515/bejm-2020-0266
- Caulkins, J. P., Grass, D., Feichtinger, G., Hartl, R. F., Kort, P. M., Prskawetz, A., Seidl, A., & Wrzaczek, S. (2021). The optimal lockdown intensity for COVID-19. Journal of Mathematical Economics, 93, 102489. https://doi.org/10.1016/j.jmateco.2021.102489
- Chen, K., Pun, C. S., & Wong, H. Y. (2023). Efficient social distancing during the COVID-19 pandemic: Integrating economic and public health considerations. European Journal of Operational Research, 304(1), 84–98. https://doi.org/10.1016/j.ejor.2021.11.012
- Cho, S. W. (2020). Quantifying the impact of nonpharmaceutical interventions during the COVID-19 outbreak: The case of Sweden. The Econometrics Journal, 23(3), 323–344. https://doi.org/10.1093/ectj/utaa025
- Clarke, D., & Kathya, T. (2022). Implementing the panel event study. The Stata Journal: Promoting Communications on Statistics and Stata, 21(4), 853–884. https://doi.org/10.1177/1536867X211063144
- Coccia, M. (2021). The relation between length of lockdown, numbers of infected people and deaths of COVID-19, and economic growth of countries: Lessons learned to cope with future pandemics similar to COVID-19 and to constrain the deterioration of economic system. Science of The Total Environment, 775, 145801. https://doi.org/10.1016/j.scitotenv.2021.145801
- Dai, Y., & Dai, B. (2022). Data analysis and research reveal the reasons why China still adheres to its ‘dynamic zero-COVID policy’ (Working Paper). https://doi.org/10.21203/rs.3.rs-1532279/v4
- Devendra, J. K., & Kandhway, K. (2022). Optimal lockdown to manage an epidemic. In 2022 14th international conference on COMmunication systems & NETworkS (COMSNETS) (pp. 784–788). IEEE. https://doi.org/10.1109/COMSNETS53615.2022.9668495
- Duflo, E. (2004). The medium run effects of educational expansion: Evidence from a large school construction program in Indonesia. Journal of Development Economics, 74(1), 163–197. https://doi.org/10.1016/j.jdeveco.2003.12.008
- Dutta, A., & Fischer, H. W. (2021). The local governance of COVID-19: Disease prevention and social security in rural India. World Development, 138, 105234. https://doi.org/10.1016/j.worlddev.2020.105234
- Feng, Q., Wu, G. L., Yuan, M., & Zhou, S. (2022). Save lives or save livelihoods? A cross-country analysis of COVID-19 pandemic and economic growth. Journal of Economic Behavior & Organization, 197, 221–256. https://doi.org/10.1016/j.jebo.2022.02.027
- Flaxman, S., Mishra, S., Gandy, A., (2020). Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature, 584(7820), 257–261. https://doi.org/10.1038/s41586-020-2405-7
- Freyaldenhoven, S., Hansen, C., & Shapiro, J. M. (2019). Pre-event trends in the panel event-study design. American Economic Review, 109(9), 3307–3338. https://doi.org/10.1257/aer.20180609
- Goodman-Bacon, A. (2018). Difference-in-differences with variation in treatment timing (Working Paper No. 25018). National Bureau of Economic Research (NBER).
- Hsiang, S., Allen, D., Annan-Phan, S., Bell, K., Bolliger, I., Chong, T., … Wu, T. (2020). The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature, 584(7820), 262–267. https://doi.org/10.1038/s41586-020-2404-8
- Huynh, T. L. D. (2020a). The COVID-19 containment in Vietnam: What are we doing? Journal of Global Health, 10(1), 010338. https://doi.org/10.7189/jogh.10.010338.
- Huynh, T. L. D. (2020b). Does culture matter social distancing under the COVID-19 pandemic? Safety Science, 130, 104872. https://doi.org/10.1016/j.ssci.2020.104872
- Jin, H., Lu, L., Liu, J., & Cui, M. (2021). COVID-19 emergencies in East Asian countries: Experiences and challenges. Asia Pacific Journal of Public Health, 33(4), 461–462. https://doi.org/10.1177/10105395211001658
- Karim, S. S. A., & Karim, Q. A. (2021). Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. The Lancet, 398(10317), 2126–2128. https://doi.org/10.1016/S0140-6736(21)02758-6
- Karnon, J. (2020). A simple decision analysis of a mandatory lockdown response to the COVID-19 pandemic. Applied Health Economics and Health Policy, 18(3), 329–331. https://doi.org/10.1007/s40258-020-00581-w
- Lai, S., Ruktanonchai, N. W., Zhou, L., et al. (2020). Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature, 585(7825), 410–413. https://doi.org/10.1038/s41586-020-2293-x
- Long, J. A., Malekzadeh, M., Klar, B., & Martin, G. (2021). Do regionally targeted lockdowns alter movement to non-lockdown regions? Evidence from Ontario, Canada. Health & Place, 102668. https://doi.org/10.1016/j.healthplace.2021.102668
- Mallapaty, S. (2022). China's zero-COVID strategy: What happens next? Nature, 602, 15–16. https://doi.org/10.1038/d41586-022-00191-7
- McCann, P., Ortega-Argilés, R., & Yuan, P. Y. (2021). Rebalancing UK regional and industrial policy post-Brexit and post-COVID-19: Lessons learned and priorities for the future. Regional Studies, 1–13. https://doi.org/10.1080/00343404.2021.1922663
- Mendolia, S., Stavrunova, O., & Yerokhin, O. (2021). Determinants of the community mobility during the COVID-19 epidemic: The role of government regulations and information. Journal of Economic Behavior & Organization, 184, 199–231. https://doi.org/10.1016/j.jebo.2021.01.023
- Michie, J. (2020). The COVID-19 crisis – And the future of the economy and economics. International Review of Applied Economics, 34(3), 301–303. https://doi.org/10.1080/02692171.2020.1756040
- New Straits Times. (2021). Southern provinces in Vietnam tightening Covid-19 restrictions again. New Straits Times. https://www.nst.com.my/world/region/2021/11/747880/southern-provinces-vietnam-tightening-covid-19-restrictions-again
- Nguyen, B., Mickiewicz, T., & Du, J. (2018). Local governance and business performance in Vietnam: The transaction costs’ perspective. Regional Studies, 52(4), 542–557. https://doi.org/10.1080/00343404.2017.1341625
- Nguyen, T. V., Dai Tran, Q., Phan, L. T., Vu, L. N., Truong, D. T. T., Truong, H. C., Le, T. N., Vien, L. D. K., Nguyen, T. V., Luong, Q. C., & Pham, Q. D. (2021). In the interest of public safety: Rapid response to the COVID-19 epidemic in Vietnam. BMJ Global Health, 6(1), e004100. https://doi.org/10.1136/bmjgh-2020-004100
- Onishi, T. (n.d.). Vietnam eases reentry curbs in move to live with COVID-19. Nikki Asia. https://asia.nikkei.com/Spotlight/Coronavirus/Vietnam-eases-reentry-curbs-in-move-to-live-with-COVID-19
- Paddock, C. R., & Doan, C. (2021). Spared for months, Vietnam faces a wave of new infections. New York Times. https://www.nytimes.com/2021/06/02/world/asia/vietnam-covid-ho-chi-minh.html
- Palomino, J. C., Rodríguez, J. G., & Sebastian, R. (2022). The COVID-19 shock on the labour market: Poverty and inequality effects across Spanish regions. Regional Studies, 1–15. https://doi.org/10.1080/00343404.2022.2110227
- Plümper, T., & Neumayer, E. (2021). Fueling the COVID-19 pandemic: Summer school holidays and incidence rates in German districts. Journal of Public Health, 43(3), e415–e422. https://doi.org/10.1093/pubmed/fdab080
- Reed, J., & Pham, H. C. (2021). Vietnam abandons zero-Covid strategy after record drop in GDP. Financial Times. https://www.ft.com/content/37f7f400-20aa-4e52-8f3b-f9359fa73fe8
- Rodríguez-Pose, A., & Burlina, C. (2021). Institutions and the uneven geography of the first wave of the COVID-19 pandemic. Journal of Regional Science, 61(4), 728–752. https://doi.org/10.1111/jors.12541
- Silver, A. (2021). COVID-19: Why China is sticking to ‘zero tolerance’ public health measures. BMJ, 375, n2756. http://dx.doi.org/10.1136/bmj.n2756
- Stevenson, B., & Justin, W. (2006). Bargaining in the shadow of the Law: Divorce laws and family distress’. The Quarterly Journal of Economics, 121(1), 267–288. https://www.jstor.org/stable/25098790
- Tian, K., Zhang, Z., Zhu, L., Yang, C., He, J., & Li, S. (2022). Economic exposure to regional value chain disruptions: Evidence from Wuhan’s lockdown in China. Regional Studies, 1–12. https://doi.org/10.1080/00343404.2022.2078802
- Ullah, A. (2020). Do lockdown and testing help in curbing COVID-19 transmission? Covid Economics: Vetted and Real-Time Papers, Issue 13 (4 May).
- Van Nguyen, P., Huynh, T. L., Ngo, V. M., & Nguyen, H. H. (2021). The race against time to save human lives during the COVID-19 With vaccines: Global evidence. Evaluation Review, 709–724. https://doi.org/10.1177/0193841X221085352
- Wang, D., Hu, B., Hu, C., Zhu, F., Liu, X., Zhang, J., & Zhao, Y. (2020). Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. Journal of the American Medical Association, 323(11), 1061–1069. https://doi.org/10.1001/jama.2020.1585
- Weber, B. S., & Huynh, T. L. D. (2022). COVID-19 challenges and firm responses: Analysis of a city-wide census in a developing country. Managerial and Decision Economics, 43(6), 2184–2195. https://doi.org/10.1002/mde.3517
- Yuan, S. (2022). Zero COVID in China: What next? The Lancet, 399(10338), 1856–1857. https://doi.org/10.1016/S0140-6736(22)00873-X