

Abstract
Integration of maternal and child health services can improve service utilisation. An operations research was conducted in a Nigerian tertiary hospital. A pilot study was conducted at three family planning (FP) and vaccination sites. A formative assessment was carried out using client records and key-informant interviews. Pre- and post-integration questionnaires were administered to 715 women attending the infant vaccination clinics. Themes were developed from the qualitative data and some verbatim quotes were reported. The quantitative data were analysed using Stata, version 17. Univariate and multivariate analyses were done to compare associations between categorical independent and outcome variables where applicable, with level of significance set at <0.05 and 95% confidence interval.
The health care workers were willing to integrate the two services but inadequate training and time constraint were key barriers. Significant increases in the knowledge of contraception (25.7% vs 34.7%, p = 0.001), intention to use contraception (31.2% vs 38.2%, p = 0.001), and number of new acceptors of FP (487 vs 664, p = 0.001), were recorded post-integration, even though it was difficult to determine whether the observed increase in new FP acceptors was due to increased patronage from the study participants and not from other clients who were not part of the study. Integration of FP education and infant vaccination services is a feasible and acceptable strategy for increasing contraceptive use among postpartum women, as vaccination clinic staff were willing to take on FP education along with their current duties.
What is already known on this subject? Few studies have reported on the outcomes related to FP and vaccination integration.
What the results of this study add? A simple model of FP education and infant vaccination services integration is a feasible and acceptable strategy for increasing contraceptive use among postpartum women. However, inadequate training and time constraint were major concerns for healthcare providers.
Implications of these findings for clinical practice and/or further research? Targeted family planning education and referral should be encouraged during infant vaccination visits. There is a need for further research to determine the providers’ skills necessary for integration and whether integration poses a risk to either service.
Impact statement
Introduction
Family planning (FP) and infant vaccination save lives and their goals are mutually supportive (FHI 360 Citation2010). The Expanded Programme on Immunisation (EPI) schedule overlaps the extended postpartum period of mothers, defined as the first 12 months after childbirth (Pfitzer et al. Citation2015). By the current EPI schedule in Nigeria, within the extended postpartum period, there are six infant vaccination visits- at birth, six weeks, 10 weeks, 14 weeks, six months and nine months. Research has shown that integrating postpartum family planning (PPFP) and infant vaccination services is a feasible, cost-effective, and acceptable strategy for increasing contraceptive use among postpartum women (Dulli et al. Citation2016).
To increase the uptake of PPFP, the World Health Organisation (WHO) recommends that PPFP should not be run as a ‘vertical’ programme, but integrated with existing maternal, new-born and child health services (WHO Citation2013). This recommendation is premised on the fact that between 50% and 60% of pregnant women make prenatal visits or have contact with health care providers at or soon after delivery, with additional contacts occurring for infant care and other child health services (Ross and Winfrey Citation2001). Locally, the 2018 Nigeria Demographic and Health Survey (NDHS) revealed that 67% of pregnant women in Nigeria receive antenatal care, while 42% of delivered mothers receive a postnatal check. The same Survey showed that even though only 31% of infants are completing basic vaccinations, with respect to specific vaccines, 65% of infants receive the first dose of DPT-HepB-Hib (Diphtheria, Pertussis, Tetanus, Hepatitis B and Hemophilus influenza type b) vaccine, 67% receive BCG, and 74% receive the first dose of polio vaccine (National Population Commission [Nigeria] and ICF International Citation2019). Given that more women bring their children for vaccination than they attend antenatal and postnatal clinics, incorporating PPFP education into infant vaccination visits has the potential of increasing uptake of PPFP (Ringheim et al. Citation2011, Cooper et al. Citation2015, Cooper et al. Citation2020).
Postpartum family planning is defined as the prevention of unintended or/and closely spaced pregnancies during the first one year following delivery (WHO Citation2013). Postpartum women who are not breastfeeding can get pregnant within 45 days of delivery, with some of them ovulating as early as 25 days postpartum (Jackson and Glasier Citation2011). Although the onset of fertility is significantly delayed in women who are breastfeeding, it is possible for lactating women to ovulate prior to their first menses, limiting their ability to accurately predict a return to fecundity (Gross and Burger Citation2002).
Pregnancy during the extended postpartum period carries the highest maternal and neonatal risks (Conde-Agudelo et al. Citation2012). This underscores the necessity of PPFP. Use of FP in the extended postpartum period may reduce the number of closely spaced pregnancies. Closely spaced pregnancies are more likely to result in miscarriage, anaemia, preterm birth, low birth weight, small for gestational age, neonatal, infant, child and maternal deaths (DaVanzo et al. Citation2007, Hounton et al. Citation2015). Thirty percent of maternal deaths and 10% of child mortality would be averted if pregnancies are spaced more than two years apart (Cleland et al. Citation2006).
Despite the numerous risks of pregnancy during the extended postpartum period and the significant benefits of PPFP, postpartum contraception use remains very low in developing countries, due to the high unmet need for FP in these countries, especially so in the postpartum period (Hounton et al. Citation2015). A review of DHS data from 27 countries found that, of the 95% of women 0–12 months postpartum who desire to prevent a subsequent pregnancy in the next 24 months, 70% of them are not using contraception (Ross and Winfrey Citation2001). In Ile-Ife, South-West Nigeria, where the present study was conducted, a previous study put the unmet need for FP during the first one year postpartum at 59.6% (Adeyemi et al. Citation2005).
Few studies have reported on the outcomes related to FP and vaccination integration (Cooper et al. Citation2015, Mackenzie et al. Citation2018, Nelson et al. Citation2019). This study sought to determine the knowledge, attitude and practice of PPFP among women attending infant vaccination clinics, the unmet need for FP and the effect of integrating FP education with infant vaccination visits on the uptake of PPFP at the Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC), Ile-Ife, Osun State, Nigeria.
Materials and methods
Study design and setting
This was an operations research with an exploratory sequential mixed method approach. The study was conducted in the OAUTHC, a foremost Teaching Hospital located in South-West Nigeria, that provides primary, secondary and tertiary healthcare services to the population in Osun State, where the hospital is located, as well as the neighbouring states of Oyo, Ondo and Ekiti. These services are provided via six health care units; Ife Hospital Unit (IHU), Ile-Ife, Wesley Guild Hospital (WGH), Ilesha, Dental Centre, Ile-Ife, Urban Comprehensive Health Centre, Eleyele, Ile-Ife, Rural Comprehensive Health Centre, Imesi-Ile, and Multipurpose Maternal and Child Health Centre, Ilesha. The hospital provides both vaccination and FP services, which run independently of each other, without any deliberate efforts or model linking the two services.
Sample size determination
Between five to 50 participants are considered adequate sample size for an In-depth Interview (IDI) study (Dworkin Citation2012). There were a total of 18 Nurses working morning and afternoon shifts in the immunisation and FP clinics of the three study sites. For the purpose of this study, it was assumed that saturation will be reached after interviewing 12 participants, which is about 2/3 of the staff, for the qualitative aspect.
The minimum sample size for the quantitative arm of the study was calculated using the formula for calculating single proportion: n = z2 x pq/e2, where n = minimum sample size, z = standard normal variate, which is 1.96 for a confidence level of 95%, p = prevalence of PPFP (of 40.6%, 0.41) from a previous study conducted in the study centre (Adeyemi et al. Citation2005), q = 1-p, e = margin of error, which is 0.05 at 95% confidence level. Substituting into the formula, n = 1.962 × 0.41 x (1–0.41)/0.052 ≈ 372. Allowing for 30% attrition rate, the calculated minimum sample size was 483.6, rounded up to 484. However, all consenting women who were in the extended postpartum period, and who brought their babies for routine vaccination visits at the three study sites within the study period, totalling 715, were recruited for the study.
Study procedure
A pilot study was conducted at the FP and vaccination units of three of the six health care units of the OAUTHC viz: WGH, Ilesha, Multipurpose Maternal and Child Health Centre, Ilesha and Urban Comprehensive Health Centre, Eleyele, Ile-Ife, Southwest Nigeria, over an eight-month period, between October 1, 2017, and May 31, 2018. One of the other three healthcare of units of the OAUTHC offer only dental services, while the other two offer either only FP or vaccination services, and not both, and so they were excluded from the study. Five trained research assistants were recruited to assist in the study.
Qualitative data
Twelve key-informant interviews (KIIs) were conducted for Nursing staff that provide infant vaccination and FP services (nine nurses from the vaccination clinics and three from the FP clinics) at the three study sites, to determine the perceived barriers against successful integration of the two services. The feasibility of integrating both services was assessed by the willingness of the infant vaccination clinics staff to take on FP education along with their current duties, as well as the willingness of the postpartum women visiting the infant vaccination clinics to discuss FP with staff at the vaccination clinics.
Quantitative data
A formative assessment was carried out in the first two weeks of the study, to retrospectively determine the monthly client load at the vaccination and FP clinics of the study sites, in the six months preceding the study, by reviewing the clinic records. This provided an estimate of the uptake of these services in the preceding six months to the commencement of the study.
Over a six-week period, questionnaires were self-administered to 715 women attending the infant vaccination clinics, pre-integration of FP education and vaccination services (i.e. before the trained staff started providing FP education to postpartum women attending the infant vaccination clinics), to determine their knowledge, attitude, and uptake of PPFP. All consenting women who were in the extended postpartum period, and who brought their babies for routine vaccination visits at the three study sites, were included in the study. For the purpose of this study, extended postpartum period was defined as the first 12 months after childbirth (Pfitzer et al. Citation2015).
Post-integration of these services, the same questionnaires were re-administered to the same 715 women who participated in the pre-integration survey, to re-assess their knowledge, attitude, and uptake of PPFP. These questionnaires were self-administered to the women at their subsequent infant vaccination visits. Client load at the FP clinics in our study sites were assessed pre- and post-integration of both services, using the clinic records.
Study interventions
The result of the formative assessment was used to develop an integration model for FP and vaccination services (), behavioural change communication materials as well as monitoring and evaluation tools. Nine infant vaccination clinic staff, recruited across the three study sites, were trained in FP education, after which they provided FP education and information leaflets to postpartum women attending the vaccination clinics.
Figure 1. Family planning education and vaccination integration model.
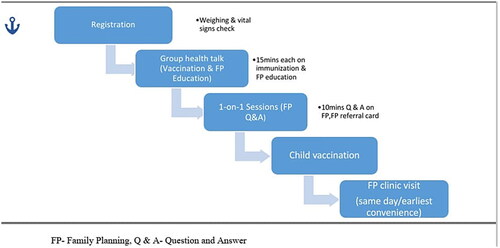
The FP education was provided to the postpartum women at every infant vaccination visit, first in group sessions, then individuals in need of further information or clarification were given one-on-one attention. Information provided included the mechanisms of action, side effects, medical eligibility criteria, as well as timing of safe commencement of specific contraceptive methods. FP education and information leaflets were provided both in the local dialect (Yoruba) and English Language. The women were given referrals to visit the FP clinics, same day/at their earliest conveniences. Women who had phones/volunteered their phone numbers were followed up for compliance with telephone calls and text messages.
Data analysis
The qualitative data was analysed using NVivo version 12. The data was transcribed, coded and categorised. Themes were developed and some verbatim quotes were reported.
The quantitative data was analysed using Stata version 17 (Statacorp, Texas USA). Descriptive statistics was conducted and continuous variables were presented as mean and standard deviation when normally distributed, or median and interquartile range when not normally distributed. Categorical variables were presented as frequency and percentages. Association between categorical variables and the current use or non-use of modern contraceptive was assessed using Pearson’s Chi-square. Fischer’s exact test was utilised when the expected cells were less than 5. Univariable logistic regression was conducted between sociodemographic and sexual characteristics, history of antenatal care, previous contraceptive use, and current use of contraceptive as the outcome. Variables with univariable p-value < 0.2 were utilised for the multivariable regression modelling. Backward elimination technique was utilised for the multivariable regression and parity and religion were chosen a priori. Collinearity was assessed using the variance inflation factor. Two-tailed test of hypothesis was assumed and statistically significant levels were set at p-value < 0.05.
Ethics
Ethical clearance for this study was obtained from the Ethics and Research Committee of the OAUTHC, with protocol number ERC/2017/03/12. Written informed consent was obtained from the study participants.
Results
Qualitative Data
Perceived barriers and benefits to integrating postpartum FP education with infant vaccination visits amongst health care providers
The following main themes were identified from the KIIs:
Training concerns
All the 12 Community Health Extension and Nursing staff, who provide FP and infant vaccination services in the OAUTHC, that were interviewed, had had previous training in FP, but a long time ago….' Yes, I have some experience in family planning but my last training in family planning was in 1995’ (a 46-year-old Assistant Director of Nursing). All the infant vaccination clinics staff felt happy and ready to take on FP education along with their current duties but stressed the need for re-training and employment of more staff in order to cope with the consequent increased workload.
Level of FP demand
Opinions concerning the demand for FP varied amongst the interviewed staff, but overall, they agreed it had increased in recent times. A 34-year-old Assistant Nursing Officer said: ‘…Now I will say it’s high. Unlike before, people are becoming more aware of family planning and even looking at the present situation, the economic situation of Nigeria, no woman, most of them don’t want their children to suffer, likewise they themselves, so I think they are patronising family planning.’
Time constraints
The infant vaccination clinic staff identified time constraint as one of the problems militating against FP education during infant vaccination visits. One of them said: ‘But let me say the patients most times come late to the clinic. They are always in a hurry to go home and most times we have to like (sic) encourage them to listen to health talk. What they want to do is quickly come in, take vaccination and go home. So those are the challenges, workload is not a problem’
Perceived benefits
The infant vaccination providers believed that integrating postpartum FP education into infant vaccination clinic visits is a particularly good idea, as stated by one of the respondents: ‘About 50–60 mothers bring their babies daily for vaccination. Integrating family planning education into the vaccination visits will afford the women the opportunity of interacting and sharing their family planning experiences. This will make more women decide to do family planning’ (A 27-year-old Nursing officer).
Information delivery
The infant vaccination providers all agreed that the use of FP information leaflets in infant vaccination clinics, in addition to the FP information given at these clinics, will further contribute to improving the uptake of PPFP.
Quantitative Data
Sociodemographic characteristics of the providers included in the KIIs
All the 12 provider participants were females, with a mean age of 34.67 years. There were two Assistant Directors of Nursing, three Chief Nursing Officers, three Assistant Chief Nursing Officers and four Nursing Officers, from the most senior to the least, respectively. Their different cadres corresponded to their years of experience in nursing.
Sociodemographic, reproductive and sexual characteristics of postpartum women attending vaccination clinics in the OAUTHC
The age of the study participants ranged between 18 to 50 years, with a mean ± SD age of 30.4 ± 5.5 years. Most of them were married (659/672, 98.1%), Christians (554/655, 84.6%) and with tertiary level of education (451/670, 67.3%). The parity of the women ranged from 1 to 13, with a median (IQR) parity of 2 (1–3). Majority of the women had resumed sexual intercourse following their last childbirth (419/648, 64.7%). Though most (466/642, 72.6%) of the women desired to get pregnant again/have another baby, the majority (372/408, 91.2%) of them desired to postpone pregnancy for at least 24 months. These characteristics are shown in .
Table 1. Sociodemographic, reproductive and sexual characteristics of postpartum women attending immunisation clinics in the OAUTHC.
Family planning awareness and uptake amongst postpartum women attending vaccination clinics in the OAUTHC
Most (671/680, 98.7%) of the respondents were aware of FP, and the most common source of information on FP were hospital/health workers (512/671, 76.3%) (). Of those who were aware of contraception, the majority (513/671, 76.5%) were aware of condoms, nearly one-half knew about intrauterine contraceptive devices (IUCD), injectables (321/671, 47.8% each) and pills (316/671, 47.1%), while more than a third (251/671, 37.4%) were aware of implants. The least known method of contraception was tubal ligation (137/671, 20.4%). Of those who were aware of FP, only 401/671 (59.8%) were aware that some FP methods (e.g. IUCD and tubal ligation) could be started immediately after birth.
Table 2. FP awareness and uptake amongst postpartum women attending immunisation clinics in the OAUTHC.
Only one-fourth (184/715, 25.7%) and one-tenth (69/715, 9.7%) of the women had good knowledge of the side effects and mechanisms of actions of contraceptives, respectively. The majority (670/685, 97.8%) of respondents attended antenatal clinic during their last pregnancy. Amongst those who attended antenatal clinics, 105/658 (16.0%) did not receive FP education during antenatal clinic visits ().
More than one-third (278/715, 38.9%; 95% CI: 35.4–42.5%) of the women were not using any modern contraceptive currently. Of this number, 223/278 (80.2%) desired contraception to delay or space subsequent pregnancy. Most (165/223, 74.0%) of those who desired contraception intended to use condoms. A third preferred IUCD and implants (73/223, 32.7% each), more than a fourth (61/223, 27.4%), injectables, while more than a tenth (32/223, 14.3%) desired pills. Only 6/223, 2.7%, wanted tubal ligation, as shown in .
Of those who were currently using modern contraception (437/715, 61.1%; 95% CI: 57.5–64.6%), the predominant contraceptive method was condom (265/437, 60.6%), while tubal ligation was the least common method (4/437, 0.9%). Nearly one-tenth of the women used IUCD (40/437, 9.2%), injectables (33/437, 7.6%), pills (31/437, 7.1%), and implants (30/437, 6.9%).
On bivariate analysis, married status (p = 0.022), tertiary level of education (p = 0.043), resumption of sexual activity following last childbirth (p = <0.001) and past contraceptive use (p= <0.001) were significantly associated with current contraceptive use (kindly see supplementary material-Table S1). However, upon univariate logistic regression and after adjusting for covariates, only resumption of sexual intercourse following last childbirth and previous use of contraception showed significant associations with current contraceptive use among our study cohort (). The likelihood of currently using contraceptives among women who had resumed sexual intercourse following their last childbirth was four times the odds of current contraceptive use among women who had not resumed sexual intercourse (AOR = 4.16, 95% CI: 1.22–14.14; p = 0.022). Women who had a past history of contraceptive use had seven-fold odds of currently using contraceptive compared to women who had no previous history of contraceptive use (AOR = 7.38, 95% CI: 1.96–27.75; p = 0.003). The variance inflation factor of the variables in the final model were each <1.1, which suggests that there was no collinearity among the explanatory variables.
Table 3. Univariable and multivariable logistic regression of the relationship between sociodemographic and sexual characteristics, history of antenatal care, previous contraceptive use and current use of contraceptive.
Most of the women (552/715, 77.2%) felt very comfortable discussing FP with staff at the infant immunisation clinics.
Effects of integration of PPFP education with infant vaccination visits in the OAUTHC
Following successful integration of PPFP education with infant vaccination visits in our study sites, the number of women who had good knowledge of the side effects and mechanisms of actions of contraceptives significantly increased from 184/715 (25.7%) and 69/715 (9.7%), respectively, to 248/715, 34.7% (p = 0.001), and 104/715, 14.5% (p = 0.003), respectively. Intention to use contraception within 12 months increased from 223/715 (31.2%) to 273/715 (38.2%), p = 0.001.
In the six months preceding our study, total client load at the FP clinics in our three study sites was 3,338, of which new acceptors were 487. In the six months following successful integration of PPFP education with infant vaccination visits, total client load at the FP clinics increased to 3,808 (p = 0.157). New acceptors increased significantly by 36.3%, from 487 to 664 (p = 0.001).
Discussion
Most women in our study were young, married, with tertiary level of education, and multiparous. Even though majority of the women in our study had resumed sexual activity and wanted to have another baby, but desired contraception to postpone another pregnancy for at least 24 months, 31.2% of them were not using any modern contraception. With an unmet need for spacing of 31.2%, the uptake of PPFP in this study was not commensurate with the high level of awareness and exposure to FP education. This underscores the fact that unmet need for FP is higher 0–12 months postpartum than at any other time (Pasha et al. Citation2015). National FP programs in many developing countries often neglect women in the postpartum period (Pasha et al. Citation2015).
Amongst women who volunteered reasons for not adopting PPFP, the most common reason was non-consent by their husbands. In mostly patriarchal low-resource settings like ours, men determine to a very great extent, women’s access to, consent for, and utilisation of healthcare services, including FP (Mersha Citation2018). Incorporating men as FP champions at community level, would therefore, significantly increase uptake of PPFP. Other reasons included inaccurate knowledge about side effects of contraceptives, and misconceptions that conception is impossible while breastfeeding or before resumption of menses, and that contraception will make subsequent pregnancy difficult. These have similarly been reported by other authors (Adeyemi et al. Citation2005). These misconceptions are against the backdrop of our study findings that whereas more than 80% of the women who had antenatal care in their last pregnancy were educated on FP, only about 10%, 26% and 60% had good knowledge of the mechanisms of actions of contraceptives, side effects of contraceptives, and were aware that PPFP could be started immediate postpartum, respectively. This calls to question the quality of information provided during the FP education sessions at these antenatal clinics. The Quality of FP education/counselling and clarification of misconceptions correlate with contraceptive uptake and continuation amongst women (Dey et al. Citation2021). Several studies have reported deficient knowledge of contraception amongst FP providers (Dehlendorf et al. Citation2010). None of the FP providers interviewed in our study had had a recent training on FP. The lack of, or incomplete knowledge of evidence-based information on contraceptive methods impairs the ability of providers to provide accurate and up-to-date contraceptive information to their clients, which consequently negatively impacts the uptake of, and continuation of contraception by the clients (Dehlendorf et al. Citation2010).
The need for regular training and retraining of FP providers, to constantly update their knowledge of quality and evidence-based contraceptive information and guidelines, including the WHO medical eligibility criteria (World Health Organisation Citation2015), cannot be over-emphasized. This was evident in our study, as the knowledge of side effects, mechanisms of actions of contraceptives, as well as intention to use FP amongst the postpartum women significantly increased after they were provided additional FP education by trained FP providers in the vaccination clinics. As also found in our study, hospital/health workers are the main sources of information about FP (Galle et al. Citation2018). Family planning education and counselling are typically provided by healthcare workers in FP and antenatal clinics (Pasha et al. Citation2015, Galle et al. Citation2018).
Our study found a significant association between past contraceptive use and resumption of sexual activity following last childbirth and current use of contraception. Sok et al similarly observed that women who reported using contraception at six weeks postpartum were 1.8 times more likely to have resumed sexual intercourse by six weeks postpartum compared to women who were not using contraception then (Sok et al. Citation2016)
Many women in low-resource settings (LRS) do not receive antenatal care, owing to patronage of unorthodox faith-based delivery units and traditional birth attendants, fuelled by poverty, ignorance, religious and superstitious beliefs, amongst others (Ubom et al. Citation2021). In addition, FP education is infrequently offered in antenatal clinics in many LRS because these clinics are often very busy and short-staffed (Anya et al. Citation2008). Sixteen percent of the women in our study did not receive any form of FP education throughout their last pregnancy, even though they received antenatal care. Offering FP education and counselling services in infant vaccination clinics provides an ample window of opportunity to reach out to women who did not benefit from these services during the antenatal period. Following integration of FP education with infant vaccination visits, a significant increase in the number of new acceptors and total client load was recorded in the FP clinics in our study.
The findings from our study provide more evidence on the potential benefits of integrating PPFP with infant vaccination, and other maternal and child health services/programs (WHO Citation2013, Dulli et al. Citation2016). Integrating PPFP with infant immunisation services may potentially reduce the unmet need for FP, as well as maternal and childhood mortality and morbidity from unintended pregnancies, unsafe abortions and inadequate birth spacing. To better improve the uptake of PPFP, PPFP education should be initiated from the antenatal care period. Future research should explore the benefits of integrating both PPFP education and delivery with infant vaccination visits on the uptake of PPFP. In our study, three-fourth of non-current contraceptive users desired to use condoms, which can easily be provided in an outpatient vaccination clinic scenario.
Limitations of the study
It was difficult to determine whether the observed increase in client load at our FP clinics following integration of FP education with infant vaccination visits was due to increased patronage from the study participants and not from other clients who were not part of the study, as the latter were not distinguished from the former in this pilot study. This limitation has been factored in in the design of the scale-up. In the scale-up, clients from the immunisation clinics will be given special referral cards so that the FP clinic staff can distinguish them from other clients, such that their records will be accounted for among the new acceptors of FP.
Another limitation of the study is the difficulty with harmonising the unmet need for FP with the time interval from delivery, as different FP methods have various time intervals that they can be commenced following delivery. The design of the scale-up study will include information on the time interval from delivery to commencement of FP for women on FP, as well as the time interval from delivery for women not on FP.
Conclusion
Integrating postpartum FP education and infant vaccination services is a feasible and acceptable strategy for increasing contraceptive use among postpartum women. Wider implementation of this strategy is desirable because it improved FP knowledge and PPFP uptake.
Supplemental Material
Download MS Word (18.3 KB)Acknowledgements
OI was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand. The statements made and views expressed are solely the responsibility of the Fellow. IT was supported by TEPHINET/CDC Research Grant for Non-Communicable diseases. The authors appreciate Dr Gbenga Olorunfemi, MBBS, MSc, FWACS, FMCOG, Division of Epidemiology and Biostatistics, University of Witwatersrand, South Africa, for the statistical analysis of the revised manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Adeyemi, A.B., et al., 2005. The unmet need for contraception among Nigerian women in the first year post-partum. The European Journal of Contraception & Reproductive Health Care, 10 (4), 229–234.
- Anya, S.E., Hydara, A. and Jaiteh, L.E., 2008. Antenatal care in The Gambia: Missed opportunity for information, education and communication. BMC Pregnancy and Childbirth, 8 (1), 9–7.
- Cleland, J., et al., 2006. Family planning: the unfinished agenda. Lancet, 368 (9549), 1810–1827.
- Conde-Agudelo, A., et al., 2012. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms. Studies in Family Planning, 43 (2), 93–114.
- Cooper, C.M., et al., 2015. Successful proof of concept of family planning and immunization integration in Liberia. Global Health, Science and Practice, 3 (1), 71–84.
- Cooper, C.M., et al., 2020. Integrated family planning and immunization service delivery at health facility and community sites in Dowa and Ntchisi Districts of Malawi: A Mixed Methods Process Evaluation. International Journal of Environmental Research and Public Health., 17 (12), 4530.
- DaVanzo, J., et al., 2007. Effects of interpregnancy interval and outcome of the preceding pregnancy on pregnancy outcomes in Matlab, Bangladesh. BJOG : An International Journal of Obstetrics and Gynaecology, 114 (9), 1079–1087.
- Dehlendorf, C., et al., 2010. Health care providers’ knowledge about contraceptive evidence: a barrier to quality family planning care? Contraception, 81 (4), 292–298.
- Dey, A.K., et al., 2021. Measuring quality of family planning counselling and its effects on uptake of contraceptives in public health facilities in Uttar Pradesh, India: A cross-sectional analysis. PLoS One, 16 (5), e0239565.
- Dulli, L.S., et al., 2016. Meeting postpartum women’s family planning needs through integrated family planning and immunization services: results of a cluster-randomized controlled trial in Rwanda. Global Health, Science and Practice, 4 (1), 73–86. 2016,
- Dworkin, S.L., 2012. Sample size policy for qualitative studies using in-depth interviews. Archives of Sexual Behavior, 41 (6), 1319–1320.
- FHI 360 2010. Integration of family planning with immunization services: A promising approach to improving maternal and child health. https://www.fhi360.org/sites/default/files/media/documents/integration-family-planning-immunization.pdf
- Galle, A., et al., 2018. Quality of care in family planning services in rural Mozambique with a focus on long acting reversible contraceptives: a cross sectional survey. BMC Women’s Health, 18 (1), 1–3.
- Gross, B.A. and Burger, H, WHO Task Force on methods for the natural regulation of fertility 2002. Breastfeeding patterns and return to fertility in Australian women. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 42 (2), 148–154.
- Hounton, S., et al., 2015. Patterns and trends of postpartum family planning in Ethiopia, Malawi, and Nigeria: evidence of missed opportunities for integration. Global Health Action, 8 (1), 29738.
- Jackson, E. and Glasier, A., 2011. Return of ovulation and menses in postpartum nonlactating women: a systematic review. Obstetrics and Gynecology, 117 (3), 657–662.
- Mackenzie, D., et al., 2018. Postpartum family planning integration with maternal, newborn and child health services: a cross-sectional analysis of client flow patterns in India and Kenya. BMJ Open, 8 (4), e018580.
- Mersha, A.G., 2018. Male involvement in the maternal health care system: implication towards decreasing the high burden of maternal mortality. BMC Pregnancy and Childbirth, 18 (1), 493.
- National Population Commission [Nigeria] and ICF International 2019. Nigeria demographic and health survey 2018. Abuja, Nigeria, and Rockville, MD: NPC and ICF.
- Nelson, A.R., et al., 2019. Operationalizing integrated immunization and family planning services in rural Liberia: lessons learned from evaluating service quality and utilization. Global Health, Science and Practice, 7 (3), 418–434.
- Pasha, O., et al., 2015. Postpartum contraceptive use and unmet need for family planning in five low-income countries. Reproductive Health, 12 (2), S11.
- Pfitzer, A., et al., 2015. A facility birth can be the time to start family planning: Postpartum intrauterine device experiences from six countries. International Journal of Gynecology & Obstetrics, 130 (S2), S54–S61.
- Ringheim, K., Gribble, J. and Foreman, M., 2011. Integrating family planning and maternal and child health care: saving lives, money, and time. Policy Brief. Population Reference Bureau. https://u.demog.berkeley.edu/∼jrw/Biblio/Eprints/PRB/files/familyplanning-maternal-child-health.pdf
- Ross, J.A. and Winfrey, W.L., 2001. Contraceptive use, intention to use and unmet needs during the extended postpartum period. International Perspectives on Sexual and Reproductive Health, 27 (1), 20–27.
- Sok, C., et al., 2016. Sexual behaviour, satisfaction, and contraceptive use among postpartum women. Journal of Midwifery & Women’s Health, 61 (2), 158–165.
- Ubom, A.E., et al., 2021. Obstructed labour in a Nigerian tertiary health facility: a mixed method study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 10 (8), 2937–2943.
- World Health Organisation 2015. Medical eligibility criteria for contraceptive use. 5th ed. Geneva: WHO.
- World Health Organization, 2013. Programming strategies for postpartum family planning. Geneva: WHO. https://apps.who.int/iris/bitstream/handle/10665/93680/9789241506496_eng.pdf