

Introduction
Tamoxifen (TAM), as a traditional endocrine therapy drug, has reduced the local recurrence and mortality of breast cancer in receptor-positive patients (Early Breast Cancer Trialists’ Collaborative Group Citation1998). However, TAM may cause a series of adverse effects on the endometrium, such as atrophy, polyps, hyperplasia and cancer (Kloos et al. Citation2002). UCS (Uterine carcinosarcoma) is a relatively rare malignancy, accounting for less than 5% of all uterine tumours. However, it is highly malignant, accounting for 15% of all deaths caused by malignant tumours of the uterine corpus (Pezzicoli et al. Citation2021). We report for the first time a rare case of HER2 amplified UCS in a HER2-negative breast cancer patient treated with TAM.
Case presentation
A 53-year-old, menopausal, non-obese woman was admitted to the hospital with irregular vaginal bleeding for 6 months. The patient had no family history of malignancy and had not previously undergone pelvic radiotherapy. The patient was diagnosed with pT2N1M0 ER (+), PR (±), and HER2 (–) breast cancer 8 years ago and subsequently underwent protective and radical mastectomy and adjuvant radiotherapy and chemotherapy. She was recommended to receive endocrine therapy with TAM 20 mg/day for at least 5 years, but stopped taking it after 2 years. Computed tomography (CT) indicated endometrial thickening with a high possibility of malignant tumours (). No elevation in tumour markers, serum CA125, or HE4. The pathological section of the scrapings from the external cavity showed uterine carcinosarcoma: the carcinoma component was approximately 40%, a grade II endometrioid adenocarcinoma with squamous metaplasia, the sarcoma component was approximately 60%, and a high-grade endometrial mesenchymal sarcoma (). She underwent extra fascial hysterectomy, bilateral adnexal resection, retroperitoneal lymph node dissection, and the release of pelvic adhesions. Postoperative pathology showed that the tumour did not invade the myometrium, no bilateral ovarian invasion, or lymph node metastasis (). The patient was diagnosed with stage IA UCS.
Figure 1. (A) initial diagnosis. (B and C) Haematoxylin and eosin staining of the primary tumour revealed endometrioid adenocarcinoma with squamous metaplasia (magnification ×200) and high grade endometrial mesenchymal sarcoma (magnification ×200). (D) formalin-fixed resected specimen. (E) Recurrence of abdominal and extensive pelvic metastases. (F) The bowel is dilated and an air-liquid plane can be seen, suggesting intestinal obstruction. (G and H) Two months after six cycles of chemotherapy and targeted anti-angiogenic therapy, the patient was found to have liver and lung metastases.
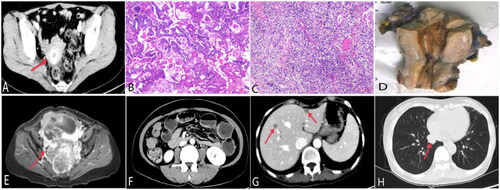
The patient did not undergo postoperative adjuvant radiotherapy or chemotherapy. She was readmitted 6 months later with abdominal pain and difficulty in defaecation. CT suggested recurrence of postoperative uterine cancer sarcoma, multiple metastases in the pelvis () and intestinal obstruction due to the recurrent tumour (). The patient underwent palliative resection and postoperatively received 6 cycles of bevacizumab + albumin-conjugated paclitaxel + carboplatin chemotherapy. About two months after the end of adjuvant therapy, the patient developed progressive disease (PD) with liver and lung metastases (). To identify potential therapeutic opportunities, we performed next-generation sequencing (NGS) of the metastatic mesenteric mass. The results showed that the HER2 gene was amplified approximately 5.7 times. The patient received trastuzumab + doxorubicin liposomes in second line, and discontinued after three cycles of treatment with oral ulcers and severe peeling of the hands. She has died at 20 months from diagnosis of UCS.
Discussion
Are uterine malignancies exposed to TAM more malignant? In a case-control study from the US, UK, and the Netherlands, patients with endometrial cancer treated with TAM for 5 years had a higher risk of death from endometrial cancer than those not treated with TAM. This could be attributed to the poorer prognosis of the endometrioid tissue subtype with long-term TAM (Jones et al. Citation2012). A multicenter retrospective study by Matsuo et al. showed that patients with TAM-related UCS were older, had a higher proportion of early stage and a lower risk of distant metastases than those with TAM-unrelated UCS, but there was no significant difference in survival outcomes between the two (Matsuo et al. Citation2017).
The incidence of HER2 overexpression/amplification in UCS ranges from 9% to 32%(Rottmann et al. Citation2020; Moukarzel et al. Citation2021). It is mostly detected in the epithelial component of the UCS and is independent of the co-expression of EGFR and KIT (Sawada et al. Citation2003). However, no significant correlation was observed between HER2 overexpression/amplification and patient prognosis (Raspollini et al. Citation2005).
There is a lack of data on anti-HER2-targeted therapies related to HER2 amplification in UCS patients. Nicoletti et al. found that trastuzumab-emtansine (T-DM1) was superior to trastuzumab in inhibiting the proliferation of ovarian and uterine cancer sarcoma cells, that the tumours in mice injected with T-DM1 largely resolved, and that the survival rate of mice was higher than that in the trastuzumab-injected group (Nicoletti et al. Citation2015).
Many studies have confirmed an increased risk of UCS in breast cancer patients treated with TAM. The molecular mechanism of UCS secondary to TAM treatment is unclear, and is a direction worthy of future research. NGS testing for UCS is used to identify potentially mutated genes, and may help improve treatment decisions to increase patient survival.
Ethical approval
Ethics committee approval was unnecessary due to the nature of the study. Written informed consent was obtained from the patient.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Early Breast Cancer Trialists’ Collaborative Group. 1998. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet 351:1451–1467.
- Jones ME, Van Leeuwen FE, Hoogendoorn WE, Mourits MJ, Hollema H, Van Boven H, et al. 2012. Endometrial cancer survival after breast cancer in relation to tamoxifen treatment: pooled results from three countries. Breast Cancer Research 14:R91.
- Kloos I, Delaloge S, Pautier P, Di Palma M, Goupil A, Duvillard P, et al. 2002. Tamoxifen-related uterine carcinosarcomas occur under/after prolonged treatment: report of five cases and review of the literature. International Journal of Gynecological Cancer 12:496–500.
- Matsuo K, Ross MS, Bush SH, Yunokawa M, Blake EA, Takano T, et al. 2017. Tumor characteristics and survival outcomes of women with tamoxifen-related uterine carcinosarcoma. Gynecologic Oncology 144:329–335.
- Moukarzel LA, Ferrando L, Da Cruz Paula A, Brown DN, Geyer FC, Pareja F, et al. 2021. The genetic landscape of metaplastic breast cancers and uterine carcinosarcomas. Molecular Oncology 15:1024–1039.
- Nicoletti R, Lopez S, Bellone S, Cocco E, Schwab CL, Black JD, et al. 2015. T-DM1, a novel antibody-drug conjugate, is highly effective against uterine and ovarian carcinosarcomas overexpressing HER2. Clinical and Experimental Metastasis 32:29–38.
- Pezzicoli G, Moscaritolo F, Silvestris E, Silvestris F, Cormio G, Porta C, D’oronzo S. 2021. Uterine carcinosarcoma: an overview. Critical Reviews in Oncology/Hematology 163:103369.
- Raspollini MR, Susini T, Amunni G, Paglierani M, Taddei A, Marchionni M, et al. 2005. COX-2, c-KIT and HER-2/neu expression in uterine carcinosarcomas: prognostic factors or potential markers for targeted therapies? Gynecologic Oncology 96:159–167.
- Rottmann D, Snir OL, Wu X, Wong S, Hui P, Santin AD, Buza N. 2020. HER2 testing of gynecologic carcinosarcomas: tumor stratification for potential targeted therapy. Modern Pathology 33:118–127.
- Sawada M, Tsuda H, Kimura M, Okamoto S, Kita T, Kasamatsu T, et al. 2003. Different expression patterns of KIT, EGFR, and HER-2 (c-erbB-2) oncoproteins between epithelial and mesenchymal components in uterine carcinosarcoma. Cancer Science 94:986–991.