
Abstract
Introduction: A new form of internationalization has been trending upward in the medical education realm: crossborder medical curriculum partnerships established to deliver the same, or adapted, curriculum to groups of geographically separated students. This study aims to investigate crossborder medical curriculum partnerships by exploring the experiences of teachers at the recipient institution who have a key role in delivering the program.
Methods: From four pioneering recipient medical schools, 24 teachers participated in a Q-sort study. Each participant rank-ordered 42 statements about teaching in a crossborder medical curriculum on a scale from −5 (indicating strong disagreement) to +5 (indicating strong agreement). The authors conducted a “by-person” factor analysis to uncover distinct patterns in the ranking of statements, using the statistical results and participants’ comments about their Q sorts to interpret these patterns and translate them into distinct viewpoints.
Results: Three viewpoints emerged, reflecting: (1) a feeling of connectedness with the partner institution, trust in the quality of the curriculum, and appreciation of interinstitutional relationships; (2) the partnership’s attractiveness because of the career opportunities it offers; and (3) concerns over the quality of graduates because of doubts about the appropriateness of the didactic model and insufficient attention to local healthcare needs, and over the practical feasibility of such partnerships.
Conclusions: The three viewpoints identified revealed a pallet of views on how host teachers might experience their work. It shows the heterogeneous features of this group and seems to counterbalance reports that they are feeling “deprived” from their role as teacher. Two viewpoints featured an appreciation of interinstitutional relationships and of the partnership, especially when perceiving a degree of autonomy. Partners can capitalize on all different viewpoints by deploying procedure and policies to raise the quality of education delivery.
Introduction
In the last decade, a number of medical schools have entered into crossborder curriculum partnerships (CCPs). In such partnerships, it is the curriculum, not students or faculty, that crosses borders from the location where it was developed (home) to an institution (host) where it will be delivered (Knight Citation2008). This transfer of the curriculum can be realized through various legal forms ranging from branch campuses to franchises or delivery agreements with host public or private providers, which of course influence the way the partnership is shaped. However, the overarching communality of these partnerships is to provide a comparable learning experience to students at both institutions. It has been argued that CCPs are a logical next embodiment of globalization in higher education following the student and teacher exchanges of the previous decades (Harden Citation2006). According to a report from the British Council (Citation2013), this type of partnership is rapidly expanding and has high-potential growth rates. Key actors in such crossborder medical curriculum partnerships are host teachers as they are expected to deliver a program that has been developed by another institution. Although host staff are typically well qualified and employed full-time, they often have no experience with the program and teaching method of the home institution (Verbik et al. Citation2006; Shams and Huisman Citation2012; Märzheuser-Wood and Chatwood Citation2014).
Despite the pivotal role host teachers play, only a few studies outside of health care education have spotlighted their experiences and perceptions. What these studies revealed is that host staff could experience little ownership of the program. Programs have been adopted from the home institution and the host teachers have not been involved in the creation of new educational materials in substantial ways (Smith Citation2009). Teachers were cited to “… just follow the syllabus” and “just [be] here to follow the home institution” (Dobos Citation2011). These studies also reported incidences of host staff feeling maltreated by their partners, whom they perceived as being disinterested, ignorant, and feeling superior (Smith Citation2009; Dobos Citation2011). Furthermore, Waterval et al. (Citation2014) identified that the necessary communication processes in curriculum partnerships between host and home teachers could be perceived as frustrating due to the use of email for correspondence, time zone differences, and large geographic distances.
Although, curriculum partnerships are often initiated by higher management (OECD Citation2004; Wilkins and Huisman Citation2012), the teachers perceptions and enthusiasm for the partnership determines to a large extent the quality of curriculum implementation. The purpose of this study is therefore to canvass host teachers’ views on teaching in a CCP, thereby contributing to the current debate on the pros and cons of this relatively novel form of internationalization that is growing in medical education and beyond (Kosmutzky and Putty Citation2016).
Methods
Setting
We purposively selected six medical partnerships that delivered a home institution’s curriculum at a host institution across borders, with the aim to provide comparable learning experiences to cohorts of geographically separated students (Waterval et al. Citation2016). In all partnerships, host teachers were familiarized and trained about content and processes of the home curriculum through mutual visits and online sessions. This study furthermore revealed that none of the partnerships had a predefined overview of the type of adaptations planned or required from host faculty. While two institutions declined due to a lack of time or interest, four responded positively to our email invitation to participate in this study. Supplementary Appendix 1 summarizes the participating partnerships and their characteristics.
Q methodology
To investigate host teachers’ perceptions of teaching in a medical curriculum partnership, we used Q methodology. An organized means to identify opinions and priorities among a group (Watts and Stenner Citation2005), this technique has been effectively used to study a wide range of topics in education and the health sciences (Barker Citation2008; Nikolaus et al. Citation2010; Wallenburg et al. Citation2010; Daniels and Kassam Citation2013; Meade et al. Citation2013; Perz et al. Citation2013; Fokkema et al. Citation2014). In applying the method, we purposively selected a representative number of participants and invited them to rank-order a set of statements about the research question on a scale ranging from “disagree most strongly” to “agree most strongly.” As the method aims to describe a population of viewpoints, and not, as is the case with conventional survey analyses, of people, we did not require a large sample (Watts and Stenner Citation2005). Each participant recorded his or her ranking of statements on the score sheet (the Q sort) depicted in and consequently participated in a short qualitative interview in which they commented verbally on the statements placed at the Q sort extremities.
Figure 1. The Q-sort grid.
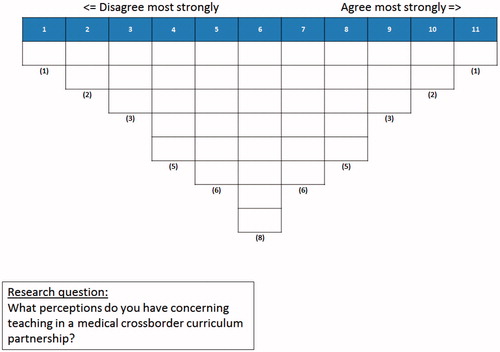
This data collection was followed by a “by-person” factor analysis of participants’ Q sorts to discover patterns in the statement rankings. Unlike traditional factor analysis, the objective of which is to identify correlations between variables across a sample of participants, Q methodology aims to detect correlations between participants across a number of variables, in this case statements. Assuming that such correlations indicated similarity of participants’ viewpoints, we used the statistical results and qualitative data from the post-Q-sort interviews to interpret these patterns and to translate them into distinct viewpoints.
Development of the Q set
Critical to Q methodology is the effective development of the research instrument, i.e. the set of statements (Q set) to be sorted. Although the generation of items does not follow a fixed procedure, an effective Q set should meet two important criteria. First, the statements should adequately represent the discourse on the topic of study, allowing for expression of all possible viewpoints (Brown Citation1996; Watts and Stenner Citation2012). Hence, they must cover all the ground and be rooted in real existence (Brown Citation1996). Second, the Q set should be balanced, ensuring the absence of bias toward any particular viewpoint (Watts and Stenner Citation2012).
To assemble the pool of statements about teaching in a CCP, we drew on two of our previous studies: a literature review of the factors that make or break CCPs (Waterval et al. Citation2014) and a qualitative study for which we interviewed 13 directors of host and home medical CCPs (Waterval et al. Citation2016). In doing so, we specifically focused on the data pertinent to the challenges host teachers face. The initial Q set that resulted comprised 48 statements and was structured around six themes: “ownership of curriculum materials,” “communication and relationship with home staff,” “challenges related to differences in learning styles,” “understanding of teaching philosophy of home institution,” “fit between adapted home curriculum and local healthcare setting,” and “miscellany.”
After all authors had reviewed the initial Q set for ambiguity, clarity, and suitability, D.W. made adjustments based on their comments. Research team members E.D., A.M., and J.F. and one host teacher then performed a dry run of the Q set to test its adequacy by completing a Q sort and critically reviewing the Q sort instructions and post-Q-sort questions (see supplemented Appendix 2). A second round of adjustments ensued, resulting in a final set of 42 statements (between 40 and 50 is most common) (Brown Citation1996; Watts and Stenner Citation2005). Finally, we randomly numbered the backside of the final statements and printed them on laminated cards for use by participants during their Q sorts.
Participant recruitment and procedure
The Q-methodological approach to recruiting participants (the P set) is to select them strategically in accordance with the study’s purpose (Watts and Stenner Citation2012). In our case, and in coordination with the host program directors, we identified 24 participants based on their long-term involvement in the partnership, preferably from the start, and their ability to provide the information sought after. Additionally, we aimed at an even distribution in terms of gender and participants’ expertise (basic/social sciences, and clinicians). All participants were approached by the researcher and volunteered to participate. presents the final list of teachers who participated. The first author and on one occasion a research assistant visited each participating institution in the period spanning December 2015 to March 2016, during which time all participants received written and verbal instructions. After completing the Q sort by placing the 42 cards on the score sheet (see ), participants provided comments on the statements they rank-ordered at the extremities. The entire exercise took participants 45 minutes on average to complete.
Table 1. P set overview: the 24 participants categorized into gender, partnership, academic background, and viewpoint loadings.
Analysis
We analyzed the data using dedicated software (PQMethod 2.11, schmolck.userweb.mwn.de/qmethod). A first exploration pointed to different numbers of factors: six when applying the “eigenvalue > 1” criterion; two or three based on the scree plot; and three or four when adopting Watts and Stenner’s rule of thumb to employ one factor for each 6–8 Q sorts (Watts and Stenner Citation2012). To find the appropriate solution, we trialed 3- to 5-factor structures using PCA and varimax. A four-factor solution, combined with a 0.45 significance threshold for the loadings, resulted in a minimum number of confounding Q sorts. After dismissing one of the factors for being associated with only one Q sort, a final, three-factor structure remained.
For each of these factors, using the PQMethod software, we generated an idealized Q sort – the score pattern over the set of statements – representing how someone teaching in a medical CCP with exactly that viewpoint would have ranked the 42 statements in the sorting grid. In the process, we flagged the statements that for a particular factor were ranked significantly differently (p < 0.05 or p < 0.01) from all other factors as “distinguishing statements.” Statements that did not distinguish between any pair of factors (p > 0.05) were identified as “consensus statements.” Finally, D.W. and J.F. independently interpreted each factor’s score pattern and translated them into viewpoints, using the crib-sheet method (Watts and Stenner Citation2012), the distinguishing statements, and the comments of participants whose Q sorts were associated with the respective viewpoint.
Results
The three viewpoints had respectively seven, seven, and two defining Q sorts (i.e. participants statistically significantly associated with the viewpoint). Together, the three viewpoints accounted for 57% of the variance in the 24 Q-sorts (see ).
Table 2. Distribution of the three emerging viewpoints regarding teaching in a medical crossborder curriculum partnership.
For each viewpoint, presents the levels of agreement on each statement on a scale from −5 to +5. In the following, we will give a detailed description of each viewpoint based on the statements that were flagged as distinguishing and characteristic of the viewpoint, illustrated by a representative quote from one of the participants. The information in parentheses refers to the statement number listed in (1–42) and the factor score (−5 to +5), respectively.
Table 3. The Q set and associated Q-sort values, indicating for each factor the average level of agreement on each statement (on a scale from −5 to +5).
Viewpoint 1: connected with home institution
Adherents of this viewpoint had great trust in the curriculum. They felt the partnership produced graduates of higher quality than would have been the case if they had developed all the educational materials themselves (37: +4). More than their peers who embraced the other two viewpoints, they strongly rejected the notion that the student-centered learning and assessment methodology of the home program would not work in their setting (38: −4, 39: −5). Neither did they believe the program did not cover certain diseases that were essential to the local context (1: −1). In a similar vein, they were more optimistic about the program being of benefit to students’ future careers (42: +4), but less so about its relevance to the local healthcare system (40; 0).
Another conviction that marks this viewpoint is that good relationships between host and home staff are essential to the delivery of a high-quality curriculum (2: +5). This may be because exemplars of this viewpoint felt more strongly than others that working with educational materials that had been constructed by someone else was difficult (15: 0). As such they felt part of the home institution’s teaching community (13: +2). In the words of one clinician (teacher 24, partnership D): “Any collaboration requires collaboration and communication at all levels. It is the glue to success; it helps them stick. Both parties should be interested; that is what makes collaboration and communication more effective.”
The Q sorts of seven participants (four females, three males) loaded onto this viewpoint, including four social scientists, two clinicians, and one basic scientist. The majority (5) were teachers from partnership B, while the remaining two participants came from partnership C and D.
Viewpoint 2: attracted because of career opportunities
The teachers represented by this viewpoint felt that working in the context of a CCP offered many career advantages (36: +5). They strongly disagreed with the statement that teaching in this context was unattractive (35: −4). Instead, they were rather proud to share in the reputation of the home institution (23: +4). To a slightly lesser degree than the group previously discussed, these teachers also had significant trust in the curriculum and positive attitudes toward the partnership regarding matters of coordination with and involvement of the home institution (42: 2, 5: 0, 19: −5, 33: −1, 34: −2). This optimism was also reflected in teachers’ confirmation that the new language of instruction, assessment methods, and required learning style were suitable for their students (6: 2, 38: −1).
Despite this optimism, however, teachers in this group were more convinced that the program did not cover certain diseases that were essential to the local context (1: +1). Consequently, they were only moderately enthusiastic about the program’s relevance to the local healthcare setting (40: 1), favoring a certain amount of independence from their home partners and adaptation of the home curriculum to their context. They did not experience a high level of interference from home teachers (25: −1), and were neutral about feeling part of the home institution’s teaching community (13: 0). Although creating educational content themselves was not among their priorities (20: −3), they did appreciate the opportunity to work with the home program and to adapt it. One basic scientist (teacher 20, partnership D) who exemplifies this viewpoint remarked: “Working in such a partnership provides more challenges and opportunities for me as faculty, which I benefitted from. Think of adjusting curriculum materials to the local context. Furthermore, the reputation of this home institution is very attractive and good for my career.”
Seven participants (four males, three females) were associated with this viewpoint, including five clinicians, and two basic scientists. Four of them were affiliated to partnership A, one to partnership C, and two to partnership D.
Viewpoint 3: concerned about appropriateness
The teachers who espoused this view were more critical of the home program and of its fit with the local healthcare context (40: −2). They were less confident that the program adequately prepared students for practice in the local healthcare setting (8: 0), also because they felt the curriculum lacked coverage of certain essential local diseases (1: +5), which, in turn, translated into a neutral stance toward the program being of benefit to graduates’ careers (42: 0). Their critical attitude also extended to the teaching and assessment methods of the home institution, which they did not always consider appropriate for their students (38: 2, 39: −1). Besides believing that students’ learning experiences differed between home and host institution (32: −3), these teachers did not appear to fully understand the philosophy of the home institution (18: −1), and certainly did not feel part of its teaching community (13: −5). They were not particularly positive about working in the context of a CCP (33: 3, 35: 0), and despite the fact that they found it easy to work with educational materials constructed by others (15: −4), they missed creating educational content themselves (20: 3, 21: 1).
This viewpoint is best captured by teacher 23 (basic scientist, partnership D), who noted that “..adjustments to the local situation are needed, not so much in [terms of] quantity, but of quality. Prevalence of certain diseases makes it essential to look for the differences in the local setting and adjust the program locally”. Two male teachers loaded onto this viewpoint: one basic scientist from partnership C and one clinician from partnership D.
Shared perceptions
As noted earlier, we also identified several consensus statements indicating similarity of viewpoints. For instance, none of the teachers felt inferior when communicating with home partners (22: −4, −3, −2) and all felt they had good relationships with their colleagues abroad (17: 2, 1, 1). Importantly, they all agreed that their students were able to attain the same intended learning objectives as home students did (7: 3, 2, 4).
Discussion
In this study, we have sought to capture the views of host teachers from four different partnerships on teaching in a crossborder medical curriculum partnership. Their viewpoints show that various aspects of the teaching experience are valued differently by host teachers, even if they work in the same context. Concerns expressed by one critical viewpoint echo previous warnings from medical scholars about home programs not being sufficiently adapted to local circumstances (Whitehead Citation2016). These findings lend further credence to the assertion that curriculum partnerships may fail to respond to the needs of the local healthcare system. The other two viewpoints show a different, more optimistic side of the teaching experienced which have been less reported in literature.
Some medical host teachers felt proud to deliver the home program and were relatively confident about its quality, as evidenced by the “connected with home institution” and “attracted because of career opportunities” viewpoints. What is more, they enjoyed the opportunity to work with materials from the home institution, as they felt it would enhance their teaching competence and career prospects. They were not dissatisfied with the program content, nor did they feel disempowered or alienated from what was on offer to students.
These first two viewpoints might be in opposition to the more concerned viewpoint, this could also be related to the amount of autonomy perceived by host teachers to be able to adapt and modify the content up to their insights. For instance, all viewpoints were positive about the working relationships with home staff. This seems to support findings indicating that feelings of control and ownership among host teachers were shown to be important determinants of job satisfaction (Toohey et al. Citation2017). As such the fact that the curriculum had initially been developed by another institution did not make them feel deprived of their role as teacher (Keay et al. Citation2014).
Although on one occasion a personal distorted relationship between a home and host course coordinator was mentioned as an illustration during the post Q-sort interview, a structural widespread troubled relationship did not emerge from our viewpoint analyses. The host teachers in our study did not report feelings of inferiority caused by inappropriate attitudes of home teachers as noted elsewhere (Bodycott and Walker Citation2000; Dobos Citation2011).
These findings offer a beginning of understanding on host staff’s attitudes toward cross-border partnerships. Further studies are recommended in more contexts and with different methodologies to broaden our understanding of the dynamics of staff within CCPs.
Several factors should be taken into account when relating our findings to those of previous studies. First, differences in research context may account for variations, as, to our knowledge, this research was the first to be conducted in the area of medical education. Next, our use of Q-sort methodology and associated quantitative analyses may have led to the emergence of main perceptions only, filtering out individual experiences that qualitative interviewing techniques would otherwise have detected. Our pool of statements, though diverse, did not incorporate every possible teaching experience within a crossborder curriculum context, which narrowed the range of possible perceptions to identify. Furthermore, we cannot rule out a selection bias in recruiting participants as host program coordinators helped to identify a first list that complied with the selection criteria. Finally, Q-sorts might have been biased by a perceived lack of confidentiality as they were purposively selected. Although this cannot be excluded, during the performance of the Q-sort and the post Q-sort questionnaire most teachers expressed their thoughts and concerns in a free and open atmosphere. Many expressed an appreciation for the methodology.
Drawing on these insights, we argue that partnership managers on both sides could put these divergent views to constructive use by appropriate policies and procedures. Responding to the concerns raised by adherents of viewpoint 3, for instance, the partnership could commission formal committees to adapt the home curriculum to the local context. Inviting critical teachers to serve on these committees would create a win-win situation: not only would the curriculum become better adapted, it would also remove some of their valid concerns.
Similarly, managers could support the teachers who feel connected and attracted by implementing communication policies and procedures between coordinators, and removing all technical communication barriers from the start. This is likely to foster strong links and facilitate engagement and interaction between teachers from both sides. Keay et al. (Citation2014), as well as the British quality assurance agency overseeing the quality of crossborder programs, argued that working toward the development of communities of practice, promoting a focus on the quality of the relationship between partners, will enhance the learning experience for host students. In addition, a recent study suggests that strong linkages between partners may also have a positive effect on the levels of commitment and satisfaction among the home teachers within a curriculum partnership (Toohey et al. Citation2017).
The role of home teachers has been left outside the scope of this research, but deserves more in-depth follow-up. In particular, it would be interesting to investigate how home teachers’ attitudes are influenced by the management of curriculum partnerships and interactions with host staff.
Unfortunately, present-day medical curriculum partnerships are not so much concerned with establishing communities of practice as with the transfer of knowledge about the curriculum and didactics by fly-in, fly-out home teachers (Waterval et al. Citation2016). In doing so, they overlook host teachers’ willingness and preparedness to engage, interact, and form joint course coordinating groups. Communities of practice will not only support host teachers in their daily activities, they will also render a more sustainable partnership. They can serve as principal platforms for the required frequent and effective communication on multiple organizational levels (Waterval et al. Citation2017). As a result, the curriculum partnership can grow to become truly bilateral, such that a “network partnership” may come to evolve that could eventually span other issues of collaboration besides the curriculum. We therefore welcome future research into the factors that promote the establishment of effective communities of practice between teachers in a CCP.
Ethical approval
The study was approved by the ethical review board of the Netherlands Association for Medical Education (NVMO-ERB; file number 579).
Glossary
Crossborder curriculum partnership: Two institutions located in different countries strive for equivalence – i.e. comparability – in terms of curriculum content and learning experiences to students in both institutions (Knight 2006). These partnerships can take many different legal forms, such as branch campuses, delivery agreements, or franchises of complete programs, they all share that the curriculum developed in one place, the home institution, is transferred across borders to the other, or host institution.
Knight J. 2006. Crossborder education: conceptual confusion and data deficits. Perspec in Educ. 24(4):15–27.
Notes on contributors
Dominique G. J. Waterval, MHPE, is a Manager of international projects and PhD student, School of Health Professions Education, Maastricht University, Maastricht, The Netherlands.
Janneke M. Frambach, PhD, is an Assistant Professor, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands.
Erik W. Driessen, PhD, is a Professor and Chair of the Department of Educational Development and Research, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands.
Arno Muijtjens, PhD, is an Associate Professor, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands.
Albert J. J. A. Scherpbier, MD, PhD, is a Professor and Dean, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands.
Dominique_G._J._Waterval_et_al._Supplementary_files.zip
Download Zip (35.9 KB)Acknowledgments
The authors wish to thank Mohammed Meziani for his assistance in the data collection, Angelique Van den Heuvel for the language editing and helpful comments, and the participants for their contribution to the research project.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
- Barker JH. 2008. Q-methodology: an alternative approach to research in nurse education. Nurse Educ Today. 28:917–925.
- Bodycott P, Walker A. 2000. Teaching abroad: lessons learned about inter-cultural understanding for teachers in higher education. Teach High Educ. 5:79–94.
- British Council. 2013. The shape of things to come 2. The evolution of transnational education: data, definitions, opportunities and impacts analysis; [accessed 28 Aug 2014]. http://www.britishcouncil.org/sites/britishcouncil.uk2/files/the_shape_of_things_to_come_2.pdf.
- Brown SR. 1996. Q methodology and qualitative research. Qual Health Res. 6:561–567.
- Daniels V, Kassam N. 2013. Impact of personal goals on the internal medicine R4 subspecialty match: a Q methodology study. BMC Med Educ. 13:1–9.
- Dobos K. 2011. “Serving two masters” – academics’ perspectives on working at an offshore campus in Malaysia. Educ Rev. 63:19–35.
- Fokkema JP, Scheele F, Westerman M, van Exel J, Scherpbier AJ, van der Vleuten CP, Dorr PJ, Teunissen PW. 2014. Perceived effects of innovations in postgraduate medical education: a Q study focusing on workplace-based assessment. Acad Med. 89: 1259–1266.
- Harden RM. 2006. International medical education and future directions: a global perspective. Acad Med. 81:S22–S29.
- Keay J, May H, O’ Mahony J. 2014. Improving learning and teaching in transnational education: can communities of practice help? Jet. 40:251–266.
- Knight J. 2008. Higher education in turmoil. Toronto (ON): Sense Publishers.
- Kosmutzky A, Putty R. 2016. Transcending borders and traversing boundaries: a systematic review of the literature on transnational, offshore, cross-border, and borderless higher education. J Stud Int Educ. 20:8–33.
- Märzheuser-Wood B, Chatwood R. 2014. How education providers are growing internationally through the strategic use of franchising; [accessed 2014 Sep]. http://www.mondaq.com/x/335030/Franchising/How+education+providers+are+growing+internationally+through+ the+strategic+use+of+franchising.
- Meade LB, Caverzagie KJ, Swing SR, Jones RR, O’Malley CW, Yamazaki K, Zaas AK. 2013. Playing with curricular milestones in the educational sandbox: Q-sort results from an internal medicine educational collaborative. Acad Med. 88:1142–1148.
- Nikolaus S, Bode C, Taal E, van de Laar MA. 2010. Four different patterns of fatigue in rheumatoid arthritis patients: results of a Q-sort study. Rheumatology. 49:2191–2199.
- OECD. 2004. Internationalisation and trade in higher education opportunities and challenges. Paris: OECD.
- Perz J, Ussher J, Gilbert E. 2013. Constructions of sex and intimacy after cancer: Q methodology study of people with cancer, their partners, and health professionals. BMC Cancer. 13:13.
- Shams F, Huisman J. 2012. Managing offshore branch campuses: an analytical framework for institutional strategies. J Stud Int Educ. 16:106–127.
- Smith L. 2009. Sinking in the sand? Academic work in an offshore campus of an Australian university. HERD. 28:467–479.
- Toohey D, McGill T, Whitsed C. 2017. Engaging academic staff in transnational teaching: the job satisfaction challenge. J Stud Int Educ. 21:333–348.
- Verbik L, Rumbley LE, Altbach PG. 2006. The international branch campus – models and trends. London: Observatory of Bordeless Higher Education.
- Wallenburg I, van Exel J, Stolk E, Scheele F, de Bont A, Meurs P. 2010. Between trust and accountability: different perspectives on the modernization of postgraduate medical training in the Netherlands. Acad Med. 85:1082–1090.
- Waterval DGJ, Frambach JM, Driessen EW, Scherpbier AJJA. 2014. Copy but not paste: a literature review of crossborder curriculum partnerships. J Stud Int Educ. 19:65–85.
- Waterval DGJ, Frambach JM, Oudkerk Pool A, Driessen EW, Scherpbier AJJA. 2016. An exploration of crossborder medical curriculum partnerships: balancing curriculum equivalence and local adaptation. Med Teach. 38:255–262.
- Waterval DGJ, Tinnemans-Adriaanse M, Meziani MA, Driessen EW, Scherpbier AJJA, Mazrou A, Frambach JM. 2017. Exporting a student-centred curriculum: a home institution’s perspective. J Stud Int Educ. 21:278–290.
- Watts S, Stenner P. 2005. Doing Q methodology: theory, method and interpretation. Qual Res Psychol. 2:67–91.
- Watts S, Stenner P. 2012. Doing Q methodological research: theory, method and interpretation. London (UK): SAGE.
- Whitehead CR. 2016. On gunboats and grand pianos: medical education exports and the long shadow of colonialism. Adv Health Sci Educ. 21:1–4.
- Wilkins S, Huisman J. 2012. The international branch campus as transnational strategy in higher education. High Educ. 64:627–645.