

Abstract
A systematic review of studies published between 1 January 1985 and 31 August 2017 was performed to analyse the efficacy of the low-molecular-weight heparin, dalteparin, in venous thromboembolism (VTE) treatment and prophylaxis during pregnancy, and to evaluate dosing practices, anticoagulant monitoring and adverse events. A therapeutic dosing throughout pregnancy or followed by reduced doses effectively prevented VTE recurrence. Anti-factor Xa activity was the most commonly used method of dose monitoring. The risk of bleeding with dalteparin was generally minor. Major bleeding was observed when a high dose of dalteparin was employed during (or close to) delivery, or postpartum. Other adverse events were minor. Disparity exists in VTE treatment and thromboprophylaxis, with wide variety in the dosing regimens, treatment strategies and monitoring practices employed. Large randomised controlled trials are warranted but due to ethical reasons, and the rarity of VTE-associated obstetric complications, case-control, registry and large observational studies present more likely options.
Introduction
During pregnancy and the postpartum period, women are at increased risk of venous thromboembolism (VTE) – a collective term for deep vein thrombosis (DVT) and pulmonary embolism (PE). Obstetric VTE is one of the major causes of maternal death and morbidity in Western countries (Marik and Plante Citation2008; Chunilal and Bates Citation2009) and complicates approximately one in 1000 pregnancies (Lindqvist et al. Citation1999; Heit et al. Citation2005; James et al. Citation2006; Jacobsen et al. Citation2008b), with equal occurrence during pregnancy and the postpartum period. There is a known association with risk factors such as personal or family history of VTE, an older age, thrombophilia, immobilisation, surgery, a high body mass index, smoking, nulliparity, cancer and obstetric complications such as placental abruption, heavy bleeding at delivery and pre-eclampsia (Lindqvist et al. Citation1999; Jacobsen et al. Citation2008a; Royal College of Obstetricians and Gynaecologists Citation2015).
During pregnancy, the risk of VTE is increased at least fivefold compared with age-matched non-pregnant women, while the relative risk in the postpartum period can be as high as 60-fold (Pomp et al. Citation2008). Ovarian hyperstimulation in relation to in vitro fertilisation is reported to have a 100-fold risk for VTE during the first trimester (Rova et al. Citation2012). The increased risk of VTE during pregnancy in women with severe thrombophilia, such as an acquired thrombophilia or hereditary deficiency in antithrombin, protein C or protein S, is reported to vary between 10% and approximately 50% (Swedish Society of Obstetrics and Gynecology (SFOG) and Working Group on Hemostatic Disorders (Hem-ARG) Citation2012; Royal College of Obstetricians and Gynaecologists Citation2015; James et al. Citation2017). The upper bound of this range (i.e. very high risk) concerns women with antithrombin deficiency type I and previous VTE (James et al. Citation2017). As these risk factors can be identified before and during pregnancy, thromboprophylaxis is important and can prevent fatal maternal complications. Women with a history of VTE have a three to four times higher risk of recurrent VTE during a subsequent pregnancy compared with during their non-pregnant periods (James et al. Citation2017). In general, women with unprovoked VTE have a higher recurrence rate than women with pregnancy-induced VTE. However, during pregnancy the risk of a recurrence is higher following pregnancy-induced VTE (Lindqvist et al. Citation2011). An absolute recurrence risk of VTE – which is ∼5‒10% during pregnancy – is reported when no thromboprophylaxis is provided () (Lindqvist et al. Citation2011).
Table 1. Recurrence of VTE in women without thromboprophylaxis during pregnancy and postpartum (adapted from Lindqvist et al. Citation2011. Acta Obstet Gynecol Scand 90:648–653, ©2011 Nordic Federation of Societies of Obstetrics and Gynecology, with permission from Wiley).
As heparins do not exhibit a placental passage, they are the drug of choice for the treatment and prophylaxis of VTE during pregnancy. Low-molecular-weight heparins (LMWH) offer advantages over unfractionated heparins (UFH), allowing mostly once-daily dosing in non-pregnant patients, a lower risk of heparin-induced thrombocytopenia (HIT) and osteoporosis, and an improved clinical benefit with respect to the efficacy and risk of bleeding (Greer and Nelson-Piercy Citation2005; Bates et al. Citation2012; Royal College of Obstetricians and Gynaecologists Citation2015).
LMWH, including dalteparin, have a reduced effect on plasma clotting time compared with UFH, as measured by the activated partial thromboplastin time. Furthermore, dalteparin exerts a smaller effect on platelet function and lipolysis than heparin and is less sensitive to neutralising components in blood (Electronic Medicines Compendium (eMC) Citation2016). These factors result in a more predictable dose–response and a decreased need for monitoring in non-pregnant individuals (Antman Citation2001).
Many current treatment guidelines – including those from Sweden (Swedish Society of Obstetrics and Gynecology (SFOG) and Working Group on Hemostatic Disorders (Hem-ARG) Citation2012), Great Britain (Royal College of Obstetricians and Gynaecologists Citation2015) and the USA (James and Committee on Practice Bulletins—Obstetrics Citation2011) recommend the use of LMWH over UFH for both the acute treatment of VTE and thromboprophylaxis in pregnancy. In the absence of randomised controlled trials (RCTs) in pregnant women, experience garnered from non-pregnant patients has been used as a basis for therapeutic planning for the pregnant patient. Published studies concerning treatment of VTE and thromboprophylaxis during pregnancy and postpartum mostly comprise a small number of participants, except for a minimal number of systematic reviews. Moreover, decisions regarding the treatment of VTE and thromboprophylaxis during pregnancy are not currently standardised among physicians, centres or countries. Current clinical practice guidelines provide varying recommendations for dosing regimens during acute-phase treatment and for long-term treatment and prophylaxis. There is also heterogeneity in guidance for the monitoring of anticoagulant effect of LMWHs. This effect can be determined by different analyses including thrombin generation, overall haemostasis potential and anti-factor Xa (anti-FXa) activity (Schambeck et al. Citation2001; Antovic et al. Citation2002; al Dieri et al. Citation2004; Harris et al. Citation2011), with the latter method being most frequently used in clinical practice.
The objective of this review was to analyse the efficacy of dalteparin in the treatment and prophylaxis of VTE in obstetric patients. The decision to study dalteparin only was made because of the absence of a comprehensive review concerning this LMWH in an obstetric population. While generally accepted as a single type of anticoagulant, differences in biochemical properties exist between LMWHs, which could be important for efficacy, dosing and drug elimination (Gerotziafas et al. Citation2007). Furthermore, it complements previously reported studies of the LMWHs enoxaparin and tinzaparin in this population (Lepercq et al. Citation2001; Nelson-Piercy et al. Citation2011). The secondary objectives were to analyse the dosing practices, the recommended measurements of determination of anticoagulant effects, and the adverse events associated with the treatment of VTE and thromboprophylaxis using dalteparin.
Materials and methods
Information sources and search strategy
A PICO framework was employed to determine the search strategy for the study and to extract data. The PICO is presented in . Relevant studies for this review were identified by an electronic literature search using Embase, MEDLINE PubMed and Cochrane Library databases. In addition, ClinicalTrials.gov was searched for ongoing studies. Searches covered published medical literature between 1 January 1985 and 31 August 2017. The search strategies with combined terms relating to [dalteparin] AND [pregnancy] followed by venous thromboembolism, deep vein thrombosis, deep venous thrombosis, PE, venous thromboses and venous thrombosis are shown in . The authors ensured that duplicate records following the database searches were removed. The language was restricted to Swedish and English. There were no restrictions placed on the study design.
Table 2. PICO framework for treatment and thromboprophylaxis.
Table 3. Search strategies for electronic databases
Eligibility criteria
The authors reviewed studies in which dalteparin was administered to pregnant women for VTE prophylaxis and treatment. The studies that were included focussed on dalteparin, pregnancy, VTE prophylaxis and treatment, and the occurrence or recurrence of VTE () with a primary outcome measure of VTE recurrence. Studies limited to investigation of adverse events, pregnancy loss, obstetric complications including placenta-mediated complications, duration of labour and coagulation parameters as outcomes, without reporting recurrences of VTE, were excluded. Studies were also excluded if they focussed on dalteparin administration following only a caesarean section or postpartum, case reports, or where fewer than five pregnant women were reported as study subjects. Finally, studies with dalteparin in combination with acetylsalicylic acid were excluded as the objective of this review was to study the efficacy of dalteparin, only.
Table 4. Characteristics of included studies.
Table 5. Risk of bias, directness and precision according to the Swedish Agency for Health Technology Assessment and Assessment of Social Services, Citation2017.
Study selection and quality assessment
Both authors independently screened the title and abstract of identified citations for potential eligibility in an unblinded manner. Full-text articles judged as potentially eligible by at least one author were then retrieved and independently screened by both authors. In case of discrepancies, a consensus was reached following discussion. The two authors independently identified trials fulfilling the inclusion criteria, assessed risk of bias and extracted data from all included trials. Data were extracted regarding the author, year of publication, location, study design, study duration, number of participants, type of intervention (and, if available, control group), mean age, anti-FXa monitoring and the outcomes ().
The risk of bias within the individual articles was evaluated using validated checklists for RCTs and observational studies from The Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) (Swedish Agency for Health Technology Assessment and Assessment of Social Services Citation2017) and modified by the Health Technology Agency, Sahlgrenska University Hospital, Gothenburg, Sweden (). The appraisal addressed directness (external validity), risk of bias (internal validity) and precision that are presented at three levels: low, moderate and high. The studies’ risk of bias was independently assessed by both authors. In reaching a decision, the appropriateness of randomisation and allocation, blinding, outcome reporting and description of withdrawals, as well as any other biases considered to be relevant, were evaluated.
Results
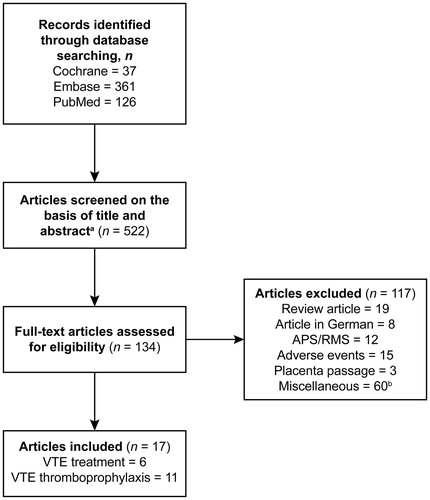
The electronic search strategy identified 522 articles, of which 134 were considered potentially eligible following a screen of the title and abstract. The full-text screen of the 134 citations identified 17 eligible articles according to the predetermined inclusion/exclusion criteria and included a total of 2144 women who were administered dalteparin. Search results are summarised in . The included studies are present in . The quality of studies was generally low as most were retrospective or small prospective cohort studies or case series. Since only one small RCT was included, we were unable to perform meta-analyses and instead provide a qualitative assessment of the studies and their results ().
Figure 1. Overview of electronic literature search. APS, antiphospholipid syndrome; RMS, recurrent miscarriage syndrome; VTE, venous thromboembolism. aDuplicate records following database searches were removed. bArticles excluded as described under eligibility criteria.
Efficacy
The incidence of recurrence of VTE either during pregnancy or postpartum is present in . Treatment of VTE using dalteparin was reported in one retrospective study (Revelj et al. Citation2015) and five prospective studies (Ulander et al. Citation2002; Jacobsen et al. Citation2003; Barbour et al. Citation2004; Voke et al. Citation2007; Knight and UKOSS Citation2008). Of the 174 women treated with dalteparin, one (0.6% [95% confidence interval: 0.01–3.16]) recurrence of VTE was reported during pregnancy (Ulander et al. Citation2002) and one (0.6% [0.01–3.16]) was reported postpartum (Revelj et al. Citation2015). Eleven studies were identified that examined the effect of dalteparin in the prophylaxis of VTE in pregnancy (Wahlberg and Kher Citation1994; Hunt et al. Citation1997; Blombäck et al. Citation1998; Pettilä et al. Citation1999; Bombeli et al. Citation2001; Schambeck et al. Citation2001; Antovic et al. Citation2002; Bauersachs et al. Citation2007; Lindqvist et al. Citation2011; Schoenbeck et al. Citation2011; Björgvinsdottir et al. Citation2013). Thromboprophylaxis was administered to 1970 women during pregnancy and postpartum. Seven (0.4% [0.14–0.73]) antenatal and eight (0.4% [0.18–0.80]) postpartum recurrences of VTE were reported in three studies (Bauersachs et al. Citation2007; Lindqvist et al. Citation2011; Björgvinsdottir et al. Citation2013). In another study, five (2.7%) recurrences were reported in 184 women mostly receiving low doses of dalteparin (2500 U per 24 h) (Wahlberg and Kher Citation1994).
Table 6. Recurrence of VTE in patients who received dalteparin for treatment or thromboprophylaxis during pregnancy.
Dosing
A summary of the dosing regimens employed in eligible studies is shown in . A wide range of dalteparin doses was used, reflecting differences in indication (treatment or prophylaxis), risk factors, body weight, duration of pregnancy and analyses of anti-FXa. In most studies where specifics were provided, the treatment ceased with the onset of labour and was resumed after delivery. Most patients continued initially on dalteparin for the postpartum period in accordance with the dosage received during pregnancy, followed by dalteparin alone, or switched to Vitamin K antagonists during treatment with dalteparin. In general, the duration of postpartum anticoagulation was 6 weeks for thromboprophylaxis and 6 weeks to 12 months following the treatment of VTE during pregnancy.
Table 7. Summary of dosing regimens in VTE treatment and prophylaxis ante- and postpartum, target anti-FXa levels and dose adjustments
Of the 17 studies included in this review, 15 reported target anti-FXa activity as a method of monitoring dalteparin dose or at least in selected cases (Wahlberg and Kher Citation1994; Hunt et al. Citation1997; Blombäck et al. Citation1998; Pettilä et al. Citation1999; Schambeck et al. Citation2001; Antovic et al. Citation2002; Ulander et al. Citation2002; Jacobsen et al. Citation2003; Barbour et al. Citation2004; Bauersachs et al. Citation2007; Voke et al. Citation2007; Lindqvist et al. Citation2011; Schoenbeck et al. Citation2011; Björgvinsdottir et al. Citation2013; Revelj et al. Citation2015) (). Most frequently, the target anti-FXa range was 0.6–1.0 IU/mL 3–4 h post-injection when used as a treatment for VTE and ∼0.2–0.4 IU/mL when used for prophylaxis (). One included study adjusted the dose according to body weight (Knight and UKOSS Citation2008), two used mainly fixed doses (Wahlberg and Kher Citation1994; Schoenbeck et al. Citation2011) and one study adjusted the dose according to thrombin-antithrombin complex and D-dimers (Bombeli et al. Citation2001).
Adverse events
All except three studies (Schambeck et al. Citation2001; Antovic et al. Citation2002; Knight and UKOSS Citation2008) of treatment and thromboprophylaxis provided information on the adverse event profile of dalteparin for both the mother and child. It is noteworthy that the studies used different regimens to monitor safety, and the safety data were presented in various ways ().
Table 8. Summary of adverse events in patients administered dalteparin
Bleeding and haematoma
Bleeding during pregnancy was reported in 13 studies (Wahlberg and Kher Citation1994; Hunt et al. Citation1997; Blombäck et al. Citation1998; Pettilä et al. Citation1999; Bombeli et al. Citation2001; Ulander et al. Citation2002; Jacobsen et al. Citation2003; Bauersachs et al. Citation2007; Voke et al. Citation2007; Lindqvist et al. Citation2011; Schoenbeck et al. Citation2011; Björgvinsdottir et al. Citation2013; Revelj et al. Citation2015) and appeared to be a risk that was dependent on dosing regimen. The bleeding was generally mild, but major bleeding was observed when a high dose of dalteparin was employed during, or close to, delivery.
Thrombocytopenia and HIT
No cases of HIT were identified. In a comparison of dalteparin versus UFH, one of 50 patients treated with dalteparin and three of 55 patients treated with UFH had a platelet count <150 × 109/L (Pettilä et al. Citation1999). No study reported patients with thrombocytopenia <100 × 109/L.
Allergy and local skin reaction
Pain, bruising, haematoma and allergic reactions were noted. While most were mild reactions, six (0.3%) women discontinued dalteparin prematurely owing to allergic reactions, two of which were considered to be severe (Bombeli et al. Citation2001; Revelj et al. Citation2015), and received an alternative LMWH (Bombeli et al. Citation2001; Schoenbeck et al. Citation2011; Revelj et al. Citation2015).
Osteoporosis and osteopenia
In total, three fractures were reported (Hunt et al. Citation1997; Blombäck et al. Citation1998; Bauersachs et al. Citation2007); a decrease in bone mineral density was noted in one study (Pettilä et al. Citation1999).
Pregnancy-associated adverse events and pregnancy outcome
Eight (0.6%) intrauterine deaths were reported (Wahlberg and Kher Citation1994; Hunt et al Citation1997; Blombäck et al. Citation1998; Jacobsen et al. Citation2003; Björgvinsdottir et al. Citation2013; Revelj et al. Citation2015). Four cases of placental abruption were reported in three studies, with an average incidence of 1% (Schoenbeck et al. Citation2011; Björgvinsdottir et al. Citation2013; Revelj et al. Citation2015). While prematurity was reported in some studies, there was no indication that rates of this or other pregnancy-associated complications were increased owing to dalteparin exposure ().
Discussion
This systematic review shows a good efficacy of dalteparin with a low risk of recurrences of VTE when used for treatment and prophylaxis during pregnancy and postpartum. In addition, we found varying dosing practices and recommendations for determination of anticoagulant effects. Adverse events were infrequent and as expected, based on studies concerning alternative LMWHs administered during pregnancy and postpartum. Obstetric adverse events could not be attributed to the treatment or thromboprophylaxis with dalteparin.
Given the ethical issues and stringent regulations surrounding the enrolment of pregnant women into clinical trials, RCTs conducted during pregnancy are very rare and generally small. We identified only one RCT that was eligible for inclusion in this review; however, this study was not optimal as the control group was treated with UFH. In addition, a placebo-controlled RCT concerning the prevention of placenta-mediated complications through administration of dalteparin was identified (Rodger et al. Citation2014). We decided not to include this study since the primary aim was not to report the benefit of thromboprophylaxis in preventing VTE but was a composite result. The subgroup of women with previous thromboembolic complications was also small. The remaining studies included in this review are retrospective studies, small prospective cohort studies or small to large case series. Future RCTs of appropriate power are needed to determine the most appropriate treatment and thromboprophylaxis against VTE during pregnancy and postpartum.
Current guidelines for the treatment of acute obstetric VTE generally recommend that anticoagulation is maintained at full dose for the duration of pregnancy (Bates et al. Citation2016). The Swedish guidelines advocate a less aggressive strategy, with 4–6 weeks of intensive treatment followed by reduced doses until delivery, based on twice-daily dosing and anti-FXa monitoring of anticoagulant effect. This approach has recently been suggested in a small systematic review of intermediate doses for the treatment of VTE during pregnancy (Gándara et al. Citation2014), which included four studies, one with, and three without, anti-FXa analyses. The present systematic review expands on the experience of the Swedish regime and confirms that reduced doses of dalteparin can be successful after initial therapeutic treatment (Revelj et al. Citation2015). Similar results have been reported following therapeutic treatment with other LMWHs throughout pregnancy (Romualdi et al. Citation2013). Results from our review of dalteparin also add to the body of evidence showing that thromboprophylaxis decreases the risk of VTE recurrence in at-risk pregnant women, as previously reported for other LMWHs (Lepercq et al. Citation2001; Greer and Nelson-Piercy Citation2005; Nelson-Piercy et al. Citation2011; Bates et al. Citation2016).
A variety of dalteparin dosing strategies are employed in pregnant women with acute VTE. The physiological changes that occur during pregnancy – weight gain, higher glomerular filtration and increased renal clearance of LMWH, and an increased plasma volume as pregnancy progresses, with simultaneous increase in volume of distribution – affect the pharmacokinetics of LMWH. These changes would be expected to increase the LMWH dose requirements in pregnant women in order to achieve an equal anticoagulant effect during all three trimesters (Sephton et al. Citation2003). Most reports support increasing LMWH dose as pregnancy progresses, and adjustments in LMWH dosing during pregnancy are recommended (Bates et al. Citation2012; Swedish Society of Obstetrics and Gynecology (SFOG) and Working Group on Hemostatic Disorders (Hem-ARG) Citation2012; Royal College of Obstetricians and Gynaecologists Citation2015). Most requirements for dose adjustments are reported where the anticoagulant effect of LMWH is monitored by analyses of anti-FXa (Wahlberg and Kher Citation1994; Hunt et al. Citation1997; Blombäck et al. Citation1998; Pettilä et al. Citation1999; Schambeck et al. Citation2001; Antovic et al. Citation2002; Ulander et al. Citation2002; Jacobsen et al. Citation2003; Barbour et al. Citation2004; Bauersachs et al. Citation2007; Voke et al. Citation2007; Lindqvist et al. Citation2011; Schoenbeck et al. Citation2011; Björgvinsdottir et al. Citation2013; Revelj et al. Citation2015; Boban et al. Citation2017).
A lower requirement for dose adjustments is noted when monitoring of anticoagulant effect is carried out according to body weight. Indeed, analyses of anti-FXa may represent a better method for dose determination, as weight gain during pregnancy can depend on multiple factors including oedema, polyhydramnios, large foetus and diet. A recent study compared the recurrence of VTE during treatment adjusted to anti-FXa activity with treatment without any adjustment, where therapeutic doses were determined according to body weight (McDonnell et al. Citation2017). There was no difference in recurrence of VTE between the two groups. However, the number of women in the treatment groups was very small: 14 and 16 for treatment with and without adjustment for anti-FXa activity, respectively, and the body weight at inclusion was not extreme. It is well known that analyses of anti-FXa can vary between different laboratories, and therefore a given individual should be monitored at the same laboratory to ensure that the same anticoagulant effect, anti-FXa activity, is achieved throughout pregnancy. Of the studies included in this review, there were very few VTE recurrences reported in total, and they did not appear to correlate with a specific dosing/monitoring regimen. The correlation between anti-FXa measurement and bleeding or thromboembolism has not been robustly demonstrated, but anti-FXa monitoring currently represents the most frequently used method for determining the anticoagulant effect of LMWH in clinical practice in pregnancy, as well as in patients with renal dysfunction and severe obesity. A study with combined analyses of anti-FXa activity and prothrombin fragment 1 + 2 has recently reported that this combination may improve the adjustment of LMWHs during pregnancy (Simeone et al. Citation2017).
When dalteparin is administered during pregnancy or postpartum, the potential for an increased risk of bleeding determined by the dose of dalteparin must be considered, and our results align with what has previously been reported for other LMWHs (Greer and Nelson-Piercy Citation2005; Nelson-Piercy et al. Citation2011). Furthermore, it is important to note that an increase in anticoagulant effect associated with a decrease in plasma volume postpartum occurs if the same dose is administered before and after delivery. A dose adjustment following delivery can be recommended. In the current review, the risk of bleeding with dalteparin was generally minor and appeared to be less of a concern than with UFH (Pettilä et al. Citation1999; Bates et al. Citation2012).
There is no evidence that the administration of dalteparin during pregnancy significantly increases the risk of HIT to a greater extent than in comparative studies of non-pregnant individuals. In pregnancy, thrombocytopenia in general and HIT – a condition with life- and limb-threatening thrombotic complications – must be considered separately. Thrombocytopenia as low as 70–80 × 109/L without other symptoms (benign thrombocytopenia, up to 7% of all pregnancies) can be found in late pregnancy without any complications (Townsley Citation2013).
Allergy and local skin reaction following dalteparin administration were reported in approximately 2–3% of patients and consisted mostly of itching and redness. Serious reactions, affecting six patients, prompted a change in anticoagulant. However, this figure does not exceed that expected for LMWHs (Wütschert et al. Citation1999; Schultinge et al. Citation2013; Electronic Medicines Compendium (eMC) Citation2016).
The studies included in this review reported three osteoporotic fractures (three per 1000 patients), but such fractures can also occur during pregnancy in the absence of LMWH or heparin (Sanz-Salvador et al. Citation2015). Osteoporosis after a long-term administration of dalteparin cannot be excluded, although a small, randomised but underpowered study previously reported no effect on bone mass (Rodger et al. Citation2007). Conversely, a study that followed approximately 100 pregnant women treated with dalteparin found diminished bone density in about 30% of the women, but no fractures (Alexandersson et al. Citation2001). During that study, a proportion of the women had measurements taken during more than one pregnancy, and results showed that the bone mass was generally unchanged between pregnancies. Repeated treatment with LMWH did not consistently impair bone density. The risk of bone loss in pregnant women is lower in those treated with dalteparin compared with those treated with UFH and may be comparable to the predicted pregnancy-induced bone loss as demonstrated in non-anticoagulant-treated patients (Rodger et al. Citation2007).
Although intrauterine death and prematurity were reported in some studies, they were most likely caused by underlying maternal disease. Four cases of placental abruption were reported from three studies, with an average incidence of 1%. However, this incidence does not exceed that expected in pregnant women who are not receiving anticoagulants (Ananth et al. Citation2015). Thus, there was no indication that the rate of pregnancy-associated complications was increased by dalteparin use. The pregnancy outcome results so far do not reveal any obvious safety concerns when dalteparin is administered throughout pregnancy, as might be expected because of the inability of dalteparin to pass the placenta. Similar positive obstetric outcomes have been previously reported concerning other LMWHs (Lepercq et al. Citation2001; Greer and Nelson-Piercy Citation2005; Nelson-Piercy et al. Citation2011).
To our knowledge, there are no studies on the health economics of treatment of obstetric VTE, a subject that warrants investigation. Two health-economic studies investigating thromboprophylaxis postpartum show the cost-effectiveness of treating women prophylactically: one following risk score assessment, and the other reporting cost-effectiveness in high-risk patients (Johnston et al. Citation2005; Lindqvist et al. Citation2008).
Conclusions
In conclusion, thromboprophylaxis in ‘at-risk’ pregnant women and treatment of VTE with dalteparin resulted in a low risk of VTE recurrence. The reported adverse events were minor, and there was no evidence of a significantly increased risk of HIT, allergy, local reactions or osteoporosis. Furthermore, there was no indication that dalteparin increases the risk for specific pregnancy complications affecting mother and/or child. Our findings show that disparity exists in the way that VTE in pregnancy is treated and how thromboprophylaxis is managed in clinical practice, with variety in the dosing regimens, treatment strategies and monitoring practices employed. Large, randomised controlled trials are warranted, but due to ethical reasons, and the rarity of VTE-associated obstetric complications, case-control, registry and large observational studies present more likely options of expanding knowledge within the field. In addition, the cost-effectiveness of treatment and prophylactic therapy has not been sufficiently examined. In the absence of such studies, an analytic model to compare efficacy and cost-effectiveness is warranted.
Acknowledgements
The authors would like to thank Ingrid Edsman of Edmedica and Therese Svanberg, librarian, Sahlgrenska University Hospital, Gothenburg for conducting the literature searches that formed the basis of this article.
Disclosure statement
Margareta Hellgren has received research support, lecture honoraria and consultancy fees from CSL Behring, Leo Pharma, Octapharma Nordica and Pfizer AB, Sweden. Oras Mistafa is an employee of Pfizer AB, Sweden.
Additional information
Funding
References
- al Dieri R, Alban S, Béguin S, Hemker HC. 2004. Thrombin generation for the control of heparin treatment, comparison with the activated partial thromboplastin time. Journal of Thrombosis and Haemostasis 2:1395–1401.
- Alexandersson M, Mellström D, Hellgren M. 2001. Bone density after long term thromboprophylaxis or treatment with dalteparin (Fragmin) during pregnancy [abstract]. 18th International Society on Thrombosis and Haemostasis, 2001 Jul 6–12; Paris, France.
- Ananth CV, Keyes KM, Hamilton A, Gissler M, Wu C, Liu S, et al. 2015. An international contrast of rates of placental abruption: an age-period-cohort analysis. PLoS One 10:e0125246.
- Antman EM. 2001. The search for replacements for unfractionated heparin. Circulation 103:2310–2314.
- Antovic A, Blombäck M, Bremme K, He S. 2002. The assay of overall haemostasis potential used to monitor the low molecular mass (weight) heparin, dalteparin, treatment in pregnant women with previous thromboembolism. Blood Coagulation & Fibrinolysis. 13:181–186.
- Badaracco MA, Vessey MP. 1974. Recurrence of venous thromboembolic disease and use of oral contraceptives. British Medical Journal 1:215–217.
- Barbour LA, Oja JL, Schultz LK. 2004. A prospective trial that demonstrates that dalteparin requirements increase in pregnancy to maintain therapeutic levels of anticoagulation. American Journal of Obstetrics and Gynecology 191:1024–1029.
- Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. 2012. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 141:e691S–e736S.
- Bates SM, Middeldorp S, Rodger M, James AH, Greer I. 2016. Guidance for the treatment and prevention of obstetric-associated venous thromboembolism. Journal of Thrombosis and Thrombolysis 41:92–128.
- Bauersachs RM, Dudenhausen J, Faridi A, Fischer T, Fung S, Geisen U, et al. 2007. Risk stratification and heparin prophylaxis to prevent venous thromboembolism in pregnant women. Thrombosis and Haemostasis 98:1237–1245.
- Björgvinsdottir A, Sporrong T, Hagman A, Hellgren M. 2013. Obstetric thromboprophylaxis in women with high to very-high risk for venous thromboembolism during pregnancy [abstract]. Thrombosis Research S87–S88.
- Blombäck M, Bremme K, Hellgren M, Siegbahn A, Lindberg H. 1998. Thromboprophylaxis with low molecular mass heparin, 'Fragmin' (dalteparin), during pregnancy – a longitudinal safety study. Blood Coagulation & Fibrinolysis: An International Journal in Haemostasis and Thrombosis 9:1–9.
- Boban A, Paulus S, Lambert C, Hermans C. 2017. The value and impact of anti-Xa activity monitoring for prophylactic dose adjustment of low-molecular-weight heparin during pregnancy: a retrospective study. Blood Coagulation & Fibrinolysis: An International Journal in Haemostasis and Thrombosis 28:199–204.
- Bombeli T, Raddatz Mueller P, Fehr J. 2001. Evaluation of an optimal dose of low-molecular-weight heparin for thromboprophylaxis in pregnant women at risk of thrombosis using coagulation activation markers. Haemostasis 31:90–98.
- Brill-Edwards P, Ginsberg JS, Gent M, Hirsh J, Burrows R, Kearon C, et al. 2000. Safety of withholding heparin in pregnant women with a history of venous thromboembolism. Recurrence of clot in This pregnancy study group. New England Journal of Medicine 343:1439–1444.
- Chunilal SD, Bates SM. 2009. Venous thromboembolism in pregnancy: diagnosis, management and prevention. Thrombosis and Haemostasis 101:428–438.
- De Stefano V, Martinelli I, Rossi E, Battaglioli T, Za T, Mannuccio Mannucci P, et al. 2006. The risk of recurrent venous thromboembolism in pregnancy and puerperium without antithrombotic prophylaxis. British Journal of Haematology 135:386–391.
- Electronic Medicines Compendium (eMC). 2016. Fragmin 5000 IU [summary of product characteristics]. Sandwich, UK: Pfizer Limited; [cited 2016 Aug 19]. Available from: https://www.medicines.org.uk/emc/medicine/26896.
- Gándara E, Carrier M, Rodger MA. 2014. Intermediate doses of low-molecular-weight heparin for the long-term treatment of pregnancy thromboembolism. A systematic review. Thrombosis and Haemostasis 111:559–561.
- Gerotziafas GT, Petropoulou AD, Verdy E, Samama MM, Elamy I. 2007. Effect of the anti-factorXa and anti-factor IIa activities of low-molecular-weight-heparins upon the phases thrombin generation. Journal of Thrombosis and Haemostasis 5:955–962.
- Greer IA, Nelson-Piercy C. 2005. Low-molecular-weight heparins for thromboprophylaxis and treatment of venous thromboembolism in pregnancy: a systematic review of safety and efficacy. Blood 106:401–407.
- Harris LF, Castro-López V, Jenkins PV, O'Donnell JS, Killard AJ. 2011. Comparison of a fluorogenic anti-FXa assay with a central laboratory chromogenic anti-FXa assay for measuring LMWH activity in patient plasmas. Thrombosis Research 128:e125–e129.
- Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ. 2005. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Annals of Internal Medicine 143:697–706.
- Hunt BJ, Doughty HA, Majumdar G, Copplestone A, Kerslake S, Buchanan N, et al. 1997. Thromboprophylaxis with low molecular weight heparin (Fragmin) in high risk pregnancies. Thrombosis and Haemostasis 77:39–43.
- Jacobsen AF, Qvigstad E, Sandset PM. 2003. Low molecular weight heparin (dalteparin) for the treatment of venous thromboembolism in pregnancy. British Journal of Obstetrics and Gynaecology 110:139–144.
- Jacobsen AF, Skjeldestad FE, Sandset PM. 2008a. Ante- and postnatal risk factors of venous thrombosis: a hospital-based case-control study. Journal of Thrombosis and Haemostasis 6:905–912.
- Jacobsen AF, Skjeldestad FE, Sandset PM. 2008b. Incidence and risk patterns of venous thromboembolism in pregnancy and puerperium – a register-based case-control study. American Journal of Obstetrics and Gynecology 198: 233.e1237.
- James A. Committee on Practice Bulletins—Obstetrics. 2011. Practice bulletin no. 123: thromboembolism in pregnancy. Obstetrics and Gynecology 118:718–729.
- James AH, Bates SM, Bauer KA, Branch W, Mann K, Paidas M, et al. 2017. Management of hereditary antithrombin deficiency in pregnancy. Thrombosis Research 157:41–45.
- James AH, Jamison MG, Brancazio LR, Myers ER. 2006. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. American Journal of Obstetrics and Gynecology 194:1311–1315.
- Johnston JA, Brill-Edwards P, Ginsberg JS, Pauker SG, Eckman MH. 2005. Cost-effectiveness of prophylactic low molecular weight heparin in pregnant women with a prior history of venous thromboembolism. The American Journal of Medicine 118:503–514.
- Knight M. UKOSS. 2008. Antenatal pulmonary embolism: risk factors, management and outcomes. British Journal of Obstetrics and Gynaecology 115:453–461.
- Lepercq J, Conard J, Borel-Derlon A, Darmon JY, Boudignat O, Francoual C, et al. 2001. Venous thromboembolism during pregnancy: a retrospective study of enoxaparin safety in 624 pregnancies. British Journal of Obstetrics and Gynaecology 108:1134–1140.
- Lindqvist P, Dahlbäck B, Marŝál K. 1999. Thrombotic risk during pregnancy: a population study. Obstetrics and Gynecology 94:595–599.
- Lindqvist PG, Bremme K, Hellgren M. Working Group on Hemostatic Disorders (Hem-ARG), Swedish Society of Obstetrics and Gynecology. 2011. Efficacy of obstetric thromboprophylaxis and long-term risk of recurrence of venous thromboembolism. Acta Obstetricia et Gynecologica Scandinavica 90:648–653.
- Lindqvist PG, Torsson J, Almqvist A, Björgell O. 2008. Postpartum thromboembolism: severe events might be preventable using a new risk score model. Vascular Health and Risk Management 4:1081–1087.
- Marik PE, Plante LA. 2008. Venous thromboembolic disease and pregnancy. The New England Journal of Medicine 359:2025–2033.
- McDonnell BP, Glennon K, McTiernan A, O’Connor HD, Kirkham C, Kevane B, et al. 2017. Adjustment of therapeutic LMWH to achieve specific target anti-FXa activity does not affect outcomes in pregnant patients with venous thromboembolism. Journal of Thrombosis and Thrombolysis 43:105–111.
- Nelson-Piercy C, Powrie R, Borg JY, Rodger M, Talbot DJ, Stinson J, et al. 2011. Tinzaparin use in pregnancy: an international, retrospective study of the safety and efficacy profile. European Journal of Obstetrics, Gynecology, and Reproductive Biology 159:293–299.
- Pabinger I, Grafenhofer H, Kaider A, Kyrle PA, Quehenberger P, Mannhalter C, et al. 2005. Risk of pregnancy-associated recurrent venous thromboembolism in women with a history of venous thrombosis. Journal of Thrombosis Haemostasis 3:949–954.
- Pettilä V, Kaaja R, Leinonen P, Ekblad U, Kataja M, Ikkala E. 1999. Thromboprophylaxis with low molecular weight heparin (dalteparin) in pregnancy. Thrombosis Research 96:275–282.
- Pomp ER, Lenselink AM, Rosendaal FR, Doggen CJ. 2008. Pregnancy, the postpartum period and prothrombotic defects: risk of venous thrombosis in the MEGA study. Journal of Thrombosis and Haemostasis 6:632–637.
- Revelj M, Hagman A, Hellgren M. 2015. Recurrence of VTE, obstetric and neonatal outcomes in 78 women with venous thromboembolism during pregnancy and puerperium [abstract]. 6th International Symposium on Women's Health Issues in Thrombosis, 2015 Feb 13–15; Berlin, Germany.
- Rodger MA, Hague WM, Kingdom J, Kahn SR, Karovitch A, Sermer M, et al. 2014. Antepartum dalteparin versus no antepartum dalteparin for the prevention of pregnancy complications in pregnant women with thrombophilia (TIPPS): a multinational open-label randomised trial. Lancet 384:1673–1683.
- Rodger MA, Kahn SR, Cranney A, Hodsman A, Kovacs MJ, Clement AM, et al. 2007. Long-term dalteparin in pregnancy not associated with a decrease in bone mineral density: substudy of a randomized controlled trial. Journal of Thrombosis and Haemostasis 5:1600–1606.
- Romualdi E, Dentali F, Rancan E, Squizzato A, Steidl L, Middeldorp S, et al. 2013. Anticoagulant therapy for venous thromboembolism during pregnancy: a systematic review and a meta-analysis of the literature. Journal of Thrombosis and Haemostasis 11:270–281.
- Rova K, Passmark H, Lindqvist PG. 2012. Venous thromboembolism in relation to in vitro fertilization: an approach to determining the incidence and increase in risk in successful cycles. Fertility and Sterility 97:95–100.
- Royal College of Obstetricians and Gynaecologists. 2015. Reducing the risk of venous thromboembolism during pregnancy and the puerperium, Green-top Guideline No. 37a. London, UK: Royal College of Obstetricians and Gynaecologists; [cited 2016 Aug 31]. Available from: https://www.rcog.org.uk/globalassets/documents/guidelines/gtg-37a.pdf
- Royal College of Obstetricians and Gynaecologists. 2015. Thromboembolic disease in pregnancy and the puerperium: acute management, Green-top Guideline No. 37b. London, UK: Royal College of Obstetricians and Gynaecologists; [cited 2016 Aug 31]. Available from: https://www.rcog.org.uk/globalassets/documents/guidelines/gtg-37b.pdf
- Sanz-Salvador L, García-Pérez MÁ, Tarín JJ, Cano A. 2015. Bone metabolic changes during pregnancy: a period of vulnerability to osteoporosis and fracture. European Journal of Endocrinology/European Federation of Endocrine Societies 172:R53–R65.
- Schambeck CM, Eberl E, Geisen U, Grossmann R, Keller F. 2001. The impact of dalteparin (Fragmin) on thrombin generation in pregnant women with venous thromboembolism: significance of the factor V Leiden mutation. Thrombosis and Haemostasis 85:782–786.
- Schoenbeck D, Nicolle A, Newbegin K, Hanley J, Loughney AD. 2011. The use of a scoring system to guide thromboprophylaxis in a high-risk pregnant population. Thrombosis 2011:652796.
- Schultinge L, Knol HM, Kluin-Nelemans HC, Erwich JJ, Meijer K. 2013. Incidence of hypersensitivity skin reactions in patients on full-dose low-molecular-weight heparins during pregnancy. The Netherlands Journal of Medicine 71:518–522.
- Sephton V, Farquharson RG, Topping J, Quenby SM, Cowan C, Back DJ, et al. 2003. A longitudinal study of maternal dose response to low molecular weight heparin in pregnancy. Obstetrics and Gynecology 101:1307–1311.
- Simeone R, Giacomello R, Bruno G, Parco S, Maximova N, Martinelli M, et al. 2017. Thrombogenesis in thrombophilic pregnancy: evaluation of low-molecular-weight heparin prophylaxis. Acta Haematologica 137:201–206.
- Swedish Agency for Health Technology Assessment and Assessment of Social Services. 2017. Stockholm, Sweden; [cited 2017 Dec 7]. Available from: http://www.sbu.se/en/About-SBU/
- Swedish Society of Obstetrics and Gynecology (SFOG), Working Group on Hemostatic Disorders (Hem-ARG). 2012. Hemostasrubbningar inom obstetrik och gynekologi [Nr 68]. Olovsson M, editor. Stockholm, Sweden. SFOG.
- Tengborn L, Bergqvist D, Matzsch T, Bergqvist A, Hedner U. 1989. Recurrent thromboembolism in pregnancy and puerperium. Is there a need for thromboprophylaxis?. American Journal of Obstetrics and Gynecology 160:90–94.
- Townsley DM. 2013. Hematologic complications of pregnancy. Seminars in Hematology 50:222–231.
- Ulander VM, Stenqvist P, Kaaja R. 2002. Treatment of deep venous thrombosis with low-molecular-weight heparin during pregnancy. Thrombosis Research 106:13–17.
- Voke J, Keidan J, Pavord S, Spencer NH, Hunt BJ. British Society for Haematology Obstetric Haematology Group. 2007. The management of antenatal venous thromboembolism in the UK and Ireland: a prospective multicentre observational survey. British Journal of Haematology 139:545–558.
- Wahlberg TB, Kher A. 1994. Low molecular weight heparin as thromboprophylaxis in pregnancy. A retrospective analysis from 14 European clinics. Haemostasis 24:55–56.
- Wütschert R, Piletta P, Bounameaux H. 1999. Adverse skin reactions to low molecular weight heparins: frequency, management and prevention. Drug Safety 20:515–525.