

Abstract
We evaluated the impact of cervical cerclage combined with one or more uterine contraction inhibitors in persistent inhibition of uterine contraction for the treatment of late abortion and premature delivery. This retrospective case series study analysed the medical data of 58 patients who underwent cervical cerclage for cervical insufficiency and simultaneously received one or more uterine contraction inhibitors (indomethacin, ritodrine, and atosiban) and magnesium sulphate at the Zibo Maternal and Child Health Hospital between January 2019 and December 2020. Patients are normal pregnancy who received cervical cerclage without complications. The rate of successful treatment was 74.14% (43/58). The prolonged gestation duration was 16.42 ± 7.84 weeks, and the average delivery gestational age was 35.91 ± 5.16 weeks. The longest duration of treatment with a uterine contraction inhibitor or inhibitors in combination or with magnesium sulphate alone was 15.34 ± 13.16 days, and nine cases developed adverse reactions. Persistent uterine contraction inhibition after cervical cerclage could prolong pregnancy and improve pregnancy outcomes.
What is already known on this subject? A crucial reason for treatment failure of cervical cerclage is that uterine contraction was not effectively inhibited.
What do the results of this study add? Persistent inhibition of uterine contraction after cervical cerclage prolonged pregnancy duration, increased gestational age at delivery, and improved pregnancy outcomes.
What are the implications of these findings for clinical practice and/or further research? This study may provide a clinical basis for prolonging gestational age, preventing late abortion and premature delivery, and improving the survival rate and quality of life of premature infants.
Impact statement
Introduction
Spontaneous abortion and premature delivery are major concerns for both obstetricians and pregnant women. Preterm birth affects approximately 10% of pregnancies (Pohl et al. Citation2018). The reasons for late abortion and premature deliveries could be multifactorial (Goldenberg et al. Citation2008). Cervical insufficiency is one of the causes of late abortion and premature delivery. A study has shown that acute cervical insufficiency accounts for 10–25% of all mid-trimester pregnancy losses (Park et al. Citation2021). Cervical cerclage was first performed to treat cervical insufficiency in 1955, and has subsequently become the most commonly performed surgical procedure to prolong the pregnancy time in patients with the loss and premature delivery of second pregnancy caused by cervical insufficiency. Zhu LQ et al. (Zhu et al. Citation2015) mentioned that cervical cerclage was a feasible choice to prolong the pregnancy. However, cervical cerclage of patients with uterine contractions may lead to abortion and premature delivery. Therefore, we retrospectively analysed the medical data at our hospital to examine the impact of persistent uterine contraction inhibition after cervical cerclage on late abortion and premature delivery.
Patients and methods
Study design and population
This retrospective case series study enrolled 58 patients who underwent cervical cerclage for cervical insufficiency and were treated with indomethacin, ritodrine, and atosiban alone, or in combination, or magnesium sulphate with indomethacin at the Zibo Maternal and Child Health Hospital between January 2019 and December 2020. 36.20% of the participant was history indicated and 63.80% was ultrasound indicated. Patients with complications that would impact their pregnancy were excluded from the study. Patients with normal pregnancy who received cervical cerclage without complications, such as persistent vaginal bleeding, premature rupture of membranes, foetal malformation or stillbirth, chorionic villitis, placenta previa, and placental abruption, were included in this study. Informed consent was obtained from all participants.
Cerclage procedure and post-operation
Shirodkar cervical cerclage was performed for all the patients. A Mersilk suture was U-shape around the cervix counterclockwise from 11 o’clock. The knot was at 12 o’clock. The patients whose amniotic sac was protruded out of the external orifice of the cervix was placed in a position that their heads lay low and their buttocks were held high. The amniotic sac was disinfected with iodophor and gently placed back into the internal orifice of the cervix by using a cotton ball. After cervical cerclage, antibiotics were administered for five days to prevent infection, and uterine contraction inhibitors (indomethacin, ritodrine, and atosiban) alone, in combination, or magnesium sulphate alone were administered. The type, dosage, and duration of uterine contraction inhibitor administration were determined according to the interval, intensity, and duration of uterine contractions. A cerclage is removed typically around the gestational age of 36–37 weeks. In the majority of our patients, the gestational age was ≥35 weeks with regular contractions or amniotic sac rupture when the cerclage was removed. However, in some patients, the cerclage was removed at the gestational age of <35 weeks when regular contractions were not effectively inhibited or amniotic sac was ruptured.
Clinical outcomes
Clinical data including age, gestational weeks, parity, foetal number, the weeks of termination of gestation, pregnancy latency, dilatation of cervix, cervical length, foetal sac, medication time, and adverse reactions were collected.
Statistical analysis
Statistical analysis was performed by SPSS, version 17 (IBM SPSS Inc., Armonk, NY, USA). Quantitative data were expressed as mean ± standard deviation (mean ± SD). Qualitative data were expressed in percentage (%). Pearson’s correlation analysis was performed and a p-value <.05 was considered statistically significant.
Results
Cervical cerclage was successfully performed in all 58 patients. The age of the patients ranged from 23 to 44 years, with an average age of 31.54 ± 4.54 years. The gestational age ranged from 12+6 to 26+6 weeks, with an average gestational age of 19.49 ± 4.70 weeks. The participants included 33 primipara and 25 multipara women. There were 49 singleton pregnancies and nine bigeminal or multiple pregnancies. The dilatation of cervix was <1 cm in 11 patients, between ≥1 and <2 cm in 36 patients, between ≥2 and <4 cm in nine patients, and ≥4 cm in two patients. The cervical length was between <2.5 and >2 cm in two patients, between ≤2 and >1 cm in 15 patients, and ≤1 cm in 41 patients. The clinical and demographic data of all patients are displayed in .
Figure 1. Flow diagram on participants flow in the study.
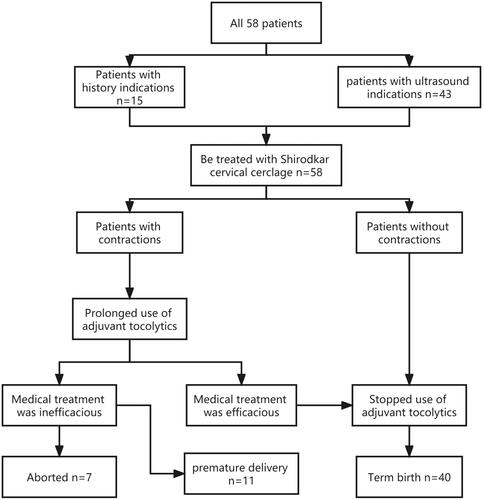
Table 1. Clinical and demographic data of the patients.
Pregnancy outcomes are presented in and . The cerclage was removed in 43 patients at a gestational age of 36–37 weeks, and the success rate was 74.14% (43/58). Seven patients delivered in <28 weeks, six delivered in 28–33+6 weeks, five delivered in 34–37 weeks, and 40 delivered in >37 weeks. Notably, there was a case of triplet pregnancy, two of which were spontaneously aborted. The average delivery gestational age was 35.91 ± 5.16 weeks. The gestational age was prolonged by 16.42 ± 7.84 weeks. The duration of medication (uterine contraction inhibitors or magnesium sulphate) was 15.34 ± 13.16 days. Fifty-four newborns survived and three newborns died because their parents did not continue the treatment. One newborn died because of premature rupture of membranes at 16+5 gestation weeks. There were six cases of neonatal respiratory distress syndrome. Gestational weeks at preterm deliveries ranged between 26 weeks and 4 days to 33 weeks and 2 days, and indication for delivery was foetal heart rate deceleration.
Table 2. Pregnancy outcomes.
As shown in , prolonged pregnancy latency was positively correlated with gestational age at delivery, p < .01 with a correlation coefficient pf 0.816, but negatively correlated with the longest duration of medication use, p < .01, with a correlation coefficient of 0.453.
Table 3. Correlation of prolonged gestational age with longest time of medication.
Table S1 shows the maternal adverse effects, which included nausea and vomiting (n = 2), headache (n = 1), hand tremor (n = 3), hypokalaemia (n = 2), and elevated serum amylase level (n = 1).
Discussion
It is 48 hours that several guidelines of preterm birth recommend duration of uterine contraction inhibition for treatment of preterm birth. However, the fact of clinic condition is not as same as description of guidelines. Clinically, we have to extend the duration of medication because of the disease. So we made the study and found use of uterine contraction inhibition more than 48 h could prolong pregnancy and improve pregnancy outcomes effectively.
In this study, the presence of regular uterine contractions was considered the primary reason for administering uterine contraction inhibitors. Furthermore, if uterine contractions are inhibited effectively but adverse reactions occur, it should be considered as the reason to reduce the dose of the inhibitors; replace these inhibitors with other medications/treatments; a combination of treatments should be used, or these drugs should be discontinued. We found that prolonged pregnancy latency could increase the gestational age of delivery (p < .01). Forty patients delivered after 37 weeks of gestation, which reduced the premature delivery rate. Prolonged gestational age was negatively correlated with the longest duration of medication (p < .01). The gestational age was not significantly prolonged in patients with duration of medication use, indicating the complexity of late abortion and premature delivery. The duration of the medication was increased because uterine contractions could not be effectively inhibited. Hence, abortion and premature birth could not be avoided. We considered that it was vital to administer persistent uterine contraction inhibitors at the same time when cervical cerclage was performed as it can prolong gestational age and reduce premature birth rate.
Neonatal outcomes are related to gestational age at delivery. Preterm birth leads to severe complications in newborns (Raia et al. Citation2020). Gestational age is a critical factor affecting the development of premature infants. The risk of mortality and morbidity of newborns is related to the gestational age (Zhang et al. Citation2020), which means the lower the gestational age, the higher the risk of mortality and morbidity (Yu et al. Citation2020). Neonatal survival rate can be increased by 3% for each delayed day at 22–26 weeks of gestation (Lamont et al. Citation2016)and reaches 90% when the gestational age is delayed to 30 weeks (Chen et al. Citation2014). Jiang ZD (Jiang and Chen Citation2014) and Liu et al. (Liu et al. Citation2013) reported that more than half of the surviving infants had varying degrees of physical disabilities. Premature infants are also at risk of underdeveloped cognitive abilities (Spittle et al. Citation2012). The gestational age of more than 34 weeks is a common milestone of foetal development and maturity. Obstetricians should therefore plan to prolong the gestational age, and improve the survival rate and quality of life of premature infants.
Liu et al. reported that both prophylactic cervical cerclage and therapeutic cervical cerclage distinctly extended the length of the pregnancy (Liu et al. Citation2018). Moreover, Li et al. concluded that cerclage placement could effectively reduce the incidence of preterm birth (Li et al. Citation2019). Vaginal cerclage can be used to treat cervical insufficiency. However, it can be ineffective in some cases (Joal et al. Citation2020). Tocolytic drugs are often used to postpone preterm delivery (Rovers et al. Citation2021). Both reasonable and in-time cervical cerclage and persistent uterine contraction inhibition are essential for effectively treating such patients. Therefore, we retrospectively analysed the medical data at our hospital and found that persistent uterine contraction inhibition after cervical cerclage could prolong gestational age. Cervical cerclage combined with persistent uterine contraction inhibition is an effective method for treating late pregnancy abortion and premature delivery caused by cervical insufficiency, and for prolonging the gestational age. This combined strategy of pregnancy management can reduce the number of preterm deliveries (Barinov et al. Citation2021).
A crucial reason for treatment failure is that uterine contraction was not effectively inhibited. Although most patients had no apparent uterine contractions before the surgery, patients had different degrees of uterine contractions after the surgery and required uterine contraction inhibitor administration accordingly because of the stimulation of the cervix and uterus. In this study, the gestational age was prolonged by 16.42 ± 7.84 weeks. The average delivery gestational age was 35.91 ± 5.16 weeks. The duration of the gestational age was positively correlated with the gestational age at delivery, p < .01. Tocolytics can delay delivery (Jørgensen et al. Citation2014). It is necessary to treat uterine contraction in order to prolong the pregnancy, achieve a higher birth weight, and reduce the associated morbidity and mortality (Carvajal et al. Citation2017). Additionally, it takes 4–7 days to produce lung surfactant after initial corticosteroid administration (Ballard et al. Citation1997). So, it is obviously important to restrain uterine contraction.
Clinical Diagnosis and Treatment Guidelines for Premature Delivery (2014) do not recommend continuous use of uterine contraction inhibitors and combination of two or more uterine contraction inhibitors after 48 h. In this study, the presence of regular uterine contractions was the primary reason for administering these inhibitors. Furthermore, if uterine contractions are inhibited effectively but adverse reactions occur, it should be considered as the standard to reduce the dose of uterine contraction inhibitors; replace the uterine contraction inhibitors with other medications/treatments; a combination of treatments should be used, or these drugs should be discontinued. The average duration of use of tocolytics was 15.34 + 13.16 days. We found that prolonged gestational age could increase the gestational age of delivery (p < .01). It is vital to administer persistent uterine contraction inhibitors at the same time when cervical cerclage is performed as it can prolong gestational age, reduce the premature birth rate, and improve neonatal survival rate and neonatal outcomes. Prolonged gestational age was negatively correlated with the longest duration of medication (p < .01). The gestational age was not significantly prolonged in patients with long medication time, indicating the complexity of late abortion and premature delivery. The duration of the medication was increased because uterine contraction could not be effectively inhibited. Hence, abortion and premature birth could not be avoided.
Limitation
This study was based on a small sample size. Therefore, the results may have limited generalisability.
Conclusions
In this study, persistent inhibition of uterine contraction after cervical cerclage prolonged pregnancy duration, increased gestational age at delivery, and improved pregnancy outcomes. This study may provide a clinical basis for prolonging gestational age, preventing late abortion and premature delivery, and improving the survival rate and quality of life of premature infants.
Ethical approval
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by Zibo Maternal and Child Health Care Hospital Medical Ethics Review Committee (202107063). This article is a retrospective study. Therefore the Institutional waived the requirement to obtain distinct written informed consent from the patients.
Author contributions
Lirong Zhao and Li Xiao carried out the studies, participated in collecting data, and drafted the manuscript. Lirong Zhao and Qing Liu performed the statistical analysis and participated in its design. Lirong Zhao, Shujing Lu and Yingchun Yu participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Supplemental Material
Download MS Word (15.8 KB)Acknowledgements
The authors would like to thank all the patients and their families who participated in the study. We also thank Li Xiao for her suggestions on the subject design.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
- Ballard PL, Ning Y, Polk D, Ikegami M, Jobe AH. 1997. Glucocorticoid regulation of surfactant components in immature lambs. The American Journal of Physiology 273:L1048–1057.
- Barinov SV, Artymuk NV, Novikova ON, Shamina IV, Tirskaya YI, Belinina AA, et al. 2021. Analysis of risk factors and predictors of pregnancy loss and strategies for the management of cervical insufficiency in pregnant women at a high risk of preterm birth. The Journal of Maternal-Fetal & Neonatal Medicine 34:2071–2079.
- Carvajal JA, Zambrano MJ, Theodor NM, Moreno LE, Olguín TR, Vanhauwaert PS, et al. 2017. The synergic in vitro tocolytic effect of nifedipine plus ritodrine on human myometrial contractility. Reproductive Sciences 24:635–640.
- Chen A-C, Chung M-Y, Chang JH, Lin H-C. 2014. Pathogenesis implication for necrotizing enterocolitis prevention in preterm very-low-birth-weight infants. Journal of Pediatric Gastroenterology and Nutrition 58:7–11.
- Goldenberg RL, Culhane JF, Iams JD, Romero R. 2008. Epidemiology and causes of preterm birth. The Lancet 371:75–84.
- Jiang ZD, Chen C. 2014. Impaired neural conduction in the auditory brainstem of high-risk very preterm infants. Clinical Neurophysiology 125:1231–1237.
- Joal A, Bouchet N, Martinez De Tejada B. 2020. MAVRIC study: when abdominal cerclage is preferable to vaginal cerclage. Revue Médicale Suisse 16:2026–2030.
- Jørgensen JS, Weile LK, Lamont RF. 2014. Preterm labor: current tocolytic options for the treatment of preterm labor. Expert Opinion on Pharmacotherapy 15:585–588.
- Lamont CD, Jørgensen JS, Lamont RF. 2016. The safety of tocolytics used for the inhibition of preterm labour. Expert Opinion on Drug Safety 15:1163–1173.
- Li C, Shen J, Hua K. 2019. Cerclage for women with twin pregnancies: a systematic review and metaanalysis. American Journal of Obstetrics and Gynecology 220:543–557.e541.
- Liu Y, Ke Z, Liao W, Chen H, Wei S, Lai X, et al. 2018. Pregnancy outcomes and superiorities of prophylactic cervical cerclage and therapeutic cervical cerclage in cervical insufficiency pregnant women. Archives of Gynecology and Obstetrics 297:1503–1508.
- Liu F, Zhao Q, Shao Y. 2013. Severe brain damage in premature infants associated with postnatal infection. Minerva Medicine 104:349–355.
- Park JY, Oh KJ, Lee S, Kim N-K, Lee Y-E, Park YH, et al. 2021. A new quantification system for assessing the degree of acute cervical insufficiency based on physical and sonographic examination. European Journal of Obstetrics & Gynecology and Reproductive Biology 256:372–378.
- Pohl O, Chollet A, Kim SH, Riaposova L, Spézia F, Gervais F, et al. 2018. OBE022, an oral and selective prostaglandin F(2)(α) receptor antagonist as an effective and safe modality for the treatment of preterm labor. The Journal of Pharmacology and Experimental Therapeutics 366: 349–364.
- Raia NR, Bakaysa SL, Ghezzi CE, House MD, Kaplan DL. 2020. Ex vivo pregnant-like tissue model to assess injectable hydrogel for preterm birth prevention. Journal of Biomedical Materials Research-Part B, Applied Biomaterials 108: 468–474.
- Rovers JF, Thomissen IJ, Janssen LC, Lingius S, Wieland BV, Dieleman JP, et al. 2021. The relationship between antenatal indomethacin as a tocolytic drug and neonatal outcomes: a retrospective cohort study. Journal of Maternal-Fetal and Neonatal Medicine 34: 2945–2951.
- Spittle A, Orton J, Anderson PJ, Boyd R, Doyle LW. 2012. Early developmental intervention programmes post-hospital discharge to prevent motor and cognitive impairments in preterm infants. Cochrane Database Systematic Review 12:CD005495.
- Yu Y, Yang Z, Wu L, Zhu Y, Guo F. 2020. Effectiveness and safety of atosiban versus conventional treatment in the management of preterm labor. Taiwanese Journal of Obstetrics and Gynecology 59: 682–685.
- Zhang Y, Raia N, Peterson A, Kaplan DL, House M. 2020. Injectable silk-based hydrogel as an alternative to cervical cerclage: a rabbit study. Tissue Engineering Part A 26: 379–386.
- Zhu LQ, Chen H, Chen LB, Liu YL, Tan JP, Wang YH, et al. 2015. Effects of emergency cervical cerclage on pregnancy outcome: a retrospective study of 158 cases. Medical Science Monitor 21:1395–1401.