

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
To evaluate the effect of hysteroscopy and suture on uterine scar diverticulum (CSD) after caesarean section and its influence on blood loss, operation time and antibiotic time. Eighty-nine patients with CSD were divided into observation group (n = 41 cases) and control group (n = 48 cases). Control group received laparoscopic scar diverticulum resection and suture, while the observation group received hysteroscopic resection of scar diverticulum. The operation time of the observation group was longer, while the bleeding volume and antibiotic administration time were significantly lower. The surgical treatment efficiency of the observation group (97.56%) was significantly higher. After treatment, the observation group’s diverticulum repair indexes (width, depth and lower uterine muscular layer thickness) were better than those of the control group (p<.05). Hysteroscopic resection of scar diverticulum in CSD reduces intraoperative blood loss and the risk of complications, shortens time of antibiotic administration, and promotes diverticulum repair.
What is already known on this subject? Uterine scar diverticulum (CSD) after caesarean section, also called postoperative uterine incision defect (PCSD), is due to poor healing of the uterine incision after caesarean section.
What do the results of this study add? Hysteroscopic resection of scar diverticulum in CSD has a significant clinical effect, which can effectively reduce intraoperative blood loss and the risk of complications, shorten the time of antibiotic administration, and promote diverticulum repair.
What are the implications of these findings for clinical practice and/or further research? Clinical effect of hysteroscopic resection of scar diverticulum in CSD is significant.
Impact Statement
Introduction
Uterine scar diverticulum (CSD) after caesarean section, also called postoperative uterine incision defect (PCSD), is caused by poor healing of the uterine incision after caesarean section, manifested as thinning of the muscle layer at the incision of the uterine scar. The depression or cavity in communication with the uterine cavity will then cause abnormal vaginal bleeding, pelvic pain and other related clinical symptoms (Minovi et al. Citation2015; Zhao et al. Citation2019). Uterine diverticulum is divided into congenital and acquired diverticulum. Congenital diverticulum is related to abnormal embryonic development. Acquired diverticulum is also called false diverticulum. Uterine incision diverticulum after caesarean section is an acquired diverticulum. In recent years, with the increase of caesarean section, acquired uterine diverticulum has gradually increased. Patients with uterine diverticulum often present with prolonged menstrual period, inexhaustible vaginal bleeding, and pregnancy in the diverticulum. Its treatment included drugs and surgery. At present, there is no unified understanding of the effects of various treatment methods, and a unified treatment standard has not been formed. This study intends to investigate the role of transvaginal CSD electro resection and suture guided by hysteroscopy in the treatment of CSD.
Methods
General information
Eighty-nine patients with CSD treated in our hospital from March 2012 to November 2019 were selected to perform different operations based on the principle of voluntariness. They were divided into an observation group (n = 41 cases) and a control group (n = 48 cases). Patients were diagnosed with CSD according to the diagnostic criteria: (1) patients with a history of caesarean section surgery and clinical manifestations such as prolonged menstrual period and infertility; (2) transvaginal ultrasound examination shows that there is a cystic, wedge-shaped or triangular liquid dark area in the uterine cavity at the caesarean section incision; (3) preoperative vaginal mycoplasma, chlamydia, gonococcus and bacterial cultures were negative; (4) patients with the caesarean history, the symptoms of menstrual period extension and secondary infertility. Inclusion criteria: (1) meet the above-mentioned CSD diagnostic criteria; (2) meet the surgical indications and have a history of caesarean section; (3) the patient signed an informed consent form. Exclusion criteria: (1) clinical symptoms caused by other gynaecological diseases such as uterine fibroids, adenomyosis; (2) acute systemic or local severe infection; (3) women who have no history of other uterine surgery or are in menstruation. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study is approved by the Ethics Committee of The First People’s Hospital of Foshan. Written informed consent was obtained. Informed consent was obtained from all individual participants included in the study.
Treatment
In both groups, patients were guided to take the position of bladder lithotomy and were given general anaesthesia for tracheal intubation. Laparoscopic electro resection and suture were performed in the control group. Transect vaginal mucosa along the bladder and groyne, inject normal saline at the junction of vagina and cervix, separate the vaginal and cervix space layer by layer, and then enter the lower part of uterus after careful exploration by laparoscope. Needle probe the scar of caesarean section incision, locate the diverticulum point, cut the diverticulum, remove the surrounding scar tissue, sew muscle layer with absorbable thread, sew vaginal wall with 1/0 absorbable thread, and insert drainage tube. Complete the operation. The observation group were treated with hysteroscopic electro resection of scar diverticulum (). The operation was as follows: a longitudinal incision of about 10 mm was made at the umbilicus, an artificial pneumoperitoneum was established, the abdominal pressure was maintained at about 13 mmHg, a laparoscope was inserted, and the bladder and scar adhesions were explored and loosened. Place the cervix with a hysteroscope to observe the depression of the incision in the lower uterus. After fully exposing the lesion site, locate the scar diverticulum range and upper and lower poles; use a probe to push out the boundary and fold the weakened mucosa of the diverticulum under laparoscopic instructions cut off and give electrocoagulation to stop bleeding. Hysteroscope was used to carefully explore again to ensure that the repair of the uterine incision diverticulum was completed. 3-0 absorbable thread was used to suture the diverticula until the diverticulum disappeared. The bladder and the uterus were sutured with inverted mattress to complete the myometrial suture. Both groups were given prophylactic antibiotics, and the drainage tube was removed 24–48 hours later.
Observation indicators
Perioperative treatment indicators, including the amount of bleeding, the operation time, the time of antibiotic medication (including the time of postoperative preventive medication and infectious medication) were compared. The postoperative curative effect of the two groups was compared. Postoperative curative effect evaluation criteria included cure: CSD-related clinical symptoms such as abnormal vaginal bleeding and pelvic pain disappeared; improvement: CSD-related clinical symptoms such as abnormal vaginal bleeding and pelvic pain were improved; invalid: clinical symptoms such as abnormal vaginal bleeding and pelvic pain related to CSD remained unchanged. The two groups of diverticulum repair indexes, including the width and depth of the diverticulum before and after treatment and the thickness of the lower uterine myometrium measured by contrast-enhanced uterine ultrasound were compared.
Statistical analysis
The data of CSD patients were included in the SPSS 23.0 software (SPSS Inc., Chicago, IL) for analysis. The measurement data were compared using t-test, and () was used to indicate the treatment index and diverticulum repair index. The count data used χ2 test, and the rate (%) was used to indicate the postoperative curative effect and complications. The risk rate (p < .05) is statistically different.
Results
Comparison of general data
The observation group was 25–36 years old (29.37 ± 1.25) years old, while the number of caesarean sections was 1–3 times (1.75 ± 0.27). The control group was 26–35 years old (29.68 ± 1.13) years old, while the number of caesarean sections was 1–3 times (1.77 ± 0.24) times. There was no statistical difference in general information of CSD patients between the two groups (p > .05).
Comparison of related treatment indicators in the perioperative period between the two groups
The operation time of the observation group was longer than that of the control group, while the bleeding volume and antibiotic administration time were significantly lower than those of the control group (p < .05) (, ).
Figure 1. Hysteroscopic excision and suture of scar diverticulum.
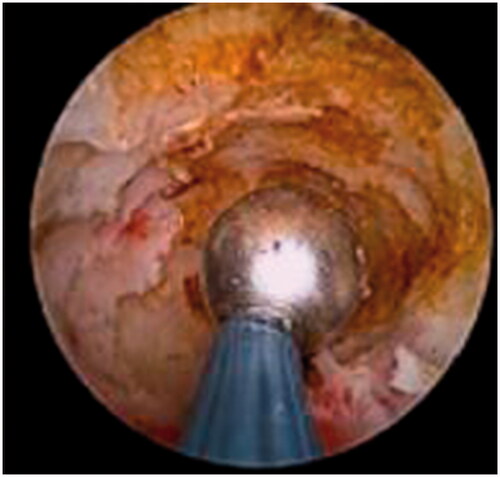
Table 1. Comparison of related treatment indicators in the perioperative period between the two groups ().
Comparison of the postoperative efficacy of the two groups
The surgical treatment efficiency of the observation group (97.56%) was significantly higher than that of the control group (85.42%) (χ2 = 3.986, p < .05) ().
Figure 2. Laparoscopic excision and suture of scar diverticulum.
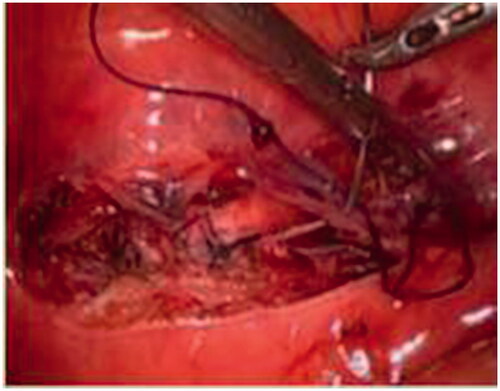
Table 2. Comparison of postoperative curative effect between the two groups (n (%)).
Comparison of repair indexes of two groups of diverticulum
There was no significant difference in the width and depth of the diverticulum and the thickness of the lower uterine muscular layer between the two groups before treatment (p > .05); after treatment, the observation group’s diverticulum repair indexes (width, depth and lower uterine muscular layer thickness) were significantly better than those of the control group (p < .05) ().
Table 3. Comparison of repair indexes of two groups of diverticulum (, mm).
Discussion
Due to the onset of drug treatment and adverse reactions, surgery can preserve normal muscle tissue, remove the scar diverticulum structure, and fundamentally solve the disease, surgical treatment is the main clinical method. Currently, hysteroscopy, hysteroscopy combined, vaginal surgery and minimally invasive surgery are the main surgical methods (Abacjew-Chmylko et al. Citation2017; Savilo et al. Citation2020; Zhu et al. Citation2020). Hysteroscopy combined treatment is based on the precise positioning of the diverticulum lesion site under the guidance of hysteroscope, the electro resection of the diverticulum wall under the guidance of laparoscopic, and the full-thickness suture of the diverticulum wall under the hysteroscope can effectively avoid poor suture or residual diverticulum. The wall leads to poor healing of diverticula (Urbina et al. Citation2019; Redman et al. Citation2020). At present, the theoretical and practical research of clinical hysteroscopy combined surgery is gradually increasing, but the indicators and influence of combined treatment need to be further improved. Therefore, this study will analyse the clinical effect of hysteroscopic electro resection of scar diverticulum in CSD and its influence on blood loss, operation time and antibiotic use time.
CSD is a long-term complication of caesarean section. With the development and progress of clinical diagnosis technology and disease awareness, the detection rate of this disease is getting higher and higher. CSD has severely affected the quality of life of patients, and increased the risk of adverse outcomes in patients with re-pregnancy. Therefore, it is necessary to strengthen the diagnosis and treatment of CSD (Zhou et al. Citation2016; Zou et al. Citation2020). The aetiology of CSD is not yet clear, and it is mainly believed to be closely related to the location of the incision of the caesarean section, the method of suture of the incision, the number of operations, and infection factors. Too close sutures leads to significant reduction in blood supply and bleeding of the incision, tissue ischaemic necrosis, which in turn affects the quality of healing, and single-layer sutures are more prone to incision defects. The more frequent of caesarean sections is, the higher risk of scar formation is. Uterine defects are often located at the site of infection. Infection can easily cause damage to the lower part of the uterus. Surgical treatment has the advantages of radical, rapid and convenient treatment, by removing or cauterising abnormal mucosal tissue in the diverticula, it can meet the needs of patients for symptom improvement and fertility, and is widely used in clinical treatment. At present, hysteroscopy and hysteroscopy combined with minimally invasive surgery are mainly used in clinical practice, but the specific clinical impact of hysteroscopy combined with hysteroscopy needs to be further studied.
Vaginal surgery is based on vaginal scar removal, which can avoid abdominal tissues and reduce the damage and impact on abdominal organs. However, due to the higher vaginal conditions of the patient and the smaller visual field, it is susceptible to uterine and pelvic adhesions and pelvic infections. The risk is extremely high (He et al. Citation2020). Hysteroscopic laparoscopic surgery combines the advantages of hysteroscopy and laparoscopy. Hysteroscopic surgery is based on hysteroscope-guided incision of the inferior wall tissue of the diverticulum that obstructs the flow of menstrual blood, and the use of electrocoagulation to destroy the intima. At the same time, it can play a diagnostic value in the operation. However, using it alone cannot avoid the risk of complications such as uterine perforation and bladder injury (Tulandi and Cohen Citation2016). Combined with laparoscopic surgery, the field of view is wider, the pelvic and abdominal cavity is fully explored, the adhesion tissue is separated, the bladder tissue is fully exposed, and the diverticulum tissue is accurately positioned based on the hysteroscope-guided light transmission experiment to ensure the full electro resection of the diverticulum fibrous tissue. Laparoscopic intermittent and continuous suture of the defective tissue is performed to completely repair the diverticulum. Laparoscopy is used to explore again to observe whether the sutured scar tissue is flat, which can reduce the stimulation of the wound to the pelvic and abdominal cavity, and reduce the probability of pelvic adhesions and recurrence (Chai et al. Citation2018; Khawcharoenporn and Kanoktipakorn Citation2021). It can not only effectively alleviate the patient’s clinical symptoms, but can also safely repair the narrow part without destroying the continuous muscular tissue of the lesion site, reducing the risk of uterine rupture in the second pregnancy, and then reducing the risk of perioperative infection. Compared with pure hysteroscopic surgery, this surgery can repair and strengthen the uterine scar muscle layer, and at the same time has a certain effect of correcting the uterine inclination (Ferrandina et al. Citation2016; Casadio et al. Citation2021).
The results of this study showed that the operation time of the observation group was longer than that of the control group, while the bleeding volume and antibiotic administration time were significantly lower than that of the control group. In order to reduce the risk of postoperative infection, perioperative preventive antibiotics have become a clinical consensus, but with the frequent occurrence of antibiotic abuse and misuse, antibiotic resistance events have also increased significantly. Therefore, the clinic advocates the rational use of antibiotics for preventive medication. Vaginal surgery has a large field of vision, and there are many adhesions between the lower part of the uterus and the bladder and peritoneum. There are separation gaps, and the suture operation is difficult, which causes greater trauma and pain. Laparoscopy combined with hysteroscopy and laparoscopic electro resection and suture can accurately locate the tissues and explore the adhesion of surrounding tissues to reduce the risk of active bleeding. At the same time, the operation under direct vision can ensure the safety of the operation and reduce the bladder, urethra, etc. The risk of damage to surrounding tissues reduces the risk of postoperative incision exposure and infection, and then reduces the use of preventive antibiotics, the toxicity and drug resistance caused by long-term antibiotics use. But at the same time, the operation time is prolonged due to the precise positioning operation (Takahashi et al. Citation2019). The surgical treatment efficiency of the observation group (97.56%) was significantly higher than that of the control group (85.42%). The reason is that vaginal surgery requires the bladder to be fully pushed open, the risk of bladder injury is high, and the surgical field of view is relatively difficult to expose. The positioning of the diverticulum mainly depends on the experience of the operator, and the positioning is not accurate enough. The combined hysteroscopy and laparoscopic electro resection and suture are based on the direct view of the diverticulum under a clear field of vision to accurately guide the treatment of the scar to ensure the integrity of the scar resection and the alignment and suture. There was no significant difference of the width and depth of the diverticulum and the thickness of the lower uterine muscular layer between the two groups before treatment (p > .05). After treatment, the observation group’s diverticulum repair indexes (width, depth and lower uterine muscular layer thickness) were significantly better than those of the control group (p < .05). The reason is that hysteroscopic electro resection of scar diverticulum can repair the diverticulum on the basis of preserving the integrity of the uterine scar, ensuring the integrity of the lesion tissue resection. Accurate suture and reinforcement can prevent the recurrence of the diverticulum and improve the effect of diverticulum repair.
Scar diverticulum may be coming a problem with increasing caesarean section rates in case of surgery fertility sparing treatments and robotic surgery (Gullo et al. Citation2021). For the women wishing to conceive, it is be much accounted (Cavaliere et al. Citation2021; Gullo et al. Citation2022). With the aim to improve the surgical outcomes and reduce the length and complication rate of the transition process, even robotic surgery has been performed (Laganà et al. Citation2021). To preserve the intrauterine pregnancy, treatment on CSD is remarkable A previous study has reported a successful laparoscopic treatment of an extrauterine pregnancy with the prosecution of the intrauterine pregnancy up to the third trimester (Cucinella et al. Citation2021). Gynaecological diseases are often associated with high stress and have a negative impact on quality of life and psychological well-being of women affected (La Rosa et al. Citation2018). The psychological impact depends on the level of severity of the disorder and on how much the symptoms interfere with occupational and social activities (La Rosa et al. Citation2018). The effect of hysteroscopy and suture treatment in the psychology needs to be further investigated. The main limitation of this study is that the sample size of this study is relatively small and the there is no randomisation in this study. Further study with strict design is needed.
In summary, the clinical effect of hysteroscopic electro resection of scar diverticulum in CSD is significant, which can effectively reduce intraoperative blood loss and the risk of complications, shorten the time of antibiotic administration, and promote diverticulum repair, which is worthy of clinical promotion.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study is approved by the Ethics Committee of The First People’s Hospital of Foshan. Written informed consent was obtained.
Consent form
Informed consent was obtained from all individual participants included in the study.
Author contributions
Guarantor of integrity of the entire study: Weifeng Li; study concepts: Weifeng Li; study design: Weifeng Li; definition of intellectual content: Tiecheng Lin and Yong Xie; literature research: Weifeng Li; clinical studies: Tiecheng Lin and Yong Xie; experimental studies: Weifeng Li, Tiecheng Lin and Yong Xie; data acquisition: Pei Cheng and Chunxiang Duan; data analysis: Lijiang Xu, Yangping Chen, Yuyuan Zhu and Xia Dong; statistical analysis: Lijiang Xu, Yangping Chen, Yuyuan Zhu and Xia Dong; manuscript preparation: Weifeng Li, Lijiang Xu, Yangping Chen, Yuyuan Zhu and Xia Dong; manuscript editing: Weifeng Li; manuscript review: Tiecheng Lin and Yong Xie.
Disclosure statement
None.
Data availability statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
References
- Abacjew-Chmylko A, Wydra DG, Olszewska H. 2017. Hysteroscopy in the treatment of uterine cesarean section scar diverticulum: a systematic review. Advances in Medical Sciences 62:230–239.
- Casadio P, Ambrosio M, Verrelli L, Salucci P, Arena A, Seracchioli R. 2021. Conservative cesarean scar pregnancy treatment: local methotrexate injection followed by hysteroscopic removal with hysteroscopic tissue removal system. Fertility and Sterility 116:1417–1419.
- Cavaliere AF, Perelli F, Zaami S, D’Indinosante M, Turrini I, Giusti M, et al. 2021. Fertility sparing treatments in endometrial cancer patients: the potential role of the new molecular classification. International Journal of Molecular Sciences 22:12248.
- Chai ZY, Zhang SS, Hu XH, Liu MM, Qi F. 2018. Successful resection of an 11-week cesarean scar pregnancy with a combination of laparoscopy and hysteroscopy. Journal of Minimally Invasive Gynecology 25:320–321.
- Cucinella G, Gullo G, Etrusco A, Dolce E, Culmone S, Buzzaccarini G. 2021. Early diagnosis and surgical management of heterotopic pregnancy allows us to save the intrauterine pregnancy. Przeglad Menopauzalny = Menopause Review 20:222–225.
- Ferrandina G, Palluzzi E, Fanfani F, Gentileschi S, Valentini AL, Mattoli MV, et al. 2016. Endometriosis-associated clear cell carcinoma arising in caesarean section scar: a case report and review of the literature. World Journal of Surgical Oncology 14:300.
- Gullo G, Etrusco A, Cucinella G, Perino A, Chiantera V, Laganà AS, et al. 2021. Fertility-sparing approach in women affected by stage I and low-grade endometrial carcinoma: an updated overview. International Journal of Molecular Sciences 22:11825.
- Gullo G, Etrusco A, Fabio M, Cucinella G, Rossi C, Billone V. 2022. The reproductive potential of uterus transplantation: future prospects. Acta Bio-Medica: Atenei Parmensis 93:e2022138.
- He Y, Zhong J, Zhou W, Zeng S, Li H, Yang H, et al. 2020. Four surgical strategies for the treatment of cesarean scar defect: a systematic review and network meta-analysis. Journal of Minimally Invasive Gynecology 27:593–602.
- Khawcharoenporn T, Kanoktipakorn P. 2021. Effectiveness of appropriate antibiotic prophylaxis for transurethral resection of the prostate in the era of antibiotic resistance. Infection Control & Hospital Epidemiology 15:1–5.
- La Rosa VL, Lucia V, Valenti G, Sapia F, Gullo G, Rapisarda A. 2018. Psychological impact of gynecological diseases: the importance of a multidisciplinary approach. Italian Journal of Gynaecology and Obstetrics 30:23–26.
- Laganà AS, Garzon S, Raffaelli R, Gullo G, Franchi M. 2021. Robotic surgery in female-to-male transition: a possible way for further improvement. Journal of Investigative Surgery 34:651–652.
- Minovi CM, Minovi A, Dost P. 2015. Suture of the mucosa after the endoscopic LASER mucomyotomy of Zenker’s diverticulum. European Archives of Oto-Rhino-Laryngology 272:2947–2952.
- Redman EP, Mishra PR, Stringer MD. 2020. Laparoscopic diverticulectomy or laparoscopic-assisted resection of symptomatic Meckel diverticulum in children? A systematic review. Pediatric Surgery International 36:869–874.
- Savilo CE, Smith RB, Mourad J. 2020. Robotic resection and revision of uterine scar defect with hysteroscopic guidance. Journal of Minimally Invasive Gynecology 27:S89.
- Takahashi A, Kimura F, Tsuji S, Yamanaka A, Takashima A, Takebayashi A, Murakami T. 2019. 1514 impact of hysteroscopic surgical management of cesarean scar syndrome on pregnancy rate: a prospective observational study. Journal of Minimally Invasive Gynecology 26:S203.
- Tulandi T, Cohen A. 2016. Emerging manifestations of cesarean scar defect in reproductive-aged women. Journal of Minimally Invasive Gynecology 23:893–902.
- Urbina P, Wu CZ, Vargas MV. 2019. Laparoscopic-assisted hysteroscopic resection of cesarean scar ectopic. Journal of Minimally Invasive Gynecology 26:S2.
- Zhao W, Yang Q, Zhang N, Wang Y, Wang G, Wang D. 2019. An effective assisted method using hysteroscopy transmittance test and a Foley catheter to repair previous cesarean scar defect by laparoscopy. Journal of Minimally Invasive Gynecology 26:605–606.
- Zhou J, Yao M, Wang H, Tan W, Chen P, Wang X. 2016. Vaginal repair of cesarean section scar diverticula that resulted in improved postoperative menstruation. Journal of Minimally Invasive Gynecology 23:969–978.
- Zhu Q, He X, Jiang L, Liang G, Zhu C, Pan H, et al. 2020. Effectiveness of hysteroscopic resection of a uterine caesarean niche can be predicted: a prospective cohort study. Scientific Reports 10:17424.
- Zou Z, Xiao S, Xue M. 2020. Clinical analysis of the preoperative condition and operative prognosis of post-cesarean section scar diverticulum: a case series. Journal of Perinatal Medicine 48:803–810.