
Abstract
We investigated distinct profiles in emotion regulation strategies (reappraisal and suppression) and their associations with sexual function and mental health. The online survey sample consisted of 5436 adult participants. The gender stratified cluster analysis resulted in a four-cluster solution for both men and women. Better sexual function and mental health scores were found for participants with high cognitive reappraisal and low expressive suppression. High expressive suppression was associated with higher anxiety and depression and worse sexual function. Sexological care should take into account the assessment of emotion regulation abilities and emotion regulation training interventions to support reappraisal strategies.
Introduction
According to the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders-5-TR (American Psychiatric Association, Citation2013), sexual disorders are characterized by difficulties in the ability to respond sexually or to obtain sexual pleasure. From a functional perspective, sexual health refers to the ability to experience the full sexual response cycle (Girardi et al., Citation2015). Mental health refers to the state of mental well-being which make individuals capable of managing their life stressors and accomplish their potential (World Health Organization, Citation2023)
Epidemiological studies on sexual disorders in the general population report prevalence rates varying from 20-30% for adult men and 40-45% for adult women, fulfilling the criteria for at least one sexual dysfunction during their lifetime (Lewis et al., Citation2010).
The etiology of sexual disorders is multifactorial, encompassing physiological, affective, interpersonal, and psychological, context-dependent-factors (Willi & Burri, Citation2015), which predispose, precipitate, or maintain sexual dysfunction (Hawton & Catalan, Citation1986). Psychological factors include performance anxiety, attitudes toward sex, self-reported levels of stress and fatigue, and anxiety (McCabe, Citation2005), and they may either contribute to the development of sexual problems or be a consequence thereof (Leiblum & Rosen, Citation2000).
Emotional reactions and thoughts during sexual activity can also affect sexual functionality. With respect to emotions, studies have reported different patterns for individuals with and without sexual dysfunction. For instance, among healthy women and men, anxiety had no effect or even increased sexual arousal (Barlow, Sakheim, & Beck, Citation1983; Laan, Everaerd, Van Aanhold, & Rebel, Citation1993), whereas in women and men with sexual difficulties these factors rather decrease sexual responses (Beck, Barlow, Sakheim, & Abrahamson, Citation1987; Dèttore, Pucciarelli, & Santarnecchi, Citation2013). In a similar vein, sexually dysfunctional men reported significantly more sadness, disillusion, and fear, and less pleasure and satisfaction when compared to men without sexual problems. Similarly, women with sexual dysfunction showed less pleasure and satisfaction, and more sadness, disillusion, guilt, and anger (Nobre & Pinto-Gouveia, Citation2006).
These results suggest that emotion regulation (ER) may be important for sexual health and most likely also in the treatment of sexual problems. ER refers to the process of modulating an emotional response, which includes whether and how an emotion is experienced or expressed (Gross, Citation1998). Functionally, efficient ER involves: (1) awareness and understanding of emotions (clarity); (2) acceptance of emotions; (3) the ability to control impulsive behaviors and to behave in accordance with desired goals when experiencing both negative and positive emotions; and (4) the ability to use situationally appropriate ER strategies to achieve personal goals and meet situational demands (Gratz & Roemer, Citation2004).
Among the different ER strategies, the two most frequently studied are reappraisal and suppression (John & Gross, Citation2004). Reappraisal refers to the modulation of an emotional experience by changing how one perceives an emotionally provoking event or finding benign or positive attributions or interpretations of an event to prevent or reduce negative mood concerning the event (Gross, Citation1998; John & Gross, Citation2004). In contrast, suppression involves the inhibition of one’s emotional reaction to an event (John & Gross, Citation2004). Depending on the context and on the situation, the use of different ER strategies can be considered adaptive or maladaptive (Rogier, Garofalo, & Velotti, Citation2019; Webb, Miles, & Sheeran, Citation2012).
Overall, greater use of reappraisal has been linked with better psychological well-being and more adaptive social functioning whereas greater suppression use has been associated with poorer social functioning and lower relationship quality (Chervonsky & Hunt, Citation2017). Also, the ability to communicate emotions (verbally or as overt behavior) is a crucial component of emotion regulation and of healthy coping (Bloch, Haase, & Levenson, Citation2014).
In this sense, the ability to flexibly regulate emotions can be seen as a therapeutic goal in sexual therapy since it facilitates emotional awareness and experience, problem-solving, acceptance and mindfulness, ultimately, diminishing the sensitivity and reactivity to negative stimuli (Rosen & Bergeron, Citation2019).
Sexual experiences occur in complex relational environments, with relationship processes being involved not only in the generation and experience of sexual emotions, but also in their regulation (Dewitte, Citation2014). In other words, the social-relational context and the dynamic interplay between cognitive, affective, and motivational responses may shape how sexual emotions are generated and regulated (Houck, Barker, Hadley, Menefee, & Brown, Citation2018).
As a result, dysregulation of emotions in sexual contexts most likely constitute a risk factor for developing sexual problems (Janssen, Everaerd, Spiering, & Janssen, Citation2000; Payne, Binik, Amsel, & Khalifé, Citation2005). Reduced ER capacity may lead individuals not to be focused on the present moment of sexual interaction, becoming overwhelmed or distracted by difficult emotions associated with self-criticism, performance anxiety, low self-esteem, or sexual inhibition (Pepping, Cronin, Lyons, & Caldwell, Citation2018; Pepping, O’donovan, Zimmer-gembeck, & Hanisch, Citation2014). For example, alexithymia, (i.e., deficits in the processing of emotions, or more generally, a disturbance in the regulation of emotions) has been associated with Hypoactive Sexual Desire Disorder both in men and women (Taylor, Michael Bagby, & Parker, Citation1991), and with Erectile Disorder (Madioni & Mammana, Citation2001) and Premature Ejaculation (Simonelli, Bonanno, Michetti, & Rossi, Citation2008) in men.
Difficulties in regulating negative emotions may represent a key mechanism hampering the well-being of couples (Rosen & Bergeron, Citation2019). According to the interpersonal emotion regulation model of women’s sexual dysfunction, a lack of emotional awareness, expression, and experience could lead to increased sensitivity and reactivity to negative stimuli (e.g., pain) and promote the use of less adaptive ER strategies (avoidance, suppression, catastrophizing, emotional outbursts), rather than adaptive ones (reappraisal, approach, problem-solving, appropriate disclosure, acceptance, mindfulness) (Rosen & Bergeron, Citation2019). Although not developed to include male sexual dysfunction, it is plausible that this model also is applicable for men. For example, a study investigating couples affected by Female Sexual Interest/Arousal Disorder found that respondents reporting difficulties regulating negative emotion and greater use of emotional suppression showed higher depression and anxiety, and lower relationship satisfaction (Dubé, Corsini-Munt, Muise, & Rosen, Citation2019)
We recently conducted a scoping review aiming at identifying the state of the art of the relationship between ER and sexual health (Fischer, Andersson, Billieux, & Vögele, Citation2022). One of the main findings concerned the result that overall poor ER was associated with poor sexual health and diminished satisfaction. We concluded that ER interventions may be beneficial in the treatment of sexual difficulties. Notwithstanding these results, we also inferred from this review that little attention has been devoted in previous research to the investigation of the role of ER strategies and their relationships with sexual health.
The present study was designed to explore the role of ER strategies (cognitive reappraisal and expressive suppression) for sexual function and mental health using a data-driven cluster analytical approach to identify participants with different profiles of ER strategies in relation to their sexual function and mental health. Results from such studies may fill the current literature gap regarding ER strategies use and its relationship to sexual function as well as inform targeted interventions addressing the needs of patients according to their ER profiles.
We hypothesized that (1) higher use of cognitive reappraisal would be grouped with better sexual function and mental health scores both in men and women while (2) higher use of expressive suppression would be grouped with worse sexual function and mental health scores both in men and women.
Method
Participants
Participants were aged between 18 and 77 years (M = 25.80, SD = 6.96). A majority self-identified as female (82.49%, n = 4484), French speakers (40.29%, n = 2190), students (67.95%, n = 3694), with a post-secondary/university grade (73.99%, n = 4022) and as heterosexual (79.73%, n = 4334), see . Among the initial 5504 participants 68 respondents were discarded because they did not meet the inclusion criteria or had missing values. The final sample consisted of 5436 participants.
Table 1. Participants sociodemographic characteristics (N = 5436).
Procedure
A cross-sectional online survey was conducted using the SoSci Survey platform addressing sexual function, mental health, and the use of ER strategies. The survey was available in English, French, German, Spanish, and Portuguese. All questionnaires used had previously been validated except for the PHQ-9 and GAD-7 French versions (Pfizer, https://www.phqscreeners.com/), which were translated but without published validation. Recruitment and advertisement took place mainly via social media platforms, such as Facebook and Instagram. Before taking part in the survey and electronically signing the consent form, participants were informed about the content and the purpose of the study, the guarantee of anonymity, their right to withdraw from the study at any moment without any explanation, and about the possibility to contact the research team for questions or concerns. No monetary incentive was offered to participants.
Participants were eligible to take part in the survey if they met the following inclusion criteria: a) 18 years of age or older, b) fluent in one of the languages in which the questionnaires were available (English, German, French, Spanish or Portuguese).
Data collection took place between January 2019 and October 2019, with a total response rate of 56% (44% gave consent and started completing the survey but did not finish it). The time taken to complete the survey was on average 10 min. Ethical approval was obtained from the University of Luxembourg Ethics Review Panel (ERP 18-075).
Measures
Patient-health questionnaire (PHQ-9) (Kroenke, Spitzer, & Williams, Citation2001)
The PHQ-9 is a 9-item Likert scale instrument (responses ranging from 0 = not at all to 3 = nearly every day), which rates the frequency of symptoms over the past two weeks resulting in a severity index score (total score 5-9 = mild, 10-14 = moderate, 15-19 = moderately severe, 20-27 = severe). An item example of the scale is: “Over the last 2 wk, how often have you been bothered by any of the following problems? Ex: Little interest or pleasure in doing things.” The instrument has been validated in Spanish (Diez-Quevedo, Rangil, Sanchez-Planell, & Kroenke, Citation2001), German (α = .88; Gräfe, Zipfel, Herzog, & Löwe, Citation2004), Portuguese (α = .86; Monteiro, Torres, Pereira, Albuquerque, & Morgadinho, Citation2013) and is available in French. In our sample there was an across language Cronbach’s alpha of .85.
General anxiety disorder scale (GAD-7) (Spitzer, Kroenke, Williams, & Löwe, Citation2006)
the GAD-7 is a 7-item Likert scale instrument (responses ranging from 0 = not at all to 3 = nearly every day), which investigates anxiety-related symptoms over the past two weeks (total score 5 = mild, 10 = moderate, 15 = severe). An item example of the scale is: “Over the last 2 wk, how often have you been bothered by the following problems? Ex: Feeling nervous, anxious or on edge.” The GAD-7 has been validated in English (α = .92; Mills et al., Citation2014), Spanish (α = .936; Garcia-Campayo et al., Citation2010), German (α = .85; Hinz et al., Citation2017), Portuguese (α = .916; Moreno et al., Citation2016) and is available in French. In our sample there was an across language Cronbach’s alpha of .88.
Emotion regulation questionnaire (ERQ) (Gross & John, Citation2003)
the ERQ is a 10-item Likert scale designed to measure respondents’ tendency to regulate their emotions in two ways: (1) Cognitive Reappraisal (6 items, total scores between six and 42) and (2) Expressive Suppression (4 items, total scores between four and 28). Respondents answer each item on a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). An item example is: “When I want to feel more positive emotion (such as joy or amusement), I change what I’m thinking about.” Higher values on the expressive suppression factor indicate higher use of expressive suppression, and higher values on cognitive reappraisal indicate higher use of this ERS. The original study found a two-factor structure for both subscales in samples of different ages and cultures with adequate internal consistency (α = .73 suppression, α = .79 reappraisal). Validated versions of the ERQ are available in Spanish (suppression α = .75, reappraisal α = .79; Cabello, Salguero, Fernández-Berrocal, & Gross, Citation2013), German (suppression α = .76, reappraisal α = 73; Abler & Kessler, Citation2009), French (suppression α = .78, reappraisal α = .73; D’Argembeau & Van der Linden, Citation2006), and Portuguese (suppression α = .69, reappraisal α = .74; Batistoni, Ordonez, Silva, Nascimento, & Cachioni, Citation2013). In our sample there was an across language Cronbach’s alphas of .85 for reappraisal and of. 77 for suppression.
Sexual function
Sexual function assessment was conducted using the Female Sexual Function Index (FSFI) and the International Index of Erectile Function (IIEF) and directed to the FSFI or the IIEF according to their self-reported biological sex.
Female sexual function index (FSFI) (Rosen, Brown, Heiman, & Leib, Citation2000)
This is a 19-item questionnaire with each item answered on a 5-point Likert scale, developed for assessing domains of sexual functioning (e.g., desire, arousal, lubrication, orgasm, satisfaction, pain) in women. An item example is: “Over the past 4 wk, how often did you feel sexual desire or interest?” Women with a total score ≤ 26.55 were considered sexually dysfunctional (Wiegel, Meston, & Rosen, Citation2005). The questionnaire has been validated in German (Berner, Kriston, Zahradnik, & Härter, Citation2004), French (all alpha’s higher than .80; Wylomanski et al., Citation2014), Spanish (all alpha’s higher than .82; Vallejo-Medina, Pérez-Durán, & Saavedra-Roa, Citation2018), and Portuguese (standardized alpha = .96, domains alpha’s ranging from .31 to .97; Pacagnella, Vieira, Rodrigues, & Souza, Citation2008; Thiel et al., Citation2008) as well as for web-administration (Crisp, Fellner, & Pauls, Citation2015). In our sample there was an across language Cronbach’s alpha of .91.
International index of erectile function (IIEF) (Rosen et al., Citation1997)
This is a 15-item, 6-point Likert scale, self-administered questionnaire for assessing sexual functioning in men. It encompasses five different domains of sexual function: erectile function, orgasm function, sexual desire, intercourse satisfaction and overall satisfaction. An item example is: “Over the past 4 wk, how often were you able to get an erection during sexual activity?” The cutoff for Erectile Dysfunction was established, with scores < 25 indicating erectile dysfunction and those with scores ≥ 25 as not having erectile dysfunction. The questionnaire has been validated in German (α = .95; Wiltink, Hauck, Phädayanon, Weidner, & Beutel, Citation2003), French (α = .91; Dargis et al., Citation2013), Spanish (α = .97; Hernández, Thieme, & Araos, Citation2017), and Portuguese (α = .89; Gonzáles et al., Citation2013). In our sample there was an across language Cronbach’s alpha of .90.
Data analyses
The distributions of the questionnaire data were examined using the Kolmogorov-Smirnov test. Depending on the distribution, we computed internal consistency (Cronbach’s alpha) and produced a correlation matrix using Spearman or Pearson correlations to examine the associations between the variables.
Cluster analyses were performed to generate profiles according to the preferred use of ER strategies. For these analyses we combined a hierarchical and nonhierarchical clustering approach, as recommended by Hair, Black, Babin, and Anderson (Citation2010). By using this approach, the strengths of one method compensates for the disadvantage of the other (e.g., sensitivity to outliers). For the clusters’ generation, we used the ER strategies from the ERQ (cognitive reappraisal and expressive suppression). After verifying the presence of collinearity between the clustering variables using the correlation matrix, we proceeded with the following steps: (1) we applied a z-transformation to cluster variables followed by (2) hierarchical clustering, using Ward’s method with squared Euclidian distances. This approach is designed to identify the optimal number of clusters for the nonhierarchical clustering analyses. The best number of clusters was evaluated using the NbClust R package. This package is based on the majority rule and reports the best number of clusters proposed for all the available indices (e.g., Duda, silhouette, Dunn, Friedman, etc.); (3) we proceeded to a nonhierarchical K-means clustering (iter max = 1000, nstart = 50) to create the clusters using the optimal number of clusters identified with the hierarchical clustering; (4) we determined the characteristics of the clusters regarding their ER strategy use profiles; and (5) we compared the identified clusters on Anxiety (GAD-7), Depression (PHQ-9), and Sexual function (FSFI and IIEF).
The analyses were performed using R (v4.0.3) and the following packages: factoextra (kmeans clustering), psych (anova, non param test), nbClust (hierarchical clustering), tidyverse (plot generation), dist (distribution matrix generation).
Results
All scales used showed good Cronbach’s alphas (see ). Due to the non-normal distribution of the variables, we used Kruskal Wallis and Dunn’s test with Bonferroni correction to analyze differences between clusters. shows the Spearman correlation matrix. Correlations between the cluster variable (reappraisal and suppression) did not show multicollinearity (rs = .049). The hierarchical clustering analyses suggested 4 clusters. Among all the indices (n = 23), 7 proposed 4 as the best number of clusters.
Table 2. Cronbach’s alpha for each scale (for each language).
Table 3. Spearman Correlation matrix.
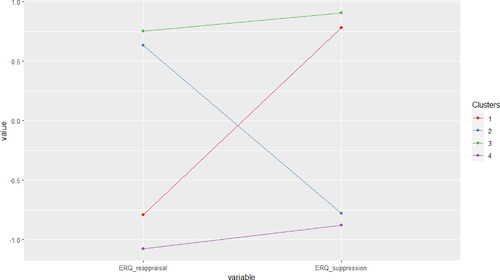
Four ER profiles were created using nonhierarchical K-means clustering (). The identified profiles were characterized by: low reappraisal and high suppression (LR-HS), n = 1243; high reappraisal and low suppression (HR-LS), n = 1695; high reappraisal and high suppression (HR-HS), n = 1425; low reappraisal and low suppression (LR-LS), n = 1073.
Figure 1. Clusters of emotion regulation strategy.
Cluster 1. Z scores: Reappraisal = −0.795; Suppression = 0.783.
Cluster 2. Z scores: Reappraisal = 0.632; Suppression = −0.779.
Cluster 3. Z scores: Reappraisal = 0.755; Suppression = 0.908.
Cluster 4. Z scores: Reappraisal = −1.080; Suppression = −0.882.
Details of the cluster profiles are shown in . All clusters differed with respect to the reappraisal ER strategy (p<.001). Regarding the use of suppression as ER strategy, clusters also differed except for LR-LS and HR-LS who are identical (p = 0.0426), meaning that these 2 groups were similar regarding their suppression scores ().
Table 4. Descriptive statistics by cluster.
Table 5. Groups comparison (Kruskal Wallis rank sum test and Dunn’s pairwise with Bonferroni correction).
Depression and anxiety
The Kruskall Wallis test showed significant differences between the clusters on both depression (χ2(3) = 339.2, p < .001) and anxiety (χ2(3) = 221.91, p < .001) scores.
Depression
Pairwise comparisons using Dunn’s test indicated that all clusters differed with regards to depression scores (PHQ, p <.001), except for clusters HR-HS and LR-LS who were identical. It is important to note that their mean depression scores were close to the overall mean of the dataset.
Anxiety
The clusters differed in anxiety scores (GAD) except for the LR-HS and LR-LS clusters (p = 0.21). It is interesting to note that the LR-LS groups showed significant differences on the HR-HS cluster, where the LR-LS scores were significantly higher on the anxiety scale (GAD). This was not the case for depression for which these two clusters showed no significant differences.
Among all the clusters, individuals in the HR-LS cluster reported the lowest anxiety and the lowest depression scores, while the LR-HS cluster was characterized by a higher level of anxiety and depression. Clusters that were characterized by a high level of suppression tended to show higher anxiety and depression scores.
Sexual function
The Kruskal Wallis test resulted in significant differences between the clusters on sexual function regarding the FSFI (χ2(3) = 116.24, p < .001) and the IIEF (χ2(3) = 18.449, p < .001) scores.
For both IIEF and FSFI scores, there were significant differences between LR-HS and HR-LS, and between HR-LS and HR-HS, where HR-LS showed a higher mean score suggesting better sexual function. In terms of sexual function, individuals in the HR-HS cluster did not differ from those in the LR-HS (IIEF: p = 1; FSFI: p =.0256) or LR-LS clusters (IIEF: p = 1; FSFI: p = 0.2955).
On the IIEF scale participants in the HR-LS cluster did not differ from those in the LR-LS cluster (p = 0.1149). In contrast, FSFI scores differed significantly between those in the HR-LS and the LR-LS cluster (p <.001), with the HR-LS indicating better sexual function. The same was true for the LR-HS and LR-LS clusters who were not significantly different on the IIEF scale (p = 0.5407) but differed on the FSFI (p <.001), with the LR-LS suggesting better sexual function.
Discussion
The present study investigated the role of ER strategies in relation to sexual function and mental health. The cluster analytical approach enabled us to examine self-reported sexual function and mental health in men and women in terms of their ER strategies, namely cognitive reappraisal, and expressive suppression. For both genders, four clusters were observed: low reappraisal and high suppression (LR-HS), high reappraisal and low suppression (HR-LS), high reappraisal and high suppression (HR-HS), low reappraisal and low suppression (LR-LS).
We hypothesized that in both men and women (1) higher use of cognitive reappraisal would be associated with better sexual function and mental health scores and (2) higher use of expressive suppression would be linked with worse sexual function and mental health scores. Both hypotheses were confirmed. Regarding mental health, our data showed to be in accordance with emotion regulation models and previous studies suggesting that poor emotion regulation interferes with adaptive coping, leading to adverse psychological consequences such as anxiety and depression (Aldao, Nolen-Hoeksema, & Schweizer, Citation2010; Ehring, Tuschen-Caffier, Schnülle, Fischer, & Gross, Citation2010; Gross, Citation2002; Vujanovic, Zvolensky, & Bernstein, Citation2008).
Higher scores on suppression were associated with higher anxiety and depression scores. In contrast, higher reappraisal and lower suppression were associated with better mental health (lowest scores in anxiety and depression in the current sample). In addition, participants using neither of these ER strategies had the highest anxiety scores. Difficulties with regulating (negative) emotions (e.g., poor awareness and clarity of the emotion) have been shown to be linked to poorer adjustment in several clinical conditions (e.g., posttraumatic stress disorder, pain disorders) (Doolan, Bryant, Liddell, & Nickerson, Citation2017; Lutz, Gross, & Vargovich, Citation2018).
Regarding sexual function, our hypotheses were also confirmed. Similar to the results on mental health, the cluster of participants with higher reappraisal use had better sexual function scores in both the male and the female questionnaire. Despite the overall positive association of reappraisal with sexual function for both men and women (and the association of suppression with sexual disorders symptomatology), there were some differences. For women, there was a significant difference between the groups with low suppression but with high and low reappraisal use. In other words, low use of both strategies differed from low suppression with high reappraisal. This is in line with previous studies on ER and gender differences, which found that for women the use of adaptive strategies (such as reappraisal) may have some compensatory effects among those with higher levels of maladaptive strategies (e.g., suppression). Such compensatory effects have not been shown for men (Nolen-Hoeksema, Citation2012).
Negative emotions in sexual contexts are linked to both impaired desire and reduced arousal, as well as heightened sexual distress (Bancroft, Loftus, & Long, Citation2003; Nobre & Pinto-Gouveia, Citation2006; Citation2008). With respect to ER, difficulties in ER have been associated with negative sexual outcomes regarding functionality, satisfaction (Rellini, Vujanovic, Gilbert, & Zvolensky, Citation2012; Rellini, Vujanovic, & Zvolensky, Citation2010) and compulsivity (Rendina et al., Citation2017). In this respect, ER abilities are important since they may enable the ability to effectively share emotions in intimate relationships, which is thought to indicate relationship functioning and satisfaction (Laurenceau, Barrett, & Rovine, Citation2005).
Our study adds to the literature, by emphasizing the importance of ER strategies for sexual function. The ability to flexibly choose between ER strategies, and to be able to cognitively reappraise events and emotions generated, are associated with sexual function. In addition, it supports the interpersonal ER model of women’s sexual dysfunction (Rosen & Bergeron, Citation2019) by supporting the negative effect of suppression and the positive effect of reappraisal for sexual function. This finding also reinforces the notion of ER ability as a transversal element in sexual function. Even though our study instruments did not focus on Genito-pelvic pain/penetration disorder (as did the model), we found the expected role of ER strategies for both men and women.
In the current study we used a cluster analytical approach as this methodology allows for the identification of profiles and, therefore, the characterization of ER groups and related patterns of ER with mental health and sexual function. The 4-group solution identified in the present study enabled a continuum perspective on the use of ER strategies and their effects on sexual function and mental health outcomes.
Limitations
First, due to the sexual function measures instruments used, no information about participants current sexual activity was collected. It is possible, therefore, that, for example, women’s scores of sexual function are inflated (no activity can either indicate no motivation to engage in it or the lack of possibility). Second, the data were obtained via an online survey from non-representative samples, which does not allow for the extrapolation of the results to the general population and may not fully reflect what is found in clinical settings. Third, despite being fluent in one of the languages, many respondents did not answer in their maternal native language, which may have impacted the reliability of the results. Also, regarding language, due to the different countries of origin of our sample, respondents may have answered questionnaire validated in their language but not necessarily validated in their country. Fourth, due to the cross-sectional nature of the study, no conclusions can be drawn on the stability of the cluster identified.
Implications
Based on our findings we were able to identify profiles of men and women regarding sexual function, anxiety and depression based on their ER strategy profiles. Both for men and women, the higher use of cognitive reappraisal was associated with better sexual function and mental health. From a clinical point of view, the current findings underline the importance of the assessment of ER strategies and the inclusion of ER strategies when conducting treatments for sexual and mental health. From a research point of view, further investigations on the impact of ER strategies for sexual health should be conducted, encompassing other strategies than suppression and reappraisal. Also, future research should investigate the relationship between ER strategies and sexual motivation and activity.
Conclusions
We identified distinct clinical subgroups with respect to anxiety, depression and sexual disorders based on their preferred ER strategies. By revealing the impact of ER strategies on sexual function, anxiety, and depression these findings support the inclusion of ER training as therapeutic goal in sexological care. Our findings highlight the association between sexual and mental health and suggest that when dealing with sexological patients, ER abilities should be assessed and emotion regulation training interventions fostering reappraisal should be used.
Authors contributions
VJF, GA, JB, AI and CV conceived of the study and developed the design of the study. AI performed the data analysis. VJF wrote the first draft of the manuscript, and all authors contributed revising it critically. The authors read and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Data is available upon request from the corresponding author.
Additional information
Funding
References
- Abler, B., & Kessler, H. (2009). Emotion regulation questionnaire – Eine deutschsprachige Fassung des ERQ von Gross und John. Diagnostica, 55(3), 144–152. doi:10.1026/0012-1924.55.3.144
- Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. doi:10.1016/j.cpr.2009.11.004
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Arlington, VA: American Psychiatric Publishing.
- Bancroft, J., Loftus, J. & Long, J. S. (2003). Distress about sex: A national survey of women in heterosexual relationships. Archives of Sexual Behavior, 32(June), 193–208. doi:10.1023/A:1023420431760
- Barlow, D. H., Sakheim, D. K., & Beck, J. G. (1983). Anxiety increases sexual arousal. Journal of Abnormal Psychology, 92(1), 49–54. doi:10.1037/0021-843X.92.1.49
- Batistoni, S. S. T., Ordonez, T. N., Silva, T. B. L. da, Nascimento, P. P. P. do, & Cachioni, M. (2013). Emotional Regulation Questionnaire (ERQ): indicadores psicométricos e relações com medidas afetivas em amostra idosa. Psicologia: Reflexão e Crítica, 26(1), 10–18. doi:10.1590/S0102-79722013000100002
- Beck, J. G., Barlow, D. H., Sakheim, D. K., & Abrahamson, D. J. (1987). Shock threat and sexual arousal: The role of selective attention, thought content, and affective states. Psychophysiology, 24(2), 165–172. doi:10.1111/j.1469-8986.1987.tb00273.x
- Berner, M. M., Kriston, L., Zahradnik, H.-P., & Härter, M. R. A. (2004). Überprüfung der Gültigkeit und Zuverlässigkeit des deutschen Female Sexual Function Index (FSFI-d). Geburtshilfe Und Frauenheilkunde, 64(3), 293–303. doi:10.1055/s-2004-815815
- Bloch, L., Haase, C. M., & Levenson, R. W. (2014). Emotion regulation predicts marital satisfaction: More than a wives’ tale. Emotion, 14(1), 130–144. doi:10.1037/a0034272
- Cabello, R., Salguero, J. M., Fernández-Berrocal, P., & Gross, J. J. (2013). A Spanish adaptation of the emotion regulation questionnaire. European Journal of Psychological Assessment, 29(4), 234–240. doi:10.1027/1015-5759/a000150
- Chervonsky, E., & Hunt, C. (2017). Suppression and expression of emotion in social and interpersonal outcomes: A meta-analysis. Emotion, 17(4), 669–683. doi:10.1037/emo0000270
- Crisp, C. C., Fellner, A. N., & Pauls, R. N. (2015). Validation of the Female Sexual Function Index (FSFI) for web-based administration. International Urogynecology Journal, 26(2), 219–222. doi:10.1007/s00192-014-2461-3
- D’Argembeau, A., & Van der Linden, M. (2006). Individual differences in the phenomenology of mental time travel: The effect of vivid visual imagery and emotion regulation strategies. Consciousness and Cognition, 15(2), 342–350. doi:10.1016/j.concog.2005.09.001
- Dargis, L., Trudel, G., Cadieux, J., Villeneuve, L., Préville, M., & Boyer, R. (2013). Validation of the International Index of Erectile Function (IIEF) and presentation of norms in older men. Sexologies, 22(1), e20–e26. doi:10.1016/j.sexol.2012.01.001
- Dèttore, D., Pucciarelli, M., Santarnecchi, E. (2013). Anxiety and female sexual functioning: an empirical study. Journal of Sex & Marital Therapy, 39(3), 216–240. doi:10.1080/0092623x.2011.606879
- Dewitte, M. (2014). On the interpersonal dynamics of sexuality. Journal of Sex & Marital Therapy, 40(3), 209–232. doi:10.1080/0092623X.2012.710181
- Diez-Quevedo C, Rangil T, Sanchez-Planell L, Kroenke K. S. R. (2001). Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosomatic Medicine, 63(4), 679–686. doi:10.1097/00006842-200107000-00021
- Doolan, E. L., Bryant, R. A., Liddell, B. J., & Nickerson, A. (2017). The conceptualization of emotion regulation difficulties, and its association with posttraumatic stress symptoms in traumatized refugees. Journal of Anxiety Disorders, 50, 7–14. doi:10.1016/j.janxdis.2017.04.005
- Dubé, J. P., Corsini-Munt, S., Muise, A., & Rosen, N. O. (2019). Emotion regulation in couples affected by female sexual interest/arousal disorder. Archives of Sexual Behavior, 48, 2491–2506. doi:10.1007/s10508-019-01465-4
- Ehring, T., Tuschen-Caffier, B., Schnülle, J., Fischer, S., & Gross, J. J. (2010). Emotion regulation and vulnerability to depression: Spontaneous versus instructed use of emotion suppression and reappraisal. Emotion, 10(4), 563–572. doi:10.1037/a0019010
- Fischer, V. J., Andersson, G., Billieux, J., & Vögele, C. (2022). The relationship between emotion regulation and sexual function and satisfaction: a scoping review. Sexual Medicine Reviews, 10(2), 195–208. doi:10.1016/j.sxmr.2021.11.004
- Garcia-Campayo, J., Zamorano, E., Ruiz, M. A., Pardo, A., Perez-Paramo, M., Lopez-Gomez, V., Freire, O., & Rejas, J. (2010). Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health and Quality of Life Outcomes, 8(1), 8. doi:10.1186/1477-7525-8-8
- Giraldi, A., Kristensen, E., & Sand, M. (2015). Endorsement of models describing sexual response of men and women with a sexual partner: An online survey in a population sample of Danish adults ages 20–65 years. The Journal of Sexual Medicine, 12(1), 116–128. doi:10.1111/jsm.12720
- Gonzáles, A. I., Sties, S. W., Wittkopf, P. G., Mara, L. S. de, Ulbrich, A. Z., Cardoso, F. L., & Carvalho, T. de. (2013). Validation of the International Index of Erectile Function (IIFE) for Use in Brazil. Arquivos Brasileiros de Cardiologia. 101(2), 176–182. doi:10.5935/abc.20130141
- Gräfe, K., Zipfel, S., Herzog, W., & Löwe, B. (2004). Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ-D)”. Diagnostica, 50(4), 171–181. doi:10.1026/0012-1924.50.4.171
- Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. doi:10.1023/B:JOBA.0000007455.08539.94
- Gross, J. (2002). Emotion regulation: Affective, cognitive, and social consequences. Psychophysiology, 39(3), S0048577201393198. doi:10.1017/S0048577201393198
- Gross, J. J. (1998). The emerging field of emotion regulation: An integrative review. Review of General Psychology, 2(3), 271–299. doi:10.1037/1089-2680.2.3.271
- Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. doi:10.1037/0022-3514.85.2.348
- Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis: A global perspective. London: Pearson Education.
- Hawton, K., & Catalan, J. (1986). Prognostic factors in sex therapy. Behaviour Research and Therapy, 24(4), 377–385. doi:10.1016/0005-7967(86)90002-1
- Hernández, R., Thieme, T., & Araos, F. (2017). Adaptación y Análisis Psicométrico de la Versión Española del Índice Internacional de Función Eréctil (IIEF) en Población Chilena. Terapia Psicológica, 35(3), 223–230. doi:10.4067/S0718-48082017000300223
- Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., Wirkner, K., & Hilbert, A. (2017). Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. Journal of Affective Disorders, 210, 338–344. doi:10.1016/j.jad.2016.12.012
- Houck, C. D., Barker, D. H., Hadley, W., Menefee, M., & Brown, L. K. (2018). Sexual risk outcomes of an emotion regulation intervention for at-risk early adolescents. Pediatrics, 141(6), 1–11. doi:10.1542/peds.2017-2525
- Janssen, E., Everaerd, W., Spiering, M., & Janssen, J. (2000). Automatic processes and the appraisal of sexual stimuli: Toward an information processing model of sexual arousal. Journal of Sex Research, 37(1), 8–23. doi:10.1080/00224490009552016
- John, O. P., & Gross, J. J. (2004). Healthy and unhealthy emotion regulation: Personality processes, individual differences, and life span development. Journal of Personality, 72(6), 1301–1334. doi:10.1111/j.1467-6494.2004.00298.x
- Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9. Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. doi:10.1046/j.1525-1497.2001.016009606.x
- Laan, E., Everaerd, W., Van Aanhold, M.-T., & Rebel, M. (1993). Performance demand and sexual arousal in women. Behaviour Research and Therapy, 31(1), 25–35. doi:10.1016/0005-7967(93)90039-W
- Laurenceau, J.-P., Barrett, L. F., & Rovine, M. J. (2005). The interpersonal process model of intimacy in marriage: A daily diary and multilevel modeling approach. Journal of Family Psychology, 19, 314–323. doi:10.1037/0893-3200.19.2.314
- Leiblum, S. R., & Rosen, R. C. (2000). Principles and practice of sex therapy. New York: Guilford Press.
- Lewis, R. W., Fugl-Meyer, K. S., Corona, G., Hayes, R. D., Laumann, E. O., Moreira, E. D., Rellini, A. H., & Segraves, T. (2010). Definitions/epidemiology/risk factors for sexual dysfunction. The Journal of Sexual Medicine, 7(4), 1598–1607. doi:10.1111/j.1743-6109.2010.01778.x
- Lutz, J., Gross, R. T., & Vargovich, A. M. (2018). Difficulties in emotion regulation and chronic pain-related disability and opioid misuse. Addictive Behaviors, 87, 200–205. doi:10.1016/j.addbeh.2018.07.018
- Madioni, F., & Mammana, L. A. (2001). Toronto Alexithymia scale in outpatients with sexual disorders. Psychopathology, 34(2), 95–98. doi:10.1159/000049287
- McCabe, M. P. (2005). The role of performance anxiety in the development and maintenance of sexual dysfunction in men and women. International Journal of Stress Management, 12(4), 379–388. doi:10.1037/1072-5245.12.4.379
- Mills, S. D., Fox, R. S., Malcarne, V. L., Roesch, S. C., Champagne, B. R., & Sadler, G. R. (2014). The psychometric properties of the Generalized Anxiety Disorder-7 Scale in Hispanic Americans with English or Spanish language preference. Cultural Diversity and Ethnic Minority Psychology, 20(3), 463–468. doi:10.1037/a0036523
- Monteiro, S., Torres, A., Pereira, A., Albuquerque, E., & Morgadinho, R. (2013). 2077 – Preliminary validation study of a portuguese version of the patient health questionnaire (PHQ-9). European Psychiatry, 28, 1. doi:10.1016/S0924-9338(13)76982-7
- Moreno, A. L., DeSousa, D. A., Souza, A. M. F. L. P., Manfro, G. G., Salum, G. A., Koller, S. H., Osório, F. L., & Crippa, J. A. S. (2016). Factor structure, reliability, and item parameters of the Brazilian-Portuguese Version of the GAD-7 questionnaire. Temas Em Psicologia, 24(1), 367–376. doi:10.9788/TP2016.1-25
- Nobre, P. J., & Pinto-Gouveia, J. (2006). Emotions during sexual activity: differences between sexually functional and dysfunctional men and women. Archives of Sexual Behavior, 35(4), 491–499. doi:10.1007/s10508-006-9047-1
- Nobre, P. J., & Pinto-Gouveia, J. (2008). Cognitions, emotions, and sexual response: analysis of the relationship among automatic thoughts, emotional responses, and sexual arousal. Archives of Sexual Behavior, 37(4), 652–661. doi:10.1007/s10508-007-9258-0
- Nolen-Hoeksema, S. (2012). Emotion regulation and psychopathology: the role of gender. Annual Review of Clinical Psychology, 8(1), 161–187. doi:10.1146/annurev-clinpsy-032511-143109
- Pacagnella, R. D. C., Vieira, E. M., RodriguesJr, O. M., & Souza, C. D. (2008). Cross-cultural adaptation of the female sexual function index. Cadernos de Saude Publica, 24(2), 416–426. doi:10.1590/s0102-311x2008000200021
- Payne, K. A., Binik, Y. M., Amsel, R., & Khalifé, S. (2005). When sex hurts, anxiety and fear orient attention towards pain. European Journal of Pain, 9(4), 427–427. doi:10.1016/j.ejpain.2004.10.003
- Pepping, C. A., Cronin, T. J., Lyons, A., & Caldwell, J. G. (2018). The effects of mindfulness on sexual outcomes: the role of emotion regulation. Archives of Sexual Behavior, 47(6), 1601–1612. doi:10.1007/s10508-017-1127-x
- Pepping, C. A., O’donovan, A., Zimmer-gembeck, M. J., & Hanisch, M. (2014). Is emotion regulation the process underlying the relationship between low mindfulness and psychosocial distress? Australian Journal of Psychology, 66(2), 130–138. doi:10.1111/ajpy.12050
- Rellini, A. H., Vujanovic, A. A., Gilbert, M., & Zvolensky, M. J. (2012). Childhood maltreatment and difficulties in emotion regulation: Associations with sexual and relationship satisfaction among young adult women. Journal of Sex Research, 49(5), 434–442. doi:10.1080/00224499.2011.565430
- Rellini, A. H., Vujanovic, A. A., & Zvolensky, M. J. (2010). Emotional dysregulation: Concurrent relation to sexual problems among trauma-exposed adult cigarette smokers. Journal of Sex & Marital Therapy, 36(2), 137–153. doi:10.1080/00926230903554545
- Rendina, H. J., Gamarel, K. E., Pachankis, J. E., Ventuneac, A., Grov, C., & Parsons, J. T. (2017). Extending the minority stress model to incorporate HIV-positive gay and bisexual men’s experiences: A longitudinal examination of mental health and sexual risk behavior. Annals of Behavioral Medicine, 51(2), 147–158. doi:10.1007/s12160-016-9822-8
- Rogier, G., Garofalo, C., & Velotti, P. (2019). Is emotional suppression always bad? A matter of flexibility and gender differences. Current Psychology, 38, 411–420. doi:10.1007/s12144-017-9623-7
- Rosen, N. O., & Bergeron, S. (2019). Genito-pelvic pain through a dyadic lens: Moving toward an interpersonal emotion regulation model of women’s sexual dysfunction. The Journal of Sex Research, 56(4–5), 440–461. doi:10.1080/00224499.2018.1513987
- Rosen, C. Brown, J. Heiman, S. Leib, R. (2000). The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. Journal of Sex & Marital Therapy, 26(2), 191–208. doi:10.1080/009262300278597
- Rosen, R. C., Riley, A., Wagner, G., Osterloh, I. H., Kirkpatrick, J., & Mishra, A. (1997). The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology, 49(6), 822–830. doi:10.1016/S0090-4295(97)00238-0
- Simonelli, C., Bonanno, D., Michetti, P. M., & Rossi, R. (2008). Premature ejaculation and dysregulation of emotions: Research and clinical implications. Sexologies, 17(1), 18–23. doi:10.1016/j.sexol.2007.07.003
- Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder. Archives of Internal Medicine, 166(10), 1092. doi:10.1001/archinte.166.10.1092
- Taylor, G. J., Michael Bagby, R., & Parker, J. D. A. (1991). The alexithymia construct: A potential paradigm for psychosomatic medicine. Psychosomatics, 32(2), 153–164. doi:10.1016/S0033-3182(91)72086-0
- Thiel, R. do R. C., Dambros, M., Palma, P. C. R., Thiel, M., Riccetto, C. L. Z., & Ramos, M. de F. (2008). Tradução para português, adaptação cultural e validação do Female Sexual Function Index. Revista Brasileira de Ginecologia e Obstetrícia, 30(10), 504–510. doi:10.1590/S0100-72032008001000005
- Vallejo-Medina, P., Pérez-Durán, C., & Saavedra-Roa, A. (2018). Translation, adaptation, and preliminary validation of the female sexual function index into Spanish (Colombia). Archives of Sexual Behavior, 47(3), 797–810. doi:10.1007/s10508-017-0976-7
- Vujanovic, A. A., Zvolensky, M. J., & Bernstein, A. (2008). The interactive effects of anxiety sensitivity and emotion dysregulation in predicting anxiety-related cognitive and affective symptoms. Cognitive Therapy and Research, 32(6), 803–817. doi:10.1007/s10608-007-9148-8
- Webb, T. L., Miles, E., & Sheeran, P. (2012). Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychological Bulletin, 138(4), 775–808 doi:10.1037/a0027600
- Wiegel, M., Meston, C., & Rosen, R. (2005). The Female Sexual Function Index (FSFI): Cross-validation and development of clinical cutoff scores. Journal of Sex & Marital Therapy, 31(1), 1–20. doi:10.1080/00926230590475206
- Willi, J. Burri, A. (2015). Emotional intelligence and sexual functioning in a sample of Swiss men and women. Journal of Sexual Medicine, 12(10), 2051–2060. doi:10.1111/jsm.12990
- Wiltink, J., Hauck, E. W., Phädayanon, M., Weidner, W., & Beutel, M. E. (2003). Validation of the German version of the International Index of Erectile Function (IIEF) in patients with erectile dysfunction, Peyronie’s disease and controls. International Journal of Impotence Research, 15(3), 192–197. doi:10.1038/sj.ijir.3900997
- World Health Organization. (2023). Mental health fact sheets. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
- Wylomanski, S., Bouquin, R., Philippe, H.-J., Poulin, Y., Hanf, M., Dréno, B., Rouzier, R., & Quéreux, G. (2014). Psychometric properties of the French Female Sexual Function Index (FSFI). Quality of Life Research, 23(7), 2079–2087. doi:10.1007/s11136-014-0652-5