

Introduction
Ovarian cancer is one of the three most common gynaecological tumours. However, there are no obvious symptoms in the early stage and no effective early screening methods. Furthermore, the high recurrence rate of advanced ovarian cancer and resistance of recurrent ovarian cancer to chemotherapy make ovarian cancer one of the most challenging malignancies to treat. Poly adenosine diphosphate-ribose polymerase (PARP) is a family of enzymes involved in single-stranded DNA repair (Caldecott et al. Citation1996, Konecny and Kristeleit Citation2016). Since it was discovered that the loss or inhibition of PARP causes increased apoptosis and cell cycle arrest, the role of PARP in DNA repair has become an area of interest for tumour therapy (Jacobson et al. Citation1985).
Consequently, PARP inhibitors (PARPis) have become exciting new treatments for ovarian cancer, especially in females with breast cancer (BRCA) 1 or BRCA2 mutations or with non-functional homologous recombination repair pathways (Laganà et al. Citation2015, LaFargue et al. Citation2019). Three PARPis have been approved in the United States for treating epithelial ovarian cancer: olaparib, niraparib, and rucaparib. However, various adverse events (AEs) occur during therapy with these drugs, among which increased serum creatinine is common. The cause and mechanism of elevated serum creatinine during PARPi therapy are still unclear. Furthermore, distinguishing this AE from acute kidney injury (AKI) remains challenging for clinicians. Herein, we report a patient with elevated serum creatinine during first-line maintenance therapy with olaparib. Additionally, we review the relevant literature to learn about the influence of PARPis on creatinine levels and the possible causes and mechanisms of the changes in serum creatinine levels.
Case presentation
The patient was a 53-year-old BRCA1-mutation positive female (height: 153 cm; weight: 57.5 kg) who was referred for surgical resection of a ‘right adnexal mass’ on October 15, 2020. Intra-operative frozen section confirmed a diagnosis of poorly differentiated carcinoma of the right adnexa. The patient then underwent a comprehensive staging operation, and complete resection (R0) of the cancer was performed. The post-operative paraffin-section was diagnosed as stage IIIB high-grade serous adenocarcinoma of the right fallopian tube. Six cycles of paclitaxel plus carboplatin chemotherapy were administered after the operation. After chemotherapy, the cancer antigen 125 level was 4.2 U/ml. Combined with the computed tomography result, the treatment efficacy was evaluated as a complete response.
After fully informed communication, the patient selected olaparib for maintenance therapy. Hence, oral maintenance therapy with olaparib was commenced at a dose of 300 mg bid. Renal function was measured regularly, and serum creatinine levels were observed to increase progressively. Renal ultrasonography revealed that there was no post-renal obstruction or nephropathy. However, the patient was worried about a further increase in creatinine levels and irreversible damage to renal function; hence, we suggested that the patient discontinue the drug and visit a nephrologist. Olaparib was discontinued on the 42nd day of administration, and the serum creatinine decreased afterward (). The nephrologist recommended a glomerular filtration rate (GFR) scan to evaluate renal function further. Unfortunately, the patient refused to undergo the test after understanding the test method. After the creatinine levels decreased, the patient was advised to recommence olaparib, reduce the dose to 150 mg bid, and monitor creatinine levels dynamically.
Figure 1. Serum creatinine levels of the patient.
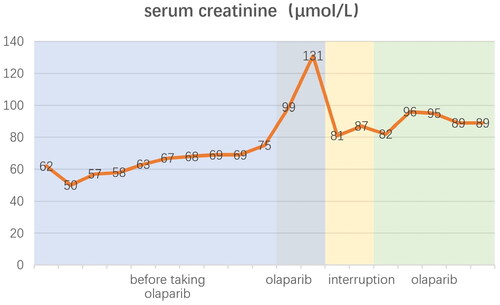
At the time of writing this report, the patient had continued maintenance therapy for 14 months, her serum cancer antigen 125 level was <10 U/ml, and her serum creatinine was about 90 µmol/L. Moreover, no tumour recurrence or adverse events had been observed.
Discussion
Increased serum creatinine is one common AE in patients treated with PARPis. In the clinical trial of olaparib (Ray-Coquard et al. Citation2019), the proportion of increased creatinine levels in the olaparib group ranged from 20% to 61%. Apart from two (0.4%) of the 535 patients treated with olaparib who had grade 3–4 elevation of creatinine in the PAOLA-1 trial, and four (2%) patients treated with olaparib who had grade 3–4 elevation of creatinine in the pooled data trial, other patients had a milder increase in creatinine levels (grade 1–2).
A single-centre retrospective cohort study (Zibetti Dal Molin et al. Citation2020) examined serum creatinine changes in patients with ovarian or endometrial cancer treated with the PARPis: olaparib, niraparib, or rucaparib. The discrepancy in the calculated and measured GFRs was compared. The study included 211 patients, of whom 64 (30%) developed elevated serum creatinine during treatment, and 23 (36%) underwent 32 GFR scans (six patients underwent more than one scan), of which only six were lower than normal. The calculated GFRs were almost the same as the patients’ baseline. This suggests that the increased serum creatinine in patients receiving PARPis may be unrelated to decreased GFRs. Furthermore, paying more attention to other factors that may affect GFR might be necessary throughout treatment.
Another study involving 66 patients (Bruin et al. Citation2021) found that olaparib may inhibit renal transporters, resulting in a reversible and dose-dependent increase in creatinine levels. Although this does not affect the GFR, creatinine-derived estimated GFR (eGFR) measurement might underestimate the GFR of patients receiving olaparib. Hence, alternative renal markers, such as cystatin C, may be used to accurately calculate the eGFR in patients on olaparib therapy since the cystatin C-derived eGFR was the same before, during, and after olaparib therapy.
Several studies have shown that creatinine is secreted into urine through renal transporters (e.g. multidrug and toxin extrusion 1, multidrug and toxin extrusion 2-k, organic cation transporter 1, and organic cation transporter 2) (Coleman et al. Citation2017). This pathway is inhibited by various PARPis in vitro, including olaparib (McCormick and Swaisland Citation2017) and veliparib (Kikuchi et al. Citation2013). Therefore, elevated creatinine levels may inhibit renal transporters more than actual renal injury.
LaFargue et al. (Citation2019) pointed out that increased serum creatinine may not reflect an actual decrease in GFR or renal insufficiency. Furthermore, they suggest that if there are concerns about kidney disease based on clinical signs, symptoms, and biochemical or radiographic abnormalities, other methods for evaluating GFR, such as a radioactive nucleotide scan, should be employed. However, if the GFR is appropriate (i.e. GFR is typical or inconsistent with elevated creatinine levels), dose reduction or discontinuation of the drug can be avoided.
Drew et al. (Citation2020) suggested that patients receiving rucaparib who present with elevated serum creatinine be suspected of having AKI. Hence, these patients should first receive appropriate clinical evaluation and investigation to exclude and treat other causes of AKI. During these preliminary investigations, rucaparib therapy can be suspended. Mildly elevated serum creatinine levels do not require dose adjustment. In patients with creatinine clearance rates <30 ml/min or those requiring dialysis, a recommended dose has not been determined because there has been no special clinical study of rucaparib in such patients. Therefore, it is recommended that renal function be monitored monthly in patients receiving rucaparib.
The sensitivity of recurrent ovarian cancer to extra rounds of chemotherapy is still an important factor related to the prognosis of patients with ovarian cancer. Furthermore, the sensitivity to chemotherapy is closely related to progression-free survival (PFS). PARPi maintenance therapy can significantly prolong PSF and improve the prognosis of patients with advanced ovarian cancer after the remission of surgery plus adjuvant chemotherapy (Ray-Coquard et al. Citation2019, Fagotti et al. Citation2020). PARPis are a novel type of antitumour treatment with a different mechanism of action for ovarian cancer therapy. Hence, a comprehensive understanding of its mechanisms of action, indications, and side effects is crucial to ensure safe therapy with PARPis in patients. In addition to haematological and gastrointestinal toxicity, elevated serum creatinine is a common side-effect of PARPis. Presently, the mechanism through which PARPis cause elevated serum creatinine levels remains unclear, and different PARPis seem to have different mechanisms. For patients with elevated creatinine levels, evaluating renal function to exclude AKI and dose adjustment of PRAPis are issues that should be focussed on by clinicians. Renal function can be evaluated by methods other than serum creatinine evaluation to determine whether the dose of PARPis needs to be adjusted. After serum creatinine levels have increased, clarity is still required regarding how the PARPi dose should be adjusted.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of West China Second University Hospital of Sichuan University, and the patient provided written informed consent.
Consent for publication
Written informed consent to publish the case report was obtained from the patient.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bruin, M.A.C., et al., 2021. A real or apparent decrease in glomerular filtration rate in patients using olaparib? European journal of Clinical Pharmacology, 77 (2), 179–188.
- Caldecott, K.W., et al., 1996. XRCC1 polypeptide interacts with DNA polymerase beta and possibly poly (ADP-ribose) polymerase, and DNA ligase III is a novel molecular ‘nick-sensor’ in vitro. Nucleic acids Research, 24 (22), 4387–4394.
- Coleman, R.L., et al., 2017. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. The lancet, 390 (10106), 1949–1961.
- Drew, Y., et al., 2020. Real‐world delivery of Rucaparib to patients with ovarian cancer: recommendations based on an integrated safety analysis of ARIEL2 and Study 10. The oncologist, 25 (1), e109–e119.
- Fagotti, A., et al., 2020. Randomized trial of primary debulking surgery versus neoadjuvant chemotherapy for advanced epithelial ovarian cancer (SCORPION-NCT01461850). International journal of Gynecological Cancer : official Journal of the International Gynecological Cancer Society, 30 (11), 1657–1664.
- Jacobson, E.L., et al., 1985. Cellular recovery of dividing and confluent C3H10T1/2 cells from N-methyl-N′-nitro-N-nitrosoguanidine in the presence of ADP ribosylation inhibitors. Carcinogenesis, 6 (5), 715–718.
- Kikuchi, R., et al., 2013. Prediction of clinical drug–drug interactions of veliparib (ABT-888) with human renal transporters (OAT1, OAT3, OCT2, MATE1, and MATE2K). Journal of Pharmaceutical Sciences, 102 (12), 4426–4432.
- Konecny, G.E. and Kristeleit, R.S., 2016. PARP inhibitors for BRCA1/2-mutated and sporadic ovarian cancer: current practice and future directions. British journal of Cancer, 115 (10), 1157–1173.
- LaFargue, C.J., et al., 2019. Exploring and comparing adverse events between PARP inhibitors. The Lancet. Oncology, 20 (1), e15–e28.
- Laganà, A.S., et al., 2015. Cytogenetic analysis of epithelial ovarian cancer’s stem cells: an overview on new diagnostic and therapeutic perspectives. European journal of Gynaecological Oncology, 36 (5), 495–505.
- McCormick, A. and Swaisland, H., 2017. In vitro assessment of the roles of drug transporters in the disposition and drug–drug interaction potential of olaparib. Xenobiotica; the Fate of Foreign Compounds in Biological Systems, 47 (10), 903–915.
- Ray-Coquard, I., PAOLA-1 Investigators., et al., 2019. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. The New England Journal of Medicine, 381 (25), 2416–2428.
- Zibetti Dal Molin, G., et al., 2020. Discrepancy in calculated and measured glomerular filtration rates in patients treated with PARP inhibitors. International journal of Gynecological Cancer, 30 (1), 89–93.