

Abstract
This study evaluated the effect of intrauterine perfusion of autologous platelet-rich plasma (PRP) on pregnancy outcomes in women with recurrent implantation failure (RIF). Key biomedical databases were searched to identify relevant clinical trials and observational studies. Outcomes included clinical pregnancy rate, chemical pregnancy rate, implantation rate, live birth rate, and abortion rate. Data was extracted from ten studies (six randomised controlled trials, four cohort studies) involving 1555 patients. Pregnancy outcomes were improved in women treated with PRP compared to controls: clinical pregnancy rate (RR = 1.96, 95% CI [1.67, 2.31], p < 0.00001, I2 = 46%), chemical pregnancy rate (RR = 1.79, 95% CI [1.54, 2.08], p < 0.00001, I2 = 29%), implantation rate (RR = 1.90, CI [1.50, 2.41], p < 0.00001, I2 = 0%), live birth rate (RR = 2.83, CI [1.45, 5.52], p = 0.0007, I2 = 83%), abortion rate (RR = 0.40, 95% CI [0.18, 0.90], p = 0.03, I2 = 59%). These data imply PRP has potential to improve pregnancy outcomes in women with RIF, suggesting a promising role in assisted reproductive technology.
What is already known on this subject? Platelet-rich plasma (PRP) is an autologous blood product that contains platelets, various growth factors, and cytokines at concentrations above the normal baseline level. Recent studies have shown that intrauterine infusion of autologous PRP can improve pregnancy outcomes in infertile women.
What do the results of this study add? This systematic review and meta-analysis of data from ten studies (n = 1555; 775 cases and 780 controls) investigated the effect of intrauterine perfusion of autologous PRP on pregnancy outcomes in women with recurrent implantation failure (RIF). Findings suggest that pregnancy outcomes, including clinical pregnancy rate, chemical pregnancy rate, implantation rate, live birth rate and abortion rate were improved in women treated with PRP compared to controls.
What are the implications of these findings for clinical practice and/or further research? RIF remains a challenge for researchers, clinicians, and patients. Our study identified PRP as a potential intervention in assisted reproduction. As an autologous blood preparation, PRP eliminates the risk of an immune response and transmission of disease. PRP is low cost and effective and may represent a new approach to the treatment of patients with RIF.
IMPACT STATEMENT
Introduction
Despite advances in assisted reproductive technology (ART), recurrent implantation failure (RIF) remains a major challenge, affecting at least 10% of women who undergo in vitro fertilisation and embryo transfer (IVF-ET) (Somigliana et al. Citation2018, Busnelli et al. Citation2020). Although there is no consensus (Coughlan et al. Citation2014), the most widely accepted definition of RIF is ‘the failure to achieve a clinical pregnancy after the transfer of four good-quality embryos in a minimum of three fresh or frozen cycles to the normal uterine cavity’ (Cavalcante et al. Citation2020, Chen et al. Citation2020). The aetiology of RIF can be grouped into three categories, including decreased endometrial receptivity, embryonic defects, and immunological factors (Margalioth et al. Citation2006). There are numerous interventions and therapies for RIF. Recently, immunomodulatory therapies, including intravenous immunoglobulin (IVIG) administration, intrauterine peripheral blood mononuclear cell (PBMC) infusion, subcutaneous or intrauterine granulocyte colony stimulating factor (G-CSF) administration, intravenous intralipid administration, intrauterine human chorionic gonadotropin (hCG) injection, low-molecular-weight heparin (LMWH) administration and intrauterine autologous platelet-rich plasma (PRP) infusion, have received increasing attention (Busnelli et al. Citation2021).
In recent years, intrauterine infusion of autologous PRP has emerged as an immunotherapy for RIF (Marx Citation2001). Autologous PRP has a platelet concentration four to five times above baseline and contains abundant growth factors and cytokines, such as vascular endothelial growth factor (VEGF), transforming growth factor (TGF), platelet-derived growth factor (PDGF) and epidermal growth factor (EGF) (Christgau et al. Citation2006). Autologous PRP has been applied extensively in regenerative medicine, including orthopaedics, dermatology and aesthetic surgery (Whitney et al. Citation2017, Zhang et al. Citation2018, Samadi et al. Citation2019). Recent research implies that PRP may improve pregnancy outcomes in women with RIF by regulating endometrial cell migration, attachment, proliferation, differentiation, and neo-angiogenesis (Farimani et al. Citation2016, Dieamant et al. Citation2019), but these findings remain controversial. Urman et al. perceived that existing studies were insufficient to provide convincing evidence for the effectiveness of PRP for ART, and that more clinically relevant outcomes should be evaluated (Urman et al. Citation2019). A published meta-analysis evaluated the effect of PRP on pregnancy outcomes in women undergoing ART. In a subgroup analysis of women with RIF, PRP was associated with improved clinical pregnancy rates (CPR), but other pregnancy outcomes were not investigated (Maleki-Hajiagha et al. Citation2020). Consequently, there remains an unmet need to objectively evaluate the effectiveness of PRP in RIF.
The objective of this systematic review and meta-analysis was to evaluate the effect of intrauterine perfusion of autologous PRP on pregnancy outcomes in women with RIF. The present study extends previous reviews by including new studies. Findings may help clarify the therapeutic role of PRP in RIF.
Materials and methods
This study was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 Checklist (David et al.) (http://www.prisma-statement.org/). The protocol of the meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO, https://www.crd.york.ac.uk/PROSPERO/) with the registration number of PROSPERO CRD42020160798.
Search and selection strategy
Eight electronic databases, including the PubMed, Embase, Cochrane, Web of Science (WOS), Wan Fang, China National Knowledge Infrastructure, and VIP Science Technology Periodical databases, were systematically searched from 1 January 2000 to 13 August 2022 to identify studies in the English or Chinese language that investigated the impact of intrauterine perfusion of autologous PRP on pregnancy outcomes in women with RIF. Keywords included: ‘platelet-rich plasma’ or ‘PRP’ or ‘autologous platelet-plasma’, ‘repeated implantation failure’ or ‘recurrent implantation failure’ or ‘RIF’.
Inclusion criteria were: (1) study design: randomised controlled trials (RCTs) or cohort studies; (2) subjects: infertile women who had experienced at least three implantation failures; (3) intervention: intrauterine perfusion of PRP before ET; (4) outcomes: at least one of clinical pregnancy rate, chemical pregnancy rate, implantation rate, live birth rate or abortion rate. Exclusion criteria were: (1) animal or cell culture experiments; (2) single-arm or studies with a pre-post design; (3) case reports; or (4) conference abstracts.
After removing duplicates, two researchers (Deng, H. and Li, Z.) independently screened the titles and abstracts of retrieved articles and reviewed the full-text of eligible studies. Disagreements were resolved by discussion or, if needed, third party arbitration (Wang, S. and Ma, L.)
Data extraction and quality assessment
Two reviewers independently extracted data from included studies using a standardised data extraction tool. Two reviewers (Deng, H. and Xiao, L) independently evaluated the methodological quality of the included studies. RCTs were appraised with the modified Jadad Score (total score = 7), which includes assessment items for randomisation, concealment of allocation, double-blinding, and withdrawal and dropouts. Cohort studies were assessed with the Newcastle-Ottawa Quality Assessment Scale (total score = 9) (Wells et al. Citation2013), which includes assessment items for selection, comparability, and exposure. A score of ≥5 points was considered high-quality.
Statistical analysis
Statistical analyses were performed using Cochrane Review Manager software (RevMan 5.3). Risk ratios (RR) with 95% confidence intervals (CIs) were used to determine associations between dichotomous variables. Heterogeneity was assessed by the inconsistency index (I2). A random-effects model was used to pool studies with significant heterogeneity, determined as an inconsistency index (I2) ≥ 50%, otherwise, a fixed-effect model was used. If heterogeneity existed, a subgroup or sensitivity analysis was performed to detect the source. Publication bias was assessed with a funnel plot.
Results
Study selection
The searches identified 195 potentially eligible records, and 101 records were retained after removing duplicates. After scrutinising the titles and abstracts, the full text of 24 articles were reviewed. Reasons for exclusion were study design, interventions other than PRP, and definition of RIF included a different number of failed treatment cycles. Finally, 10 studies (8 in English, 2 in Chinese) were included in this meta-analysis (Supplementary Figure 1).
Study characteristics
The characteristics of the ten included studies are shown in . Six studies were RCTs, and four were cohort studies. One study reported negative results (Tehraninejad et al. Citation2021), and nine studies reported positive results. Studies were conducted in Iran (n = 5), China (n = 3), Egypt, and Turkey, and all were published in the last 5 years (2019–2022). All women were aged below 40 years. Sample sizes of the included studies varied from 70 to 393. Dose of PRP, which was infused into the uterine cavity before ET, was grouped as: 0.5 mL (n = 4), 0.5−1 mL (n = 1), and 1 mL (n = 5). Seven studies described PRP platelet count as four to five or four to seven times more than peripheral blood, and two study recorded the exact PRP platelet count (Coksuer et al. Citation2019). Blastocysts were transferred in seven studies, cleavage embryos were transferred in one study, and two articles did not provide that information.
Table 1. Characteristics of the included studies.
Risk of bias within studies
Of the ten studies, seven were assessed as having a low risk of bias and three were assessed as having a high risk of bias ( and ). RCTs assessed as having a high risk of bias had an unclear risk of bias for allocation concealment and double blinding and some lacked a clear description of the randomisation scheme. Cohort studies assessed as having a high risk of bias had an unclear risk of bias for comparability.
Table 2. Quality assessment of randomised controlled trials by the modified JADAD scale (max. 7–points).
Table 3. Quality assessment of cohort studies by the Newcastle-Ottawa Quality Assessment Form (max. 9–points).
Outcomes
Clinical pregnancy rate
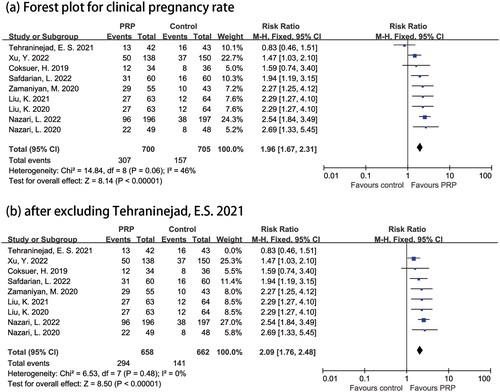
A clinical pregnancy was defined as the presence of a gestational sac with an embryo on ultrasound. Clinical pregnancy rate was reported by nine studies (n = 1405; 700 cases and 705 controls)(Coksuer et al. Citation2019, Liu et al. Citation2020, Citation2021, Nazari et al. Citation2020, Safdarian et al. Citation2020, Tehraninejad et al. Citation2021, Zamaniyan et al. Citation2021, Nazari et al. Citation2022, Xu et al. Citation2022). The meta-analysis demonstrated a significantly higher clinical pregnancy rate in women treated with PRP compared to controls (RR = 1.96, 95% CI [1.67, 2.31], p < 0.00001). There was evidence of low heterogeneity between studies (I2 = 46%) (). When one study, which reported negative results, was excluded, effect size was similar but there was no evidence of heterogeneity between studies (I2 = 0%) (Tehraninejad et al. Citation2021; ). A funnel plot revealed no significant publication bias (Supplementary Figure 2).
Figure 1. Forest plot for clinical pregnancy rate.
PRP: platelet-rich plasma; CI: confidence interval.
Chemical pregnancy rate
A chemical pregnancy was defined as a positive serum β-hCG (14 days after ET). Chemical pregnancy rate was reported in eight studies (n = 1358; 678 cases and 680 controls) (Nazari et al. Citation2020, Rageh et al. Citation2020, Safdarian et al. Citation2020, Liu et al. Citation2021, Tehraninejad et al. Citation2021, Zamaniyan et al. Citation2021, Nazari et al. Citation2022, Xu et al. Citation2022). The meta-analysis demonstrated a significantly higher chemical pregnancy rate in women treated with PRP compared to the controls (RR = 1.79, 95% CI [1.54, 2.08], p < 0.00001). There was evidence of low heterogeneity between studies (I2 = 29%) (Supplementary Figure 3).
Implantation rate
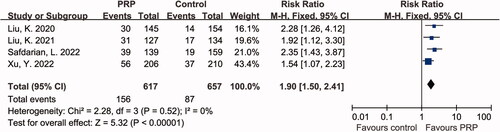
Implantation rate was defined as the number of gestational sacs divided by the number of transferred embryos. Implantation rate was reported in four studies (n = 560; 266 cases and 294 controls) (Liu et al. Citation2020, Safdarian et al. Citation2020, Liu et al. Citation2021, Xu et al. Citation2022). The meta-analysis demonstrated a significantly higher implantation rate in women treated with PRP compared to controls (RR = 1.90, CI [1.50, 2.41], p < 0.00001). There was no evidence of heterogeneity between studies (I2 = 0%) ().
Figure 2. Forest plot for implantation rate.
PRP: platelet-rich plasma; CI: confidence interval.
Live birth rate
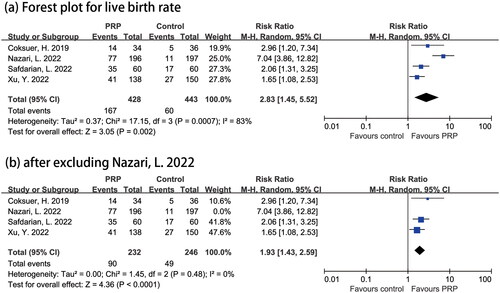
Live birth rate was defined as the number of live birth events (> 24 weeks of gestation) divided by the number of ET cycles. Live birth rate was reported in four studies (n = 871; 428 cases and 443 controls) (Coksuer et al. Citation2019, Safdarian et al. Citation2020, Nazari et al. Citation2022, Xu et al. Citation2022). The meta-analysis demonstrated a significantly higher live birth rate in women treated with PRP compared to controls (RR = 2.83, CI [1.45, 5.52], p = 0.0007). There was evidence of high heterogeneity between studies (I2 = 83%) (). Sensitivity analysis showed the robustness of the pooled RR, ranging from RR 1.93, CI [1.43, 2.59] to 3.49. When one study that used stringent inclusion criteria (Nazari et al. Citation2022; patient age ≤ 38 years versus < 40 years, serum FSH level ≤10 mIU/mL on day 2 or 3 of the menstrual cycle, exclusion of patients with PCOS and OHSS, which may result in a higher rate of euploid embryos) was excluded, effect size was similar but there was no evidence of heterogeneity between studies (RR = 1.93, CI [1.43, 2.59], p < 0.0001, I2 = 0%) ().
Figure 3. Forest plot for live birth rate
. PRP: platelet-rich plasma; CI: confidence interval.
Abortion rate
Abortion was defined as spontaneous pregnancy loss in a pregnant woman. Abortion rate was reported in four studies (n = 304; 206 cases and 98 controls). The meta-analysis demonstrated a significantly higher abortion rate in controls compared to women treated with PRP (RR = 0.40, 95% CI [0.18, 0.90], p = 0.03). There was evidence of low heterogeneity between studies (I2 = 59%) (Supplementary Figure 4a). When the study with stringent inclusion criteria was excluded (Nazari et al. Citation2022), effect size was not significant but there was no evidence of heterogeneity between studies (RR = 0.59, 95% CI [0.26, 1.38], p = 0.23, I2 = 18%) (Supplementary Figure 4b).
Discussion
In this meta-analysis, data from ten studies (n = 1555; 775 cases and 780 controls) were pooled to investigate the effect of intrauterine perfusion of autologous PRP on pregnancy outcomes in women with RIF. Findings suggest that pregnancy outcomes, including clinical pregnancy rate, chemical pregnancy rate, implantation rate, live birth rate and abortion rate were improved in women treated with PRP compared to controls. This data confirms that PRP improves live birth rate, which may be considered the most critical clinical outcome, in patients with RIF.
There were several strengths associated with our meta-analysis. To minimise heterogeneity across study populations, a narrowly defined criterion was used to identify patients with RIF (at least three failed ET cycles). Studies involving patients with one or two implant failures or undefined RIF were excluded. Busnelli et al. reported that a definition of RIF based on three failed attempts (but not two) was justified as the rate of false-positive diagnoses of RIF is reduced (from 46% to 25%) (Busnelli et al. Citation2020). Only one included article reported negative results. The methodological design, quality of the transferred embryos, and the preparation and dosage of PRP in the study that reported negative results were not obviously different from the other studies evaluated in this analysis. However, the negative study excluded women with an endometrial thickness < 7 mm, whereas other studies did not have similar restrictions. Evidence shows that PRP may improve pregnancy outcomes by promoting endometrial growth and receptivity (Eftekhar et al. Citation2018, Nazari et al. Citation2019), which implies that PRP may be helpful in cases with a thin endometrium.
RIF is a common concern among researchers, physicians and patients. Patients with RIF desperately require more innovative treatments to improve their likelihood of pregnancy. In 2016, Farimani et al. first administered PRP to nine infertile women with RIF, and six women achieved clinical pregnancy (66%) (Farimani et al. Citation2016). Despite typical limitations, this pilot study suggested that PRP may be beneficial for patients with RIF. Subsequently, numerous studies have been published on this topic, supporting the efficacy of PRP (Nazari et al. Citation2016, Mehrafza et al. Citation2019). Mehrafza et al. conducted a cohort study including 123 patients with history of more than two failed cycles to compare the impact of PRP and G-CSF. Findings showed that intrauterine infusion of PRP had a more positive effect on pregnancy outcomes compared to G-CSF (Mehrafza et al. Citation2019). A previous meta-analysis assessing the effect of PRP in women undergoing frozen-thawed ET supported the use of PRP as a treatment strategy in patients with a thin endometrium and RIF. However, this study was limited as RIF was defined as one to three or more failures of IVF-ET therapy compared to our narrower criterion of infertile women who had experienced at least three implantation failures (Maleki-Hajiagha et al. Citation2020).
The mechanisms underlying the role of PRP in women with RIF remain to be elucidated. Implantation is a three-step process that consists of (1) apposition of the blastocyst to the implantation site, (2) adhesion of the blastocyst to the endometrial epithelium (3) and invasion of a receptive endometrium by the embryo. Successful implantation requires a complex interplay between cytokines, chemokines, an immune infiltrate, adhesion molecules, and growth and other factors. The expression of growth factors in the endometrium of women with RIF is less than normal fertile women (Sak et al. Citation2013). Thus, intrauterine infusion of PRP, which is rich in granules that contain numerous proteins, cytokines and growth factors, may improve endometrial receptivity and implantation (Alves and Grimalt Citation2018, Bos-Mikich et al. Citation2019, Sfakianoudis et al. Citation2019). Amable et al. quantified 37 growth factors and cytokines in different fractions obtained during PRP preparation. Twelve growth factors and cytokines were secreted from activated platelets (Amable et al. Citation2013). Several factors have paracrine effects on the endometrium and regulate the effects of proliferation, apoptosis, inflammation, cell adhesion, chemotaxis and the immune response during the process of blastocyst implantation (Srivastava et al. Citation2013). For example, EGF is present in PRP. Human endometrial tissue contains EGF receptors, which regulate the production of VEGF, locally promote decidual angiogenesis, placental angiogenesis and endometrial hyperplasia, and play a key role in successful implantation (Furukawa et al. Citation2009). In vitro and in vivo studies imply that PRP may impact the proliferation and migration of mesenchymal stem cells, which play an essential role in the growth and function of the endometrium (Wang et al. Citation2018).
This review was associated with some limitations. First, the number of included studies reduced the statistical power. Second, six RCTs and four cohort studies were included in this meta-analysis. PRP is an emerging technology for RIF, and the number of relevant published clinical studies is small; therefore, cohort studies were included. This is unlikely to affect the findings, as data for clinical pregnancy rates was stratified into subgroups based on RCTs or cohort studies, and results for the primary and subgroup analyses were similar (data not shown). Most included studies lacked reasonable measures for allocation concealment and blinding, which reduced their methodological quality. However, objective outcomes were unlikely to be influenced by blinding. Last, most studies did not describe the components and concentrations of PRP, so we could not discuss the specific effects of PRP composition on pregnancy outcomes.
Clinical implications
As a preparation of autologous blood, PRP eliminates the risk of immune responses and the spread of transmissible diseases. Combined with its low cost and evidence of effectiveness, PRP shows potential for assisted reproduction. However, PRP application remains at the experimental stage. Previously conducted RCTs of PRP for fertility lacked robust study designs, and did not describe PRP preparation (Urman et al. Citation2019). Variability in PRP formulations and patient-specific factors, including the use of drugs, can impact clinical efficacy and pose challenges when interpreting the literature (Le et al. Citation2019). Before PRP is widely used for patients with suboptimal endometrial growth, its mechanism of action, dosage, preparation process, and other issues must be clarified. Therefore, more well-designed studies with relevant outcomes, such as live birth rate, should be conducted.
Conclusion
Our meta-analysis shows that PRP has potential to improve pregnancy outcomes in women with RIF. However, given the limited number and variable quality of the included studies, the current evidence should be interpreted with caution, and more randomised clinical trials with larger sample sizes are needed.
Ethical approval
Ethical approval was unnecessary in this study because it was a systematic review and meta-analysis of existing published articles.
Author contributions
SQW, LM and HYD defined the research problem. SQW designed the search strategy. HYD, LFX and ZJL were responsible for searching and screening literature, and performed statistical analysis of the data. The manuscript was written by HYD and reviewed by SQW and LM. All authors critically reviewed the manuscript for important intellectual content and gave approval of the final version to be published.
Supplemental Material
Download Zip (1.4 MB)Data availability statement
All data generated or analysed during this study are included in published articles.
Additional information
Funding
References
- Alves, R. and Grimalt, R., 2018. A review of platelet-rich plasma: history, biology, mechanism of action, and classification. Skin Appendage Disorders, 4 (1), 18–24.
- Amable, P.R., et al., 2013. Platelet-rich plasma preparation for regenerative medicine: optimization and quantification of cytokines and growth factors. Stem Cell Research & Therapy, 4 (3), 67–67.
- Bos-Mikich, A., et al., 2019. Platelet-rich plasma or blood-derived products to improve endometrial receptivity? Journal of Assisted Reproduction and Genetics, 36 (4), 613–620.
- Busnelli, A., et al., 2020. How common is real repeated implantation failure? An indirect estimate of the prevalence. Reproductive Biomedicine Online, 40 (1), 91–97.
- Busnelli, A., et al., 2021. Efficacy of therapies and interventions for repeated embryo implantation failure: a systematic review and meta-analysis. Scientific Reports, 11 (1), 1747.
- Cavalcante, M.B., et al., 2020. Intrauterine perfusion immunotherapies in recurrent implantation failures: systematic review. American Journal of Reproductive Immunology (New York, N.Y. : 1989), 83 (6), e13242.
- Chen, T., et al., 2020. The effect of endometrial injury on reproductive outcomes of frozen-thawed embryo transfer cycles in women with one implantation failure. The Journal of International Medical Research, 48 (3), 300060520913130.
- Christgau, M., et al., 2006. Growth factors and cytokines in autologous platelet concentrate and their correlation to periodontal regeneration outcomes. Journal of Clinical Periodontology, 33 (11), 837–845.
- Coksuer, H., Akdemir, Y. and Barut, M.U., 2019. Improved in vitro fertilization success and pregnancy outcome with autologous platelet-rich plasma treatment in unexplained infertility patients that had repeated implantation failure history. Gynecological Endocrinology : The Official Journal of the International Society of Gynecological Endocrinology, 35 (9), 815–818.
- Coughlan, C., et al., 2014. Recurrent implantation failure: definition and management. Reproductive Biomedicine Online, 28 (1), 14–38.
- Dieamant, F., et al., 2019. New therapeutic protocol for improvement of endometrial receptivity (PRIMER) for patients with recurrent implantation failure (RIF) - A pilot study. JBRA Assisted Reproduction, 23 (3), 250–254.
- Eftekhar, M., et al., 2018. Can autologous platelet rich plasma expand endometrial thickness and improve pregnancy rate during frozen-thawed embryo transfer cycle? A randomized clinical trial. Taiwanese Journal of Obstetrics & Gynecology, 57 (6), 810–813.
- Farimani, M., Bahmanzadeh, M. and Poorolajal, J., 2016. A new approach using autologous Platelet-Rich Plasma (PRP) to treat infertility and to improve population replacement rate. Journal of Research in Health Sciences, 16 (3), 172–173.
- Furukawa, Y., et al., 2009. The production of vascular endothelial growth factor and metalloproteinase via protease-activated receptor in human endometrial stromal cells. Fertility and Sterility, 91 (2), 535–541.
- Le, A.D.K., et al., 2019. Platelet-rich plasma. Clinics in Sports Medicine, 38 (1), 17–44.
- Liu, K., et al., 2021. Role of platelet-rich plasma in improving pregnancy outcomes in patients with recurrent implantation failure. Progress in Obstetrics and Gynecology, 30 (01), 42–44, 49.
- Liu, K., et al., 2020. Effect of intrauterine perfusion of platelet-rich plasma on pregnancy outcome in women with recurrent implantation failure. Journal of Reproductive Medicine, 29 (05), 667–670.
- Maleki-Hajiagha, A., et al., 2020. Intrauterine infusion of autologous platelet-rich plasma in women undergoing assisted reproduction: a systematic review and meta-analysis. Journal of Reproductive Immunology, 137, 103078.
- Margalioth, E.J., et al., 2006. Investigation and treatment of repeated implantation failure following IVF-ET. Human Reproduction (Oxford, England), 21 (12), 3036–3043.
- Marx, R.E., 2001. Platelet-rich plasma (PRP): what is PRP and what is not PRP? Implant Dentistry, 10 (4), 225–228.
- Mehrafza, M., et al., 2019. Comparing the impact of autologous platelet-rich plasma and granulocyte colony stimulating factor on pregnancy outcome in patients with repeated implantation failure. Journal of Reproduction & Infertility, 20 (1), 35–41.
- Moher, D., et al., 2020. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med, 6(7), e1000097.
- Nazari, L., et al., 2016. Effects of autologous platelet-rich plasma on implantation and pregnancy in repeated implantation failure: a pilot study. International Journal of Reproductive Biomedicine, 14 (10), 625–628.
- Nazari, L., et al., 2019. Effects of autologous platelet-rich plasma on endometrial expansion in patients undergoing frozen-thawed embryo transfer: a double-blind RCT. International Journal of Reproductive Biomedicine, 17 (6), 443–448.
- Nazari, L., et al., 2020. The effects of autologous platelet-rich plasma in repeated implantation failure: a randomized controlled trial. Human Fertility (Cambridge, England), 23 (3), 209–213.
- Nazari, L., et al., 2022. The effects of autologous platelet-rich plasma on pregnancy outcomes in repeated implantation failure patients undergoing frozen embryo transfer: a randomized controlled trial. Reproductive Sciences (Thousand Oaks, Calif.), 29 (3), 993–1000.
- Rageh, K.A.I., Barakat, A. and Mohamed, A., 2020. PRP in recurrent implantation failure, hope or hype! ? A prospective randomized controlled study. Evidence Based Women s Health Journal, 10, 46–53.
- Safdarian, L., et al., 2020. Efficacy of the intrauterine infusion of platelet-rich plasma on pregnancy outcomes in patients with repeated implantation failure: a randomized control trial. International Journal of Women’s Health and Reproduction Sciences, 10 (1), 38–44.
- Sak, M.E., et al., 2013. Fibroblast growth factor-1 expression in the endometrium of patients with repeated implantation failure after in vitro fertilization. European Review for Medical and Pharmacological Sciences, 17 (3), 398–402.
- Samadi, P., Sheykhhasan, M. and Khoshinani, H.M., 2019. The use of platelet-rich plasma in aesthetic and regenerative medicine: a comprehensive review. Aesthetic Plastic Surgery, 43 (3), 803–814.
- Sfakianoudis, K., et al., 2019. Successful implantation and live birth following autologous platelet-rich plasma treatment for a patient with recurrent implantation failure and chronic endometritis. In Vivo (Athens, Greece), 33 (2), 515–521.
- Somigliana, E., et al., 2018. Repeated implantation failure at the crossroad between statistics, clinics and over-diagnosis. Reproductive Biomedicine Online, 36 (1), 32–38.
- Srivastava, A., et al., 2013. Profiles of cytokines secreted by isolated human endometrial cells under the influence of chorionic gonadotropin during the window of embryo implantation. Reproductive Biology and Endocrinology : RB&E, 11, 116–116.
- Tehraninejad, E.S., et al., 2021. Autologous platelet-rich plasma infusion does not improve pregnancy outcomes in frozen embryo transfer cycles in women with history of repeated implantation failure without thin endometrium. The Journal of Obstetrics and Gynaecology Research, 47 (1), 147–151.
- Urman, B., Boza, A. and Balaban, B., 2019. Platelet-rich plasma another add-on treatment getting out of hand? How can clinicians preserve the best interest of their patients? Human Reproduction (Oxford, England), 34 (11), 2099–2103.
- Wang, X., et al., 2018. Investigation of platelet-rich plasma in increasing proliferation and migration of endometrial mesenchymal stem cells and improving pregnancy outcome of patients with thin endometrium. Journal of Cellular Biochemistry, 120 (5), 7403–7411.
- Wells, G., Shea, B. and O’Connell, D., 2013. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp.
- Whitney, K.E., et al., 2017. Current perspectives on biological approaches for osteoarthritis. Annals of the New York Academy of Sciences, 1410 (1), 26–43.
- Xu, Y., et al., 2022. Intrauterine perfusion of autologous platelet-rich plasma before frozen-thawed embryo transfer improves the clinical pregnancy rate of women with recurrent implantation failure. Front Med (Lausanne), 9, 9850002.
- Zamaniyan, M., et al., 2021. Effect of platelet-rich plasma on pregnancy outcomes in infertile women with recurrent implantation failure: a randomized controlled trial. Gynecological Endocrinology : The Official Journal of the International Society of Gynecological Endocrinology, 37 (2), 141–145.
- Zhang, M., et al., 2018. Applications and efficacy of platelet-rich plasma in dermatology: a clinical review. Journal of Cosmetic Dermatology, 17 (5), 660–665.