

Abstract
Objective
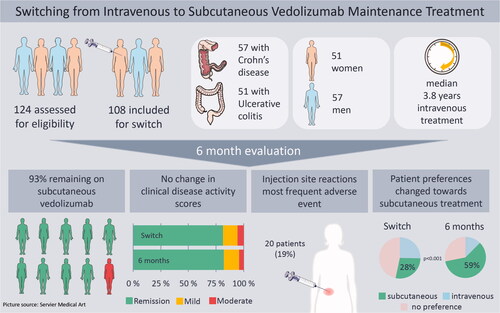
Vedolizumab (VDZ) for subcutaneous (SC) administration has recently become available. We aimed to assess feasibility, safety and clinical outcome when switching from intravenous (IV) to SC VDZ maintenance treatment in a real world cohort of patients with inflammatory bowel disease (IBD) followed by therapeutic drug monitoring (TDM).
Methods
Eligible IBD patients were switched from IV to SC treatment and assessed six months prior to switch, at baseline and six, twelve and twenty-six weeks after switch. Primary outcome was proportion of patients on SC treatment after 26 weeks. Secondary outcomes included adverse events (AEs), clinical disease activity, biochemical markers, treatment interval, serum-VDZ (s-VDZ), preferred route of administration and health-related quality of life.
Results
In total, 108 patients were switched. After 26 weeks, 100 patients (92.6%) were still on SC treatment and median s-VDZ was 47.6 mg/L (IQR 41.3 − 54.6). The most frequent AE was injection site reaction (ISR), reported by 20 patients (18.5%). There were no clinically significant changes in disease activity, biochemical markers and quality of life. The proportion of patients preferring SC administration increased from 28.0% before switch to 59.4% after 26 weeks (p < 0.001).
Conclusions
Nine out of ten patients still received SC treatment after 26 weeks. No change in disease activity occurred, and levels of serum VDZ increased. Although almost one fifth of patients experienced ISRs, a higher proportion favored SC administration at 26 weeks. This study demonstrates that SC maintenance treatment is a safe and feasible alternative to IV treatment.
Graphical abstract
Acknowledgments
The authors thank Maren Sjåmo for contributing to data collection.
Ethical approval
The study was approved by the local data protection officer (PVO 21/00119), based on a written broad informed consent given by the participants. Except for the questionnaires, only data from standard clinical follow-up were included in the study database.
Author contribution
THW was involved in study design, statistical analysis, data interpretation, drafting and revising the manuscript. AWM, MLH and BM were involved in study design, data interpretation, drafting and revising the manuscript. DJW and NB were involved in data interpretation and revising the manuscript. MCS was involved in study design, statistical analysis, data interpretation and revising the manuscript. All authors approved the final document.
Disclosure statement
THW and KA report consultant fees from Takeda outside the submitted work. AWM reports unrestricted research grant from Takeda, NB, DJW and MCS report no conflicts of interest. BM reports consultant fees from Takeda, Janssen, AbbVie, Pfizer; advisory board Takeda, Janssen, AbbVie, Pfizer, Sandoz, Pharma Cosmos; speaker fees from Takeda, Janssen, AbbVie, Sandoz, Orion Pharma. MLH reports speaker fees, consultant fees and serving as an advisory member for or receiving research funding from MSD, AbbVie, Pfizer, Takeda, Janssen, Gilead/Galapagos, Ferring and Tillots Pharma.
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.