
ABSTRACT
Objectives: Running is increasingly popular, but also carries a high injury risk, especially in novice runners. This study investigates differences in incidence and characteristics of running-related injuries (RRIs) between novice and experienced runners in the open population, in order to adapt to more specific needs for future prevention programs.
Methods: Data were obtained from Injuries and Physical Activity in the Netherlands (IPAN), a Dutch questionnaire on injuries, physical activity, and sports. A representative sample of runners (n = 4621) from IPAN, including 1405 novice runners, was used to assess injury incidence rates, anatomical site, onset and need for medical attention of RRIs. Participants who started running during the past 12 months were defined as ‘novice’ runners. ‘Experienced’ runners are participants who had been running for more than 1 year.
Results: Of the 4621 runners, 41,8% were female. The average age was 34.2 years. From 2010 to 2013, a total of 416 injuries were reported. The incidence of RRIs was significantly higher in novice runners compared with experienced runners: 8.78 (8.59–8.96) vs. 4.24 (4.11–4.37) per 1000 h running. In both novice and experienced runners, most RRIs were located at the knee (30.5%) and lower leg (17.8%), with the Achilles’ tendon less frequently injured in novice runners (2.3% vs. 8.4%, p = 0.031). Novice runners sustained more medical attention injuries (36.8%) than experienced runners (29.2%) (p > 0.132).
Conclusions: In total, over 30% of all (novice and experienced) runners, suffered from RRI within 1 year. Novice runners reported more injuries per 1000 h of running in comparison to experienced runners. A tendency toward receiving medical attention more frequently was found in novice runners compared to experienced runners. In view of this higher injury incidence of RRIs and healthcare consumption in novice runners, more studies are needed to develop effective injury prevention programs for novice runners.
1 Introduction
Regular physical activity has a positive influence on many physical and mental outcomes, including aerobic capacity, bodyweight, blood pressure, depressive symptoms and all-cause mortality [Citation1–Citation3]. Running has become a very popular way to exercise by people of all ages and backgrounds, mainly because of low costs and easy accessibility. In view of the increasing number of running events in the Netherlands [Citation4–Citation6], it seems that the number of runners is also increasing, although precise data are lacking.
On the other hand, running also carries a high risk of injury. Commonly, running-related injury (RRI) incidences are expressed as (1) incidence of RRI expressed as a proportion of injured runners per year, or as (2) incidence of RRI per 1000 h of sports participation (running). The annual incidence of RRI ranged from 20–79% and the incidence of RRI per 1000 h of running ranged from 3–59 injuries per 1000 h of running [Citation7–Citation10]. The variance in incidence rates is mainly attributed to differences in RRI definitions and in study populations [Citation10]. Nevertheless, the injury incidence rate seems to be particularly high in novice runners [Citation4,Citation5,Citation8,Citation11].
In view of the forces to which the body is exposed during running, it is not surprising that almost all RRIs affect the lower limb. The knee is most affected, followed by the lower leg and foot [Citation10]. The majority of these injuries are caused by overuse or overtraining. Following extensive study on the cause of injury, the main risk factors are reported to be: a previous RRI [Citation10,Citation12–Citation14], lack of running experience [Citation8,Citation10,Citation13] and an excessive running distance or frequency [Citation10,Citation13,Citation15].
Because an RRI is the main reason to quit running, effective prevention programs are needed to reduce these injuries [Citation16]. Injuries lasting for a longer period often lead to decreased motivation to restart running and to maintain a physically active lifestyle [Citation17]. In the Netherlands, various programs have been developed to assist novice runners. For example, a graded 13-week training program based on the 10% rule (i.e. training load is increased with 10% per week), instead of a normal 8-week training program, was introduced [Citation4]. In another study, a 4-week preconditioning program with walking and hopping exercises prior to the regular running schedule was presented [Citation5]. Unfortunately, neither of these programs was able to reduce RRIs among novice runners substantially.
Identification and description of the extent of the sports injury problem is a first essential step before new, tailor made prevention programs can be developed [Citation18,Citation19]. A possible explanation for the lack of effectiveness of existing programs might be that they are not fully tailored to the specific target group. Although there is evidence that injury incidence and characteristics differ between novice and experienced runners [Citation4,Citation5,Citation8,Citation11], studies directly comparing these two groups are lacking. Therefore, the aim of the present study was to investigate the number of novice and experienced runners and the incidence of RRIs in these runners during a 4-year study period. Furthermore, the anatomical site, onset and need for medical attention of these injuries in both novice and experienced runners were studied.
2 Methods
To provide insight in the number of runners in the Netherlands and differences in incidence and characteristics of RRIs between novice and experienced runners, data were collected from a large population-based study, ‘Injuries and Physical Activity in the Netherlands’ (IPAN).
2.1 Injuries and physical activity in the Netherlands
IPAN is a national continuous questionnaire on accidents, injuries, sports participation, and physical activity, operated by the Dutch Consumer Safety Institute (VeiligheidNL). All respondents of IPAN are participants of InterviewBase, a database of around 238,000 people in the Netherlands willing to contribute to research. New respondents for this database are continuously recruited on the internet or by random digit dialing. Each year a representative sample of about 11,000 members are questioned for IPAN, either by telephone or online. To optimize the representativeness, socio-demographic quotas for this sample are established in advance. During the 4-year study period (2010–2013) 44,729 respondents were questioned for IPAN. To correct for differences in nonresponse within the quota groups, the data is standardized with the Dutch population by weighing the questionnaire data for age, gender, level of education, employment, urbanity, living region, and household size based on data from the Dutch Central Bureau of Statistics (CBS), using random iterative method weighting [Citation20]. Since IPAN is an existing database, data are registered anonymously and respondents cannot be traced with this data, no Ethics Committee approval was acquired.
2.2 Study participants
For the present study, data were used from the general and sports sections of IPAN. Athletes aged ≥15 years who indicated that running was (one of) their sport(s) during the past year were included in this study. Included participants who started running during the past 12 months were defined as ‘novice’ runners. ‘Experienced’ runners were defined as participants who had been running for more than 1 year. Running exposure was calculated as a product of frequency and duration. Running duration and frequency included both training and competitive events and was calculated by multiplying the reported average weekly running exposure (hours) and the number of weeks per year a participant was running.
2.3 Assessment of RRI
The main outcome measure was a new RRI. We estimated the annual number of new RRIs based on a 3-month recall period. Before an RRI was included in our study, one of the researchers (EK) checked that it was in agreement with the (general) sports injury definition by Schmikli et al.: ‘Physical damage of a musculoskeletal nature as a result of a sudden event during a sports activity or as a result of a gradual process related to sports activity’ [Citation21]. An RRI was defined as a sports injury (in accordance with abovementioned definition) caused by running as an independent sport, i.e. not caused by running during other sports such as soccer or field hockey. A maximum number of two new sports injuries in the past 3 months could be reported by participants.
The onset and location of injury were assessed by answers given to the questions ‘Did the injury start with an acute or a gradual onset?’ and ‘Which part of your body was affected by the injury?’. The second question had the following response options: ‘Head, neck, arm (including shoulder, clavicle); trunk (including back); leg (including hip); or whole body’. Depending on this answer, the location was further specified. For example, in case the leg was affected, the participant was asked to indicate the specific location of the leg, including: hip, upper leg, knee, lower leg (including calf and shin), Achilles tendon, ankle, foot/heel, toes, whole leg, or other.
A medical attention injury was defined as an RRI for which a health care professional (general practitioner, physical therapist, medical specialist, sports medicine physician, dentist) was consulted for diagnosis and/or treatment.
2.4 Statistical analysis
Descriptive statistics were used to describe characteristics of runners and injuries. The number of runners and RRI for the period 2010–2013 were calculated for each year separately. The injury incidence rate was expressed as the number of injuries per 1000 h of running. Annual percentage of running injuries with gradual onset and medical attention were calculated. The most affected anatomical sites of injury are presented for the entire study period. All analyses were performed for the entire group of runners together, as well as for experienced and novice runners separately. In addition, incidence rates were calculated for female and male runners separately. These characteristics of runners and injuries were compared between novice and experienced runners by using the independent t-test and Mann-Whitney test, for normally and non-normally distributed continues variables, respectively. Chi-square tests were used to compare categorical variables. To determine linear trends over the years linear regression was applied.
Data analysis was performed using the Statistical Package for the Social Sciences (IBM SPSS, version 23.0), with significance level set at p < 0.05.
3 Results
3.1 Baseline characteristics
During the 4-year study period (2010–2013), data were collected on 4621 runners, of which 1405 were novice runners (30.4%). These novice runners consisted of more female runners, were significantly younger, more often had an intermediate level of education, and less often a high level of education (). The proportion of female runners increased slightly over time in both the novice (from 56.1% to 62.1%) and the experienced runners (from 32.0% to 36.7%). Also the mean age increased in both groups (from 30.0 to 31.3 years in the novice runners and from 34.1 to 36.3 in the experienced runners. For 14.5% of the participants, running was the only sport they practiced, 21.4% of the participants were active in two sports, and 61.3% were active in three or more sports. Novice runners practiced more often only one sport (running) or two sports, compared to experienced runners. Furthermore, the novice runners spent less time on running per year in hours and weeks (median of 14.6 h and 20 weeks) compared to the experienced runners (median of 25 h and 36 weeks).
Table 1. Baseline characteristics of novice and experienced runners, shown as 4-year averages over 2010–2013.
3.2 Number of runners in the Netherlands
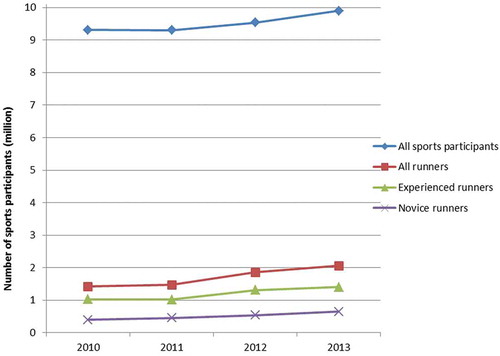
Weighted data showed that in 2010, about 9,310,000 people participated in sports in the Netherlands, in 2013 the number of sports participants had increased to 9,890,000 persons. In 2010, about 1,420,000 people (15.3% of all sports participants) participated in running in the Netherlands (total population in 2010: 16.6 million [Citation22]). During the subsequent 4 years, a significant increase was seen to almost 2 million runners in 2013 (p = 0.039; ). A similar increase was seen for novice runners (from 390,000 to 620,000) and for experienced runners (from 1,030,000 to 1,370,000); although significant only for the novice runners (p = 0.004 and p = 0.077, respectively). For comparison reasons, the number of total sports participants in the Netherlands is also shown in .
Figure 1. Numbers of total sports participants and runners in the Netherlands, 2010–2013.
3.3 Running-related injuries (RRIs)
In our study, 404 runners reported 416 RRIs within the 3-months recall period, of which 279 RRIs were reported by 271 experienced runners and 137 RRIs by 134 novice runners.
Weighted data showed that the absolute number of new RRIs in all runners almost doubled from 350,000 in 2010 to 640,000 in 2013. RRIs sustained by novice runners increased from 120,000 RRIs in 2010 to 210,000 RRIs in 2013. Four-year average injury incidence rate in all runners was 5.11 (95% Confidence Interval (CI): 4.97–5.25) injuries per 1000 h running. The injury incidence was significantly higher for novice runners compared to experienced runners for all years (). Four-year average injury incidence was 8.78 (95%CI: 8.59–8.96) vs. 4.24 (95%CI: 4.11–4.37) per 1000 h running for novice runners and experienced runners, respectively. For comparison purposes, injury incidence for all sports participants (i.e. all athletes including runners) in the Netherlands is also presented.
Table 2. Sports injury incidence in novice (n = 1405) and experienced runners (n = 3215), compared with all sports participants, 2010–2013.
From 2010 to 2013 there was a rise in injury incidence in all runners from 4.54 to 5.35 per 1000 h running (). Among the experienced runners the injury incidence rate followed the same trend, rising from 3.51 to 4.55 per 1000 h running. The injury incidence in novice runners decreased from 8.93 to 8.48 per 1000 h. Trend analysis of injury incidence rates from 2010–2013 for all runners, and the experienced runners and novice runners separately, showed that none of the changes overtime were significant (p = 0.088, p = 0.083, and p = 0.435, respectively).
Because the number of women was higher in the group of novice than in the group of the experienced runners, additional analysis was performed to compare injury rates in men and women separately. Women reported more RRIs than men in all years, Over the 2010–2013 year period, the incidence rate for women was 5.97 injuries per 1000 h of running compared to 4.68 injuries per 1000 h of running for men.
3.4 Location of injury
For all groups, the knee was the most commonly injured site: 30.7% in all runners together, 30.5% in experienced runners, and 31.1% in novice runners (). Examining the injuries incurred by experienced and novice runners showed a significant difference for injuries at the Achilles tendon (8.4% and 2.3%, respectively; p = 0.031), although too few of these injuries had occurred (n < 25) for reliable analysis. The higher percentage of hip injuries in novice runners compared to experienced runners (9.8% vs. 4.6%, respectively) approached statistical significance (p = 0.056), but again underlying number of injuries was too small for reliable analysis.
Table 3. Location of RRIs in novice and experienced runners, shown as 4-year averages over 2010–2013.
3.5 Onset of injury
The majority of RRIs had a gradual onset (). Four-year average values indicated that in the total group of runners 54.6% of RRIs started with a gradual onset. No significant differences between novice and experienced runners were seen for the yearly percentages, neither for the 4-year average percentage. A slight, nonsignificant increase overtime was seen in the injuries with gradual onset in all runners: from 52.9% in 2010 to 60.5% in 2013 (p = 0.526). The trends overtime for novice and experienced runners calculated separately were not statistically significant either (p = 0.142 and p = 0.994).
Table 4. RRIs with gradual onset and medical attention RRIs in novice and experienced runners, 2010–2013a.
3.6 Medical attention injuries
During the period of 2010–2013, 31.6% of all RRIs received medical attention (); most often provided by a physiotherapist (21%), general practitioner (10%) or medical specialist (4%). Compared to the experienced runners, novice runners had a higher percentage of medical attention RRIs for 2011, 2012 and 2013; however, this difference was significant only in 2011 (p = 0.043).
For all three groups an increase overtime in percentage of medical attention injuries was seen. However, none of these time trends were statistically significant (p = 0.092, p = 0.214 and p = 0.562, for all runners, novice and experienced runners, respectively).
4 Discussion
This study based on data from 4621 runners showed an association between running experience and incidence of RRIs: novice runners had, on average, a more than twofold higher injury incidence rate than experienced runners: 8.78 compared to 4.24 per 1000 h running. The Achilles’ tendon was less frequently injured in novice runners than in experienced runners. No significant differences were found in onset of RRI (acute or gradual) between the two groups. Although not significant, a trend was seen in the percentage of medical attention injuries: novice runners had a 1.3 times higher percentage of medical attention injuries than experienced runners. Furthermore, runners in general (i.e. novice and experienced) had a 2.5 times higher injury incidence rate compared to all sports participants (5.11 vs. 1.97 per 1000 sport hours). This confirms that running is a high-risk sport for (overuse) injuries.
In this study, we calculated the number of RRI per 1000 h or running. The incidence of RRI can also be expressed as a proportion of injured runners per year of person-time. Although both injury incidence rates could be calculated based on our data and are commonly used, we prefer to take the exposure of running into account because it better indicates who is at risk by practice running. Based on our data, the annual incidence of RRIs would be 33.9% (210,000/620,000) for novice runners and 31.4% (430,000/1,370,000) for experienced runners, with a relative risk of 1.08 for novice compared to experienced runners. Based on these annual RRI incidences, it could be concluded that novice runners are not extremely more at risk for RRIs compared to experienced runners. However, according to our calculated incidences per 1000 h of running, novice runners do have a twofold higher injury incidence rate compared to experienced runners (8.78 (95%CI: 8.59–8.96) vs. 4.24 (95%CI: 4.11–4.37). These calculations do not only show that it is important to take exposure time into account when studying incidence of RRIs, but it also shows that different conclusions can be drawn depending on how these rates are calculated. We therefore recommend including exposure time when calculating incidence rates. Furthermore, attention is needed in case of interpretation of annual incidence rates.
As far as we know this is one of the first studies to directly compare novice and experienced runners with regard to incidence and characteristics of RRIs. Until now, studies that included both novice and experienced runners lacked a direct comparison between these groups. For instance, Linton and Valentin (2018) investigated the incidence and type of RRI in novice and recreational UK runners, and identified factors associated with injury [Citation11]. Running experience of over 2 years was protective for RRI in their study (OR 0.578–0.65) [Citation11], but further comparisons between novice and experienced runners were not performed. Van Middelkoop et al. (2008) included both novice and experienced runners preparing for a marathon, but reported data only for the entire population pooled together [Citation7]. The injury incidences from their study are somewhat lower compared with ours (3.2 vs. 5.1 per 1000 h of running). Other studies, such as the GRONORUN trials and the NLstart2run study, included only novice runners and reported much higher injury incidences for this group compared with our data (28–38 vs. 8.8 per 1000 h of running) [Citation4–Citation6].
There are some explanations for the differences in injury incidence. First, differences in RRI definitions can lead to both higher and lower estimations of incidence [Citation23]. In the studies mentioned above [Citation4–Citation7] the definition included restrictions of running frequency, distance, speed, or duration, whereas the definition used in our study did not explicitly mention such restrictions. To improve inter-study comparability, a consensus-based definition was introduced by Fuller et al. [Citation24]. Although not literally the same, this latter definition and the one used in our study have the same essential features. Fuller et al. defined an injury as any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities [Citation24]. The definition we used was: ‘an RRI is a physical damage of a musculoskeletal nature as a result of a sudden event during running or as a result of a gradual process related to running’ [Citation21]. Second, the fact that the novice runners in the GRONORUN trials were training for a 4-mile race and those in the NLstart2Run were training to run 20 min nonstop might partly explain the higher injury rate compared to our study, because in a relatively short period of time (8–13 and 6 weeks, respectively) training load had to be increased [Citation4–Citation6]. Third, different data collection methods and follow-up lengths are likely to influence injury incidence rates [Citation25] For example, a study by Schmikli et al [Citation21]. also based on IPAN, reported data from 2000–2005 for novice and experienced runners together and found an RRI incidence rate of 1.6 per 1000 h of running. After 2006, method of contacting participants of IPAN changed from only by telephone to both by telephone and online. This shift resulted in a higher number of reported injuries, and might (partly) explain the higher injury incidence found in our study.
In the present study, the knee was most frequently injured, which is in line with other reports [Citation5,Citation9,Citation15]. Although significantly more injuries were found in the Achilles tendon for experienced runners than for novice runners, this result should be interpreted with caution due to the small number of these injuries. Furthermore, our study showed that a majority of RRIs in all runners started with a gradual onset. Although not synonymous, this may indicate that most RRIs are overuse injuries. This is supported by studies reporting that RRIs consist for up to 80% of overuse injuries, such as iliotibial band syndrome, patellofemoral pain syndrome and medial tibial stress syndrome [Citation15,Citation26,Citation27]. In this study, about one-third of the RRIs needed medical attention. For 3 out of 4 study years, novice runners had a higher percentage of medical attention injuries than experienced runners (albeit only significant for 2011). Remarkably, in 2011 this percentage was more than two times as high, in contrast to much smaller differences during the other years; no clear explanation for this could be found.
Some limitations of the present study need to be addressed. First, all information in IPAN is based on self-report. Although this method may not yield the highest quality data, it is a highly practical way to collect information in large cohorts on all injuries, including less severe ones. Most official medical registrations do not include minor injuries for which no medical consultation is necessary. For example, a recent study showed that self-reported incidence rates of ankle injuries were around 5.5 times higher than those based on Emergency Department registration [Citation28]. Secondly, there is a risk of recall bias because we asked participants to answer questions concerning the last 3 months. This recall bias and, therefore, the accuracy of self-reporting of sports injuries depend to a large extent on the length of the recall period [Citation29,Citation30]. A recall period of 1–3 months is recommended for injury questionnaires [Citation31], similar to that used in our study. This study concentrated on injuries caused by running in athletes who indicated themselves as runners. In this way we included all runners, i.e. also those who started running very recently, or those who participate in other sports as well. Novice runners were defined as runners who started to run in the previous 12 months. This specific group of runners might possibly be at highest risk for RRIs [Citation6] and would be left out if a narrower definition of running was used. According to our definition, runners who participate in other sports and/or do not run on a regular basis but started with running >12 months ago, were considered experienced runners. However, they could very likely be still ‘novice’. This is not taken into account in this study. In our study, 14.5% of the runners did not participate in other sports, and the median hours of running per year in our study population is rather low. This might indicate that the runners included in this study most likely consisted of recreational, noncompetitive runners. This should be taken into account when our incidence rates are compared to studies that included competitive runners, although in our opinion, our study gives a valuable insight in the injury incidences of those practicing running as a recreational type of sport. Finally, exposure time was calculated as a product of frequency (weeks) and duration (hours of running per week). Information on running intensity, which can be used to fully describe running exposure, was not available, and therefore not included in this study. To further examine the association between running experience and RRI incidence and correct for confounding factors, prospective cohort studies are needed with more detailed information on running exposure (duration, frequency and intensity (pace)).
Given the injury prevention programs setup for novice runners (e.g. GRONORUN 1 [Citation4] and 2 [Citation5], Start2Run [Citation6]) awareness of the high risk of RRIs in novice runners is, to some extent, present. All these programs focus mainly on the gradual increase of training load. The GRONORUN trials were designed to study the preventive effect of these programs, but found that they were not successful in reducing RRIs. In our opinion, to make progress in this field, future prevention programs should be multifactorial. A systematic review including 25 randomized controlled trials with interventions to prevent RRIs classified interventions in four categories: stretching and conditioning exercises, modification of training schedules, use of orthoses and type of shoes [Citation32]. Only patellofemoral braces and custom-made insoles significantly reduced RRIs. However, conclusions about the effectiveness of interventions were made based on only one or a few studies, and almost all studies included only one intervention. A prevention program using interventions from different categories might achieve better results in reducing RRIs; however, more research is needed to support this hypothesis.
In conclusion, this study compared injury data between novice and experienced runners and found a twofold greater injury incidence rate in novice runners (those who had started running in the previous 12 months). In total, over 30% of runners, whether experienced or novice, reported a RRI within 1 year. Novice runners reported more injuries per 1000 h of running than experienced runners. In both groups, most RRIs had a gradual onset and were located at the knee, lower leg and ankle. In view of the higher injury incidence rate per 1000 h of running and the higher healthcare consumption in novice runners, more studies are needed to develop effective (multifactorial) prevention programs to reduce RRIs in novice runners.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. Peer reviewers on this manuscript have no relevant financial relationships to disclose.
Authors’ contributions
EK: Performed analyses; interpreted the results; writing of the article. DB: interpreted the results; writing of the article. FB: reviewed drafts of manuscript and provided feedback. BH: interpreted the results; reviewed drafts of manuscript and provided feedback. All authors reviewed and approved the final version of the paper.
Acknowledgments
The data used in this study were provided by the Dutch Consumer Safety Institute, Amsterdam, the Netherlands.
Additional information
Funding
References
- Shaw KA, Gennat HC, O’Rourke P, et al. Exercise for overweight or obesity. Cochrane Database Syst Rev. 2006;Issue 4. DOI:10.1002/14651858.CD003817.pub3.
- Ortega FB, Ruiz JR, Castillo MJ, et al. Physical fitness in childhood and adolescence: A powerful marker of health. Int J Obes (Lond). 2008;32(1):1–11.
- Samitz G, Egger M, Zwahlen M. Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. Int J Epidemiol. 2011;40(5):1382–1400.
- Buist I, Bredeweg SW, van Mechelen W, et al. No effect of a graded training program on the number of running-related injuries in novice runners: A randomized controlled trial. Am J Sports Med. 2008;36(1):33–39.
- Bredeweg SW, Zijlstra S, Bessem B, et al. The effectiveness of a preconditioning programme on preventing running-related injuries in novice runners: A randomised controlled trial. Br J Sports Med. 2012;46(12):865–870.
- Kluitenberg B, van Middelkoop M, Smits DW, et al. The NLstart2run study: incidence and risk factors of running-related injuries in novice runners. Scand J Med Sci Sports. 2015;25(5):e515–23.
- van Middelkoop M, Kolkman J, Van Ochten J, et al. Prevalence and incidence of lower extremity injuries in male marathon runners. Scand J Med Sci Sports. 2008;18(2):140–144.
- Buist I, Bredeweg SW, Bessem B, et al. Incidence and risk factors of running-related injuries during preparation for a 4-mile recreational running event. Br J Sports Med. 2010;44(8):598–604.
- Taunton JE, Ryan MB, Clement DB, et al. A prospective study of running injuries: the vancouver sun run “in training” clinics. Br J Sports Med. 2003;37(3):239–244.
- van Gent RN, Siem D, van Middelkoop M, et al. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Br J Sports Med. 2007;41(8):469–480. discussion 480.
- Linton L, Valentin S. Running with injury: A study of UK novice and recreational runners and factors associated with running related injury. J Sci Med Sport. 2018 May 24; pii. S1440-2440(18):30179–8. DOI:10.1016/j.jsams.2018.05.021.
- Buist I, Bredeweg SW, Lemmink KA, et al. Predictors of running-related injuries in novice runners enrolled in a systematic training program: A prospective cohort study. Am J Sports Med. 2010;38(2):273–280.
- Saragiotto BT, Yamato TP, Hespanhol Junior LC, et al. What are the main risk factors for running-related injuries? Sports Med. 2014;44(8):1153–1163.
- Hulme A, Nielsen RO, Timpka T, et al. Risk and protective factors for middle- and long-distance running-related injury. Sports Med. 2017;47(5):869–886. May.
- van Mechelen W. Running injuries. A review of the epidemiological literature. Sports Med. 1992;14(5):320–335.
- Koplan JP, Powell KE, Sikes RK, et al. An epidemiologic study of the benefits and risks of running. JAMA. 1982;248(23):3118–3121.
- Sallis JF, Hovell MF, Hofstetter CR. Predictors of adoption and maintenance of vigorous physical activity in men and women. Prev Med. 1992;21(2):237–251.
- Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9(1–2): 3–9. discussion 10.
- van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992;14(2):82–99.
- Sharot T. Weighting survey results. J Mark Res Soc. 1986;28:269–284.
- Schmikli SL, Backx FJ, Kemler HJ, et al. National survey on sports injuries in the netherlands: target populations for sports injury prevention programs. Clin J Sport Med. 2009;19(2):101–106.
- CBS (Dutch Central Bureau of Statistics). population; key figures. [cited 2014 Sep]. Available from: http://statline.cbs.nl/StatWeb/publication/?DM=SLNL&PA=37296ned&D1=a&D2=0,10,20,30,40,50,60,(l-1),l&HDR=G1&STB=T&VW=T
- Kluitenberg B, van Middelkoop M, Verhagen E, et al. The impact of injury definition on injury surveillance in novice runners. J Sci Med Sport. 2016 Jun;19(6):470–475.
- Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40(3):193–201.
- Knowles SB, Marshall SW, Guskiewicz KM. Issues in estimating risks and rates in sports injury research. J Athl Train. 2006;41(2):207–215.
- Hreljac A. Impact and overuse injuries in runners. Med Sci Sports Exerc. 2004;36(5):845–849.
- Bullock SH, Jones BH, Gilchrist J, et al. Prevention of physical training-related injuries recommendations for the military and other active populations based on expedited systematic reviews. Am J Prev Med. 2010;38(1 Suppl):S156–81.
- Kemler E, van de Port I, Valkenberg H, et al. Ankle injuries in the Netherlands: trends over 10–25 years. Scand J Med Sci Sports. 2015 Jun;25(3):331–337. doi: 10.1111/sms.12248.
- Valuri G, Stevenson M, Finch C, et al. The validity of a four week self-recall of sports injuries. Inj Prev. 2005;11(3):135–137.
- Gabbe BJ, Finch CF, Bennell KL, et al. How valid is a self reported 12 month sports injury history? Br J Sports Med. 2003;37(6):545–547.
- Harel Y, Overpeck MD, Jones DH, et al. The effects of recall on estimating annual nonfatal injury rates for children and adolescents. Am J Public Health. 1994;84(4):599–605.
- Yeung SS, Yeung EW, Gillespie LD. Interventions for preventing lower limb soft-tissue running injuries. Cochrane Database Syst Rev. 2011;(7):CD001256. doi: 10.1002/14651858.CD001256.pub2.